Orthopedic Prometric MCQs - Chapter 3 Part 17
Orthopedic Prometric MCQs - Chapter 3 Part 17
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The radiographs (Slide) of a 13-year-old-boy are presented. The radiographs demonstrate characteristics of which of the following conditions:
Explanation
Question 2
An 11½ -year-old boy sustained a Salter IV fracture of the distal tibial physis. The fracture was treated in a cast. Two years later, his radiographs (Slide) are presented. The patient is starting to notice a deformity. Which of the following treatment plans is recommended:
Explanation

Question 3
The radiographs (Slide) indicate which of the following diagnoses:
Explanation
 these fractures so that the patient and family may be given proper activity restrictions and expectations for improvement.
these fractures so that the patient and family may be given proper activity restrictions and expectations for improvement.
Question 4
A 5-year-old boy was imaged after being struck by a car. His radiographs (Slide) indicate which of the following diagnoses:
Explanation
 When seen in some projections, the more distal extent of the physis may produce a lucent line. The smooth nature and characteristic location of the line should allow surgeons to make the correct interpretation. The two ossification centers of the humeral head may be misinterpreted as a fracture. This patient had a greenstick fracture of the clavicle (not included on this field), which was not noticed, and a humeral fracture was incorrectly diagnosised.
When seen in some projections, the more distal extent of the physis may produce a lucent line. The smooth nature and characteristic location of the line should allow surgeons to make the correct interpretation. The two ossification centers of the humeral head may be misinterpreted as a fracture. This patient had a greenstick fracture of the clavicle (not included on this field), which was not noticed, and a humeral fracture was incorrectly diagnosised.
Question 5
The largest available free muscle flap comes from which of the following muscles:
Explanation
Question 6
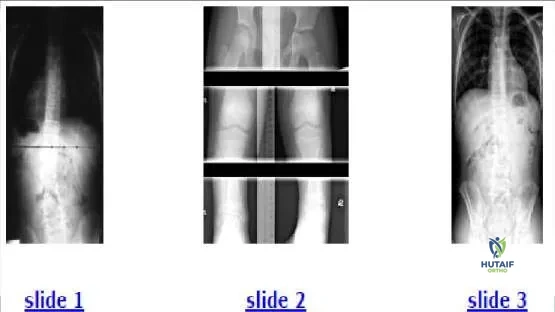
A 12-year-old boy presents for evaluation of a spinal curvature (Slide 1). Which of the following is the most likely cause of the spinal curve:
Explanation
Question 7
In the embryo, cells from the ectodermal layer give rise to which elements of the spine:
Explanation
nucleus pulposus. The mesoderm gives rise to muscles and bony elements of the spinal column.
Question 8
How many somites are involved in formation of each vertebral body of the thoracolumbar spine:
Explanation
Question 9
A 6-year-old boy sustains a supracondylar fracture of the humerus. The 2 fragments are not completely displaced, but there is some overlap of the medial column and a gap on the lateral column of the distal humerus. Baumannâ s angle measures 85°. The alignment on the lateral film shows no significant translation, but approximately 15° of increased extension. The recommended treatment is:
Explanation
Question 10
The 7-year-old patient shown in this image (Slide 1) is most likely presenting with:
Explanation
Question 11
Which of the following treatment options is recommended for the patient shown in the image (Slide 1, Slide 2):
Explanation
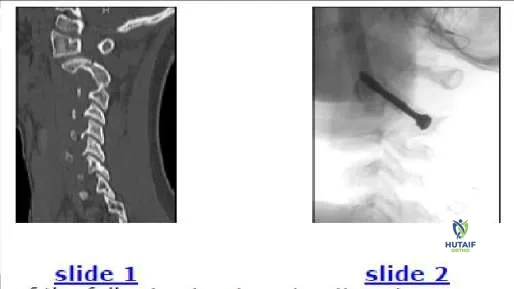 on the arch of C 2. If facet subluxation is not present, then a cervicothoracic orthosis such as a Philadelphia collar is adequate for healing of the C 2 spondylolysis.
on the arch of C 2. If facet subluxation is not present, then a cervicothoracic orthosis such as a Philadelphia collar is adequate for healing of the C 2 spondylolysis.
