Orthopedic Prometric MCQs - Chapter 3 Part 26

Orthopedic Prometric MCQs - Chapter 3 Part 26
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
How common are spinal infections following penetrating injury to the spine:
Explanation
Question 2
Risk factors implicated in postoperative wound infection following lumbar spine surgery include all of the following except:
Explanation
Question 3
In the face of vertebral infection and progressive deformity, surgical reconstruction should:
Explanation
Question 4
The spinal surgical procedure associated with the highest rate of surgical site infection is:
Explanation
Question 5
Which of the following comprises the middle column in the Denis three- column model of the thoracolumbar spine:
Explanation
Question 6
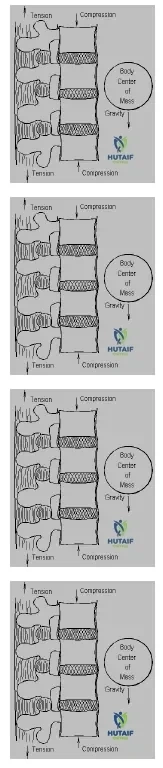
Which type of biomechanical force(s) acts on the anterior portion of the thoracolumbar junction (T12-L2) at rest in a standing position:
Explanation
osteoligamentous structures are subject to tension along with the paraspinous muscles that help to maintain an upright posture.
Question 7
Which of the following statements is true regarding the bulbocavernosus reflex:
Explanation
Question 8
According to the Frankel grading scale for a neurologic injury, what is meant by Frankel C :
Explanation
Question 9
Which type of thoracolumbar fracture is associated with the highest incidence of intra-abdominal visceral trauma:
Explanation
Question 10
Which type of treatment would be most appropriate for a young, healthy patient with an incomplete spinal cord injury (ASIA C ) 5 days following a T12 burst fracture with 30% canal compromise:
Explanation
Question 11
Which of the following is the best indication for a laminectomy in a patient who has sustained a thoracolumbar burst fracture with a neurologic deficit:
Explanation
Question 12
Which recommendations for the pharmacologic treatment of spinal cord injuries resulted from the NASC IS-II trials:
Explanation
Question 13
Which of the following statements is true regarding neurogenic shock:
Explanation
Question 14
Which is the best indication for surgical treatment of a patient with a thoracolumbar burst fracture:
Explanation
Question 15
Which of the following patients is not at increased risk for isthmic spondylolisthesis:
Explanation
Question 16
Which patient is at the lowest risk for progression of spondylolisthesis:
Explanation
Question 17
What is the most common source of neurologic compression in a patient with lumbar spinal stenosis due to degenerative changes in the lumbar spine:
Explanation
Question 18
Which of the following cervical spine nerve roots may cause paralysis of the diaphragm if injured during an anterior approach:
Explanation
Question 19
The deltoid muscle may become paralyzed as a result of injury to which of the following cervical spine nerve roots:
Explanation
Question 20
The biceps reflex is diminished by compression of which of the following cervical spine nerve roots:
Explanation
Question 21
Which of the following is the most appropriate initial imaging modality of choice for a patient presenting with suspected pyogenic vertebral osteomyelitis who is hemodynamically stable and has no neurologic deficits?
Explanation
Question 22
A 45-year-old intravenous drug user presents with a 1-week history of severe back pain, high fever, and progressive bilateral lower extremity weakness. MRI confirms a large posterior spinal epidural abscess. What is the most appropriate definitive management?
Explanation
Question 23
In contrast to pyogenic vertebral osteomyelitis, spinal tuberculosis (Pott's disease) classically exhibits which of the following radiographic features during the early stages of the disease process?
Explanation
Question 24
A 60-year-old poorly controlled diabetic male undergoes an L4-L5 posterior spinal fusion. Three weeks postoperatively, he presents with increasing back pain, incisional erythema, and purulent wound drainage. The most commonly isolated organism in this clinical scenario is:
Explanation
Question 25
Which of the following clinical examination findings is most characteristic of a psoas abscess developing as a complication of lumbar vertebral osteomyelitis?
Explanation
Question 26
A 30-year-old male sustains a transcolonic gunshot wound to the abdomen, with the bullet lodging in the L3 vertebral body. He is neurologically intact. During exploratory laparotomy, bowel perforation is confirmed and repaired. What is the standard orthopedic management regarding the spinal injury?
Explanation
Question 27
Regarding spontaneous pediatric discitis, which of the following statements is most accurate?
Explanation
Question 28
A patient with established pyogenic vertebral osteomyelitis on MRI undergoes a CT-guided needle biopsy of the affected disc space, which returns negative for bacterial growth. What is the next most appropriate step in management if the patient remains hemodynamically stable but symptomatic?