Question 12
Flexion-type supracondylar fractures of the distal humerus in children are characterized by which of the following when compared to extension-type injuries:
Explanation
Question 13
The 12-year-old boy shown in the radiographs (Slide 1, Slide 2) sustained his injury during a motor vehicle accident. Which of the following most accurately describes the injury:
Explanation
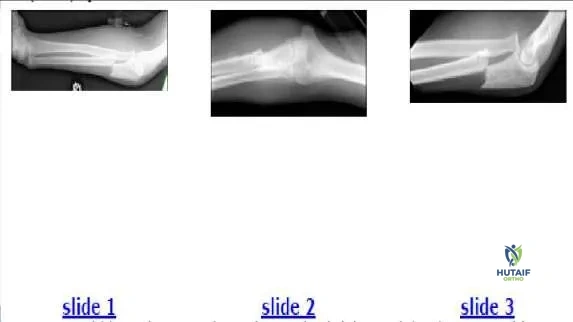 radial head does not articulate with the capitellum. On the anteroposterior film, the radial head points to the capitellum, but the joint space is absent in contrast to that of the ulna-trochlear joint, which is normal. This injury is a type 1 (anterior) Monteggia fracture. The dislocation is clearly visible on Slide 3. A Galeazzi fracture refers to a distal radioulnar dislocation with a radial fracture. A Maisonneuve fracture is a related concept in the lower extremity: a proximal fibular fracture with an ankle mortise injury.
radial head does not articulate with the capitellum. On the anteroposterior film, the radial head points to the capitellum, but the joint space is absent in contrast to that of the ulna-trochlear joint, which is normal. This injury is a type 1 (anterior) Monteggia fracture. The dislocation is clearly visible on Slide 3. A Galeazzi fracture refers to a distal radioulnar dislocation with a radial fracture. A Maisonneuve fracture is a related concept in the lower extremity: a proximal fibular fracture with an ankle mortise injury.
Question 14
A 12-year-old boy sustained the injury shown (Slide 1, Slide 2, and Slide 3). A postreduction film is also presented (Slide 4). Which of the following treatments is the most likely to produce satisfactory results:

Explanation
Question 15
A 7-year-old boy is intubated after being involved in a motor vehicle accident. His lateral cervical film (Slide 1) reveals a:
Explanation
Question 16
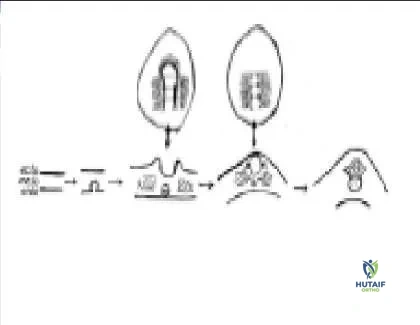
The images presented (Slide 1, Slide 2) depict which process:
Explanation
Question 17
Patients who have had a unilateral slipped capital femoral epiphysis (SC FE) are at what odds of a contralateral slip compared to the general population:
Explanation
Question 18
Which of the following conditions is represented in the clinical photographs (Slide 1, Slide 2):
Explanation
Question 19
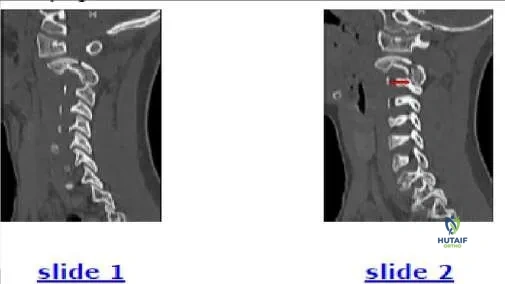
A 6-year-old child is involved in a motor vehicle accident. What injury is demonstrated by the computed tomography (C T) (Slide
Explanation
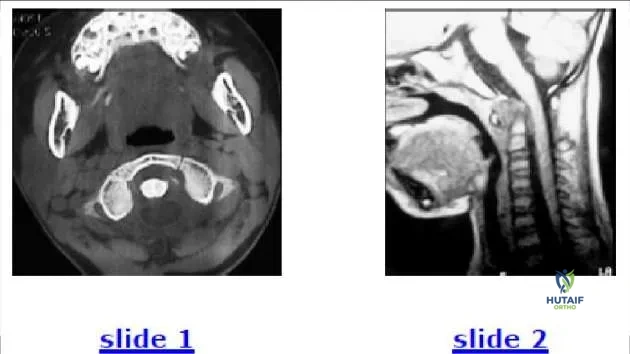 odontoid injury, the odontoid would still have a normal relationship to the ring of C 1 on the C T. Treatment involves reduction and fusion of C 1-C 2.
odontoid injury, the odontoid would still have a normal relationship to the ring of C 1 on the C T. Treatment involves reduction and fusion of C 1-C 2.
Question 20
The radiograph (Slide 1) of an 11-year-old boy with significant leg pain is presented. No other abnormalities are found during the patientâ s history or physical examination. The most likely diagnosis is:
Explanation
Question 21
A 4-week-old infant is treated with a Pavlik harness for developmental dysplasia of the hip. At a follow-up visit, the infant is noted to have decreased spontaneous movement of the knee and absent knee extension against gravity. What is the most likely iatrogenic cause?
Explanation
Question 22
An obese 12-year-old boy presents with a 3-week history of knee pain and a limp. He sits with his affected leg externally rotated. Radiographs reveal a widened and irregular proximal femoral physis. What is the most appropriate initial management?
Explanation
Question 23
A 9-year-old boy sustained a distal femoral physeal fracture 1 year ago. He now presents with a valgus deformity.
Based on the likelihood of a localized physeal bar, what percentage of physeal involvement is generally considered the upper limit for successful bar resection?
Explanation
Question 24
A 6-year-old boy presents with a painless limp. Radiographs demonstrate sclerosis and fragmentation of the proximal femoral epiphysis. Which of the following factors carries the worst prognosis for this condition?
Explanation
Question 25
A 5-year-old child sustains a displaced extension-type supracondylar humerus fracture. Examination reveals weakness in flexing the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve is most likely injured?
Explanation
Question 26
A 13-year-old boy presents with recurrent ankle sprains and rigid flat feet. CT scan confirms a calcaneonavicular coalition. If conservative management fails, what is the surgical treatment of choice for a coalition comprising less than 50% of the joint space with no degenerative changes?
Explanation
Question 27
A 3-year-old girl presents with progressive bilateral genu varum. Radiographs show a prominent metaphyseal beak and a metaphyseal-diaphyseal angle of 18 degrees. What is the recommended treatment?
Explanation
Question 28
A newborn is noted to have a foreshortened right forearm with the hand deviated radially and an absent thumb. Which of the following systemic conditions is NOT typically associated with this deformity?
Explanation
Question 29
When correcting a congenital idiopathic clubfoot using the Ponseti method, what is the correct sequence of deformity correction?
Explanation
Question 30
A 10-year-old boy falls from a tree. Radiographs reveal a fracture extending through the physis and exiting through the metaphysis of the distal radius.
What is the Salter-Harris classification of this fracture?
Explanation
Question 31
A 12-year-old premenarchal female (Risser 0) is diagnosed with adolescent idiopathic scoliosis. Her right thoracic curve measures 32 degrees. What is the most appropriate management?
Explanation
Question 32
A 4-year-old child sustains an isolated spiral fracture of the femoral shaft after a low-energy fall. Length is preserved with 1 cm of shortening. What is the standard of care for this injury?
Explanation
Question 33
A 2-year-old boy with blue sclerae presents with his third long bone fracture. Genetic testing reveals a defect in Type I collagen. Which medical treatment has been shown to reduce fracture rates and improve bone density in this condition?
Explanation
Question 34
A 14-year-old boy sustains an ankle injury. Radiographs and CT demonstrate a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. What is the anatomic reason for this specific fracture pattern?
Explanation
Question 35
A 15-year-old gymnast presents with chronic lower back pain. Radiographs demonstrate a grade II isthmic spondylolisthesis at L5-S1. She has failed 6 months of conservative management. What is the most appropriate surgical intervention?
Explanation
Question 36
A 6-year-old boy sustains a diaphyseal fracture of the proximal third of the ulna.
Which associated injury must be specifically evaluated for and excluded?