Explanation
Question 29
Review the following clinical image.
In a patient presenting with severe back pain and elevated inflammatory markers, what are the classic MRI findings of pyogenic spondylodiscitis demonstrated on T1 and T2-weighted images?
Explanation
Question 30
Which of the following laboratory markers is considered the most sensitive and useful for monitoring the clinical response to antibiotic therapy in a patient being treated for pyogenic vertebral osteomyelitis?
Explanation
Question 31
A 40-year-old farmer from the Mediterranean region presents with chronic back pain, undulating fevers, and night sweats. MRI shows focal osteolysis with anterior endplate erosions in the lower lumbar spine, without massive disc destruction. What is the most likely etiology?
Explanation
Question 32
A 12-year-old boy with a known history of sickle cell anemia develops pyogenic vertebral osteomyelitis. While Staphylococcus aureus remains the most common overall cause, which of the following organisms is classically associated with this patient's underlying condition?
Explanation
Question 33
What is the classic clinical triad of symptoms associated with a spinal epidural abscess?
Explanation
Question 34
A 55-year-old patient presents with vague neck pain and a delayed, low-grade infection 6 months after a posterior cervical fusion. Intraoperative tissue cultures are initially negative but eventually become positive at 10 days. The most likely organism is:
Explanation
Question 35
In the surgical reconstruction of a patient with spinal tuberculosis presenting with a progressive neurologic deficit and a severe, rigid kyphosis of 50 degrees, which surgical approach generally provides the most direct and effective complete debridement?
Explanation
Question 36
In adult patients diagnosed with hematogenous pyogenic vertebral osteomyelitis, which region of the spine is most frequently affected?
Explanation
Question 37
Which of the following represents an absolute indication for surgical intervention in a patient with pyogenic vertebral osteomyelitis?
Explanation
Question 38
The "Pons sign," characterized by a step-like anterior erosion of the vertebral body seen on plain lateral radiographs or CT, is a classical finding highly suggestive of which infectious process?
Explanation
Question 39
A 70-year-old male on chronic hemodialysis for 15 years develops severe neck pain and destructive lesions at the C5-C6 level on MRI, resembling an infection. Biopsy is negative for infection but reveals beta2-microglobulin amyloid deposition. This condition is known as:
Explanation
Question 40
To minimize the risk of postoperative wound infection, prophylactic intravenous antibiotics for a routine, clean lumbar microdiscectomy should ideally be administered:
Explanation
Question 41
A 55-year-old male presents with severe back pain and fever. An MRI is obtained:
What is the most common organism responsible for the condition typically shown in such presentations?
Explanation
Question 42
Following an uncomplicated instrumented lumbar fusion, at what postoperative time frame does the C-reactive protein (CRP) typically peak before starting to return to baseline?
Explanation
Question 43
Which of the following MRI findings most strongly differentiates tuberculous spondylitis from pyogenic spondylodiscitis?
Explanation
Question 44
The classic clinical triad of a spinal epidural abscess includes back pain, fever, and which of the following?
Explanation
Question 45
In a patient with a known spinal epidural abscess, which of the following is an absolute indication for emergent surgical decompression?
Explanation
Question 46
A 45-year-old undergoes a microdiscectomy. Four weeks later, he presents with severe, excruciating back pain and paraspinal spasms. Inflammatory markers are significantly elevated. What is the most appropriate next step in management?
Explanation
Question 47
A 40-year-old farmer presents with chronic back pain, undulating fever, and profound fatigue. MRI shows L4-L5 discitis with an intact vertebral body architecture and minimal paraspinal soft tissue involvement. What is the most likely diagnosis?
Explanation
Question 48
A 3-year-old child presents with refusal to walk and irritability. Labs show a normal white blood cell count but mildly elevated ESR. Plain radiographs are normal. What is the most common pathogen responsible for this condition?
Explanation
Question 49
What is the most common route of bacterial spread leading to spontaneous pyogenic spondylodiscitis in adults?
Explanation
Question 50
A patient with thoracic tuberculous spondylitis presents with progressive kyphosis and myelopathy. Which surgical approach provides the most direct and effective decompression and reconstruction?
Explanation
Question 51
Which of the following patient factors is an independent and major risk factor for deep surgical site infection following instrumented spinal fusion?
Explanation
Question 52
A patient develops a deep wound infection 2 weeks after an instrumented posterior lumbar fusion. During surgical exploration, the hardware is found to be rigidly fixed. What is the standard management regarding the instrumentation?
Explanation
Question 53
Which spinal region is most frequently associated with postoperative infections caused by Cutibacterium acnes (formerly Propionibacterium acnes)?
Explanation
Question 54
A 12-year-old patient with sickle cell disease presents with spondylodiscitis. While S. aureus remains the most common overall, which organism is uniquely highly associated with osteomyelitis in this patient population?
Explanation
Question 55
A spine MRI of an immunocompromised patient with back pain reveals vertebral body destruction sparing the disc space, with multiple small paraspinal abscesses. Biopsy shows broad, non-septate hyphae with right-angle branching. What is the diagnosis?
Explanation
Question 56
A 50-year-old intravenous drug user presents with neck pain, fever, and rapidly progressive quadriparesis. MRI confirms a large ventral cervical epidural abscess. What is the preferred surgical intervention?
Explanation
Question 57
In a patient with uncomplicated tuberculous spondylitis without neurologic deficit or significant structural deformity, what is the recommended duration of multi-drug antituberculous therapy?
Explanation
Question 58
In suspected spontaneous pyogenic spondylodiscitis with negative blood cultures, what is the approximate diagnostic yield of a single CT-guided percutaneous needle biopsy?
Explanation
Question 59
Which of the following describes the normal postoperative kinetics of the Erythrocyte Sedimentation Rate (ESR) after an uncomplicated spinal fusion?
Explanation
Question 60
A patient sustains a gunshot wound to the abdomen with the bullet lodging in the L3 vertebral body, without neurologic deficit. There is a concurrent hollow viscus injury (colon perforation) being treated. What is the most appropriate management of the retained spinal bullet?
Explanation
Question 61
A 55-year-old diabetic male presents with severe lumbar back pain, fever, and progressive lower extremity weakness. MRI reveals a spinal epidural abscess. Which of the following is the most common causative organism?
Explanation
Question 62
In differentiating tuberculous spondylitis from pyogenic vertebral osteomyelitis on MRI, which of the following is most characteristic of tuberculosis?
Explanation
Question 63
A 65-year-old patient underwent a posterior lumbar interbody fusion. Three weeks postoperatively, he developed worsening back pain and low-grade fever.
Which inflammatory marker profile most strongly suggests a postoperative deep surgical site infection rather than normal postoperative changes?
Explanation
Question 64
An intravenous drug user presents with acute thoracic back pain, fevers, and new-onset lower extremity hyperreflexia. Blood cultures are pending. What is the most appropriate empiric antibiotic regimen pending cultures for a suspected spinal epidural abscess?
Explanation
Question 65
What is the primary arterial route of hematogenous spread of pyogenic infection to the adult vertebral body?
Explanation
Question 66
A 4-year-old child presents with refusal to walk and irritability when sitting up. There is no history of trauma. Temperature is 37.8 C. Plain radiographs of the spine are normal. What is the most appropriate next step in diagnosis?
Explanation
Question 67
When performing surgical debridement for an acute deep postoperative wound infection (within 2 weeks of surgery) following an instrumented posterolateral spinal fusion, what is the standard recommendation regarding the spinal instrumentation?
Explanation
Question 68
A 60-year-old man with confirmed pyogenic vertebral osteomyelitis has been on appropriate intravenous antibiotics for 4 weeks. His CRP has normalized, but he complains of persistent severe back pain and radiographs show progressive local kyphosis of 25 degrees. What is the most appropriate management?
Explanation
Question 69
Which of the following organism profiles is most frequently isolated in spinal infections associated with penetrating trauma (e.g., gunshot wounds) to the spine involving a trans-bowel trajectory?
Explanation
Question 70
Brucellosis of the spine can clinically mimic other granulomatous infections. Which of the following radiographic features is most characteristic of Brucella spondylitis?
Explanation
Question 71
A patient with suspected native pyogenic vertebral osteomyelitis is hemodynamically stable and neurologically intact. Blood cultures are negative. A CT-guided biopsy is scheduled. What is the correct approach to antibiotic therapy?
Explanation
Question 72
The classic triad of spontaneous spinal epidural abscess includes back pain, fever, and neurologic deficit. In what percentage of patients does this classic triad present initially?
Explanation
Question 73
According to the expected kinetics of inflammatory markers, when does the Erythrocyte Sedimentation Rate (ESR) typically peak following an uncomplicated lumbar decompression and fusion?
Explanation
Question 74
In children under the age of 5, what anatomical feature is primarily responsible for the pathophysiology of primary discitis, distinguishing it from adult vertebral osteomyelitis?
Explanation
Question 75
A 30-year-old immigrant presents with an 8-month history of middle back pain, weight loss, and progressive lower extremity weakness. Imaging shows severe thoracic kyphosis, destruction of T7 and T8 vertebral bodies, and a large calcified paraspinal abscess. What is the most appropriate surgical approach?