Explanation
Question 37
A 10-year-old girl is predicted to have a 3.5 cm leg length discrepancy at skeletal maturity, with the right leg being shorter. She and her parents desire a minimal surgical intervention. What is the most appropriate management?
Explanation
Question 38
A 5-year-old child with spastic quadriplegic cerebral palsy is undergoing routine hip surveillance. Radiographs show a migration percentage of 45% with a break in Shenton's line. What is the most appropriate management?
Explanation
Question 39
A 2-year-old boy is brought to the clinic because he refuses to bear weight on his left leg. Examination reveals minimal swelling and tenderness over the distal tibia. Initial radiographs are completely normal. What is the most appropriate next step?
Explanation
Question 40
A 9-year-old boy sustains a pathologic fracture through a centrally located, purely lytic lesion in the proximal humerus metaphysis.
A "fallen leaf" sign is noted. What is the definitive treatment after the fracture has healed if the lesion persists?

Explanation
Question 41
A 12-year-old obese boy presents with a 3-week history of left groin pain and a limp. On examination, as the left hip is flexed, it obligatorily externally rotates. Radiographs are shown.
What is the most appropriate definitive management?
Explanation
Question 42
A 6-year-old boy presents with a painless limp of 2 months' duration. His hip range of motion reveals decreased abduction and internal rotation. A radiograph reveals sclerosis and fragmentation of the proximal femoral epiphysis. What is the most likely diagnosis?
Explanation
Question 43
A 14-year-old boy presents with anterior knee pain exacerbating with jumping. Examination reveals tenderness over the tibial tubercle. Radiographs demonstrate fragmentation of the tibial apophysis.
Which of the following is the most appropriate initial management?
Explanation
Question 44
A 4-week-old female infant is brought to the clinic for a routine check-up. Barlow and Ortolani maneuvers are positive on the left side. Ultrasound confirms developmental dysplasia of the hip (DDH). What is the initial treatment of choice?
Explanation
Question 45
A 3-year-old child presents with a severe bowleg deformity (varus) that has progressed over the past year. Radiographs show medial beaking and fragmentation of the proximal tibial metaphysis.
What is the most likely diagnosis?
Explanation
Question 46
A 7-year-old boy falls on an outstretched hand and sustains a widely displaced extension-type supracondylar fracture of the humerus. During assessment, he is unable to flex the interphalangeal joint of his thumb. Which nerve is most likely injured?
Explanation
Question 47
An infant is born with a rigid equinovarus deformity of the right foot. When applying the Ponseti method of serial casting, which component of the deformity is corrected first?
Explanation
Question 48
A 14-year-old gymnast presents with chronic low back pain exacerbated by extension. Radiographs and an MRI confirm a bilateral pars interarticularis defect at L5 without spondylolisthesis. What is the most appropriate initial management?
Explanation
Question 49
A 13-year-old boy sustains an ankle injury. Radiographs show a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis.
What ligament is responsible for the avulsion of this fracture fragment?
Explanation
Question 50
A 15-year-old male complains of a painful, stiff flatfoot. Symptoms are worse when walking on uneven ground. Radiographs reveal a "C sign" on the lateral view. What is the most likely diagnosis?
Explanation
Question 51
A 10-year-old boy presents with thigh pain that is worse at night and relieved dramatically by ibuprofen. Radiographs demonstrate a small radiolucent nidus surrounded by dense reactive sclerosis in the proximal femur.
What is the preferred definitive treatment if symptoms are refractory to medical management?
Explanation
Question 52
A 9-year-old boy sustains a minor fall and presents with arm pain. Radiographs reveal a mildly displaced pathologic fracture through a central, radiolucent, well-circumscribed lesion in the proximal humerus with a "fallen leaf" sign. What is the most likely diagnosis?
Explanation
Question 53
A 2-year-old child presents with a sudden onset of refusal to use the right arm after being pulled by the wrist. The arm is held in extension and pronation. Radiographs are normal. What is the most appropriate management?
Explanation
Question 54
A 16-year-old boy presents with intermittent knee catching and pain. MRI reveals an unstable osteochondral fragment in the knee joint.
What is the most common location for osteochondritis dissecans in the knee?
Explanation
Question 55
A 5-year-old boy presents with anterior bowing of his tibia and a leg length discrepancy. Radiographs reveal a pseudarthrosis of the middle third of the tibia.
This condition is most strongly associated with which of the following systemic disorders?
Explanation
Question 56
A 6-month-old infant is diagnosed with an atypical presentation of multiple fractures in various stages of healing, blue sclerae, and dentinogenesis imperfecta. A genetic defect in which of the following is most likely responsible?
Explanation
Question 57
A 14-year-old pitcher presents with progressive shoulder pain during throwing. Radiographs reveal widening of the proximal humeral physis compared to the contralateral side.
What is the best initial treatment?
Explanation
Question 58
A 12-year-old girl is diagnosed with adolescent idiopathic scoliosis (AIS). She is premenarchal, Risser stage 0, and has a right thoracic curve of 35 degrees. What is the most appropriate management?
Explanation
Question 59
A 10-year-old child presents with a spiral fracture of the distal third of the tibia and an intact fibula. Over the next few weeks, what complication should be closely monitored regarding the varus/valgus alignment?
Explanation
Question 60
An 8-year-old boy presents with a persistent limp. Radiographs demonstrate a fragmented proximal femoral epiphysis.
Which of the following factors is most predictive of the final radiographic outcome in Legg-Calvé-Perthes disease?
Explanation
Question 61
A 14-year-old boy sustains a twisting ankle injury. Radiographs show a classic triplane fracture.
Which of the following accurately describes the typical fracture pattern seen on standard anteroposterior (AP) and lateral radiographic views?
Explanation
Question 62
A 13-year-old boy presents with an isolated juvenile Tillaux fracture of the ankle. Which of the following best explains the specific anatomical pathogenesis of this fracture pattern?
Explanation
Question 63
An 8-month-old girl presents with developmental dysplasia of the hip (DDH) that has failed Pavlik harness treatment. A closed reduction and spica casting is planned. Which of the following is considered the most significant extra-articular block to closed reduction in this age group?
Explanation
Question 64
A 6-year-old boy presents with a displaced extension-type supracondylar humerus fracture. After anatomic closed reduction and percutaneous pinning, the radial pulse is absent, but the hand remains warm and pink with brisk capillary refill. What is the most appropriate next step in management?
Explanation
Question 65
When correcting a severe congenital idiopathic clubfoot using the Ponseti method, what is the correct physiological sequence of deformity correction during serial casting?
Explanation
Question 66
A 12-year-old obese boy presents with right knee pain and an antalgic gait. Hip radiographs
show a stable slipped capital femoral epiphysis (SCFE). He is treated with a single in-situ screw. What is the most common long-term complication of his underlying condition?
Explanation
Question 67
A radiograph
of a 10-year-old girl who sustained a lateral condyle fracture of the humerus 5 years ago shows an established nonunion. She now complains of clumsiness in her hand and numbness in her little finger. This complication is most directly related to:
Explanation
Question 68
A 4-year-old boy with spastic diplegic cerebral palsy undergoes routine radiographic screening of his hips. The Reimers migration percentage is calculated to be 45%. What does this value indicate, and what is the generally recommended orthopedic management?
Explanation
Question 69
A 9-year-old boy sustained a fracture to his distal radius physis. One year later, radiographs
reveal a central physeal bar occupying 25% of the cross-sectional area. He has an estimated 3 cm of growth remaining. What is the most appropriate surgical treatment?
Explanation
Question 70
A 15-year-old boy complains of vague, chronic ankle pain and a history of frequent sprains. Clinical examination reveals a rigid flatfoot. Lateral radiographs demonstrate a positive 'C-sign'. Which of the following is the most likely diagnosis?
Explanation
Question 71
An 18-month-old boy is brought to the clinic with severe bowing of the legs. Radiographs
show an abrupt varus angulation at the proximal medial tibia with a distinct metaphyseal beak. He is diagnosed with infantile Blount's disease. Which of the following Langenskiöld stages denotes the formation of a bony bar across the physis, making spontaneous resolution highly unlikely?
Explanation
Question 72
A 13-year-old gymnast presents with acute medial elbow pain after a fall. Radiographs demonstrate a displaced medial epicondyle fracture. Which of the following is universally considered an absolute indication for open reduction and internal fixation?
Explanation
Question 73
A 12-year-old boy presents with right ankle pain after a severe inversion and external rotation injury. Radiographs show a Salter-Harris III fracture of the anterolateral distal tibial epiphysis.
What is the most likely diagnosis?
Explanation
Question 74
A 14-year-old boy sustains a distal femur Salter-Harris II fracture following a football tackle. Which of the following is the most common significant complication associated with this specific injury pattern at this location?
Explanation
Question 75
A 6-year-old boy presents with a painless limp of 3 months' duration. Radiographs demonstrate sclerosis and fragmentation of the femoral head.
Measurement reveals the lateral pillar height is 60% of normal. What is the appropriate Herring classification?
Explanation
Question 76
An 18-month-old presents with unilateral in-toeing. Physical examination reveals a rigid medial deviation of the forefoot with a completely normal, flexible hindfoot. What is the most likely diagnosis?
Explanation
Question 77
A 13-year-old obese boy presents with right knee pain and a limp. On examination, obligate external rotation of the right hip is noted during passive flexion.
What is the most appropriate initial treatment?
Explanation
Question 78
A newborn is diagnosed with severe idiopathic clubfoot. The pediatric orthopedic surgeon begins treatment using the Ponseti method. According to this protocol, which deformity must be corrected first?
Explanation
Question 79
A 5-year-old child presents with a 'pink, pulseless' hand after a severely displaced extension-type supracondylar humerus fracture. After prompt closed reduction and percutaneous pinning, the hand remains well-perfused (pink) but the radial pulse is still non-palpable. What is the next best step in management?
Explanation
Question 80
A 4-year-old girl is evaluated for a persistent limp. Radiographs demonstrate late-presenting developmental dysplasia of the hip (DDH) with a fully dislocated femoral head.
What is the most appropriate definitive management?
Explanation
Question 81
A pediatric patient presents with anterolateral bowing of the tibia that progresses to a spontaneous fracture. Which of the following systemic conditions is most strongly associated with this finding?
Explanation
Question 82
A 9-year-old boy presents with shoulder pain after a minor fall. Radiographs reveal a centrally located, radiolucent metaphyseal lesion in the proximal humerus with a cortical fragment resting at the bottom of the cyst. What is the most likely diagnosis?
Explanation
Question 83
A 12-year-old competitive gymnast complains of chronic, bilateral dorsal wrist pain. Radiographs reveal widening of the distal radial physis and cystic changes.
What is the most appropriate initial management?
Explanation
Question 84
A 2-year-old presents with a fever of 39.0°C, inability to bear weight on the right leg, an ESR of 50 mm/hr, and a serum WBC of 13,000/mm3. According to Kocher's criteria, what is the probability that this child has septic arthritis of the hip?
Explanation
Question 85
A 5-year-old boy sustains a lateral condyle fracture of the distal humerus. Initial radiographs show 3 mm of displacement.
What is the most appropriate management?
Explanation
Question 86
A 13-year-old baseball pitcher presents with acute medial elbow pain after throwing a pitch. Radiographs show an avulsion fracture of the medial epicondyle. What is the primary mechanism of injury?
Explanation
Question 87
A 7-year-old is undergoing evaluation for a suspected physeal bar across the distal femur following a previous fracture.
Which imaging modality is considered the gold standard to accurately map the size, geometry, and location of the bar?
Explanation
Question 88
When considering the surgical resection of a post-traumatic physeal bar, what is the generally accepted maximum percentage of cross-sectional physeal area involvement that still permits successful resection?
Explanation
Question 89
A 14-year-old adolescent presents with a rigid flatfoot, hindfoot valgus, and frequent ankle sprains. CT scan shows a solid bony bridge between the middle facet of the talus and the calcaneus.
What is the most likely diagnosis?
Explanation
Question 90
A 1-month-old infant is being treated with a Pavlik harness for developmental dysplasia of the hip. The parents report the infant has stopped spontaneously kicking the affected leg. Ultrasound confirms the hip remains reduced. What iatrogenic complication has most likely occurred?
Explanation
None