Explanation
Question 76
When evaluating a patient for vertebral osteomyelitis, MRI with gadolinium is the imaging modality of choice. What is the hallmark MRI finding of acute pyogenic spondylodiscitis?
Explanation
Question 77
Which of the following is considered an absolute indication for emergent surgical decompression in a patient with a spinal epidural abscess?
Explanation
Question 78
During a posterior lumbar fusion, an incidental dural tear occurs and is primarily repaired. Five days later, the patient develops a high fever, severe headache, and prominent photophobia. The wound is clean and intact. What is the most likely diagnosis?
Explanation
Question 79
A 70-year-old male with a history of recurrent urinary tract infections presents with severe back pain. MRI shows discitis-osteomyelitis at L3-L4. Blood cultures grow Escherichia coli. What is the most likely route of bacterial dissemination to the spine in this specific scenario?
Explanation
Question 80
For a hemodynamically stable patient with native pyogenic vertebral osteomyelitis successfully treated with targeted intravenous antibiotics and demonstrating a good clinical and laboratory response, what is the IDSA recommended total duration of antimicrobial therapy?
Explanation
Question 81
A 65-year-old male presents with severe back pain and elevated ESR 3 weeks after an uncomplicated microdiscectomy. MRI shows fluid in the disc space with endplate edema. What is the most appropriate initial management step prior to starting antibiotics?
Explanation
Question 82
Which of the following organisms is the most common cause of delayed, indolent post-operative deep wound infections following instrumented spinal fusions, frequently requiring up to 14 days of culture to identify?
Explanation
Question 83
A patient with pyogenic vertebral osteomyelitis presents with progressive bilateral lower extremity weakness and bowel incontinence. What is the most appropriate next step in management?
Explanation
Question 84
When comparing tuberculous spondylitis (Pott's disease) to pyogenic vertebral osteomyelitis on MRI, which of the following features is most characteristic of tuberculosis?
Explanation
Question 85
A 4-year-old child presents with refusal to walk, back pain, and low-grade fever. ESR is 45 mm/hr, and WBC is normal. MRI shows fluid in the L4-L5 disc space. Blood cultures are pending. What is the most common causative organism for this condition?
Explanation
Question 86
Review the clinical image. A 55-year-old diabetic male presents with insidious onset back pain and night sweats. MRI reveals endplate destruction and disc space enhancement.
Which laboratory marker is most useful for monitoring the resolution of this condition during antibiotic treatment?
Explanation
Question 87
A 24-year-old male suffers a gunshot wound to the abdomen with the bullet lodging in the L3 vertebral body. Exploratory laparotomy reveals a colon perforation. What is the most appropriate management regarding the bullet in the spine?
Explanation
Question 88
You are treating a patient with early postoperative deep wound infection following a posterior lumbar interbody fusion (PLIF) with pedicle screws. The implants are solidly fixed. Which of the following is the standard of care?
Explanation
Question 89
Which of the following scenarios is an absolute indication for surgery in a patient with spinal tuberculosis?
Explanation
Question 90
A 35-year-old IV drug user presents with fever, severe focal back pain, and radicular leg pain. Physical exam reveals exquisite point tenderness over the spinous processes. What is the classic clinical triad associated with the most likely diagnosis?
Explanation
Question 91
What is the recommended duration of intravenous (or highly bioavailable oral) antibiotic therapy for uncomplicated pyogenic vertebral osteomyelitis?
Explanation
Question 92
A patient with suspected pyogenic spondylodiscitis has two negative sets of blood cultures. The patient is hemodynamically stable without neurological deficits. What is the next best step?
Explanation
Question 93
Which of the following imaging modalities is the most sensitive and specific for diagnosing an early spinal epidural abscess?
Explanation
Question 94
A 50-year-old farmer from the Mediterranean region presents with chronic undulating fevers, sacroiliitis, and lumbar spondylitis. Radiographs show 'parrot beak' osteophytes and the disc space is relatively maintained. Which of the following tests would best confirm the likely diagnosis?
Explanation
Question 95
In adult patients with hematogenous pyogenic vertebral osteomyelitis, which region of the spine is most frequently affected?
Explanation
Question 96
A 60-year-old female presents with neck pain, fever, and progressive quadriparesis over 48 hours. MRI reveals an anterior cervical epidural abscess behind C4 and C5 with cord compression. What is the preferred surgical approach?
Explanation
Question 97
Which anatomical structure is primarily responsible for the spread of pelvic infections to the vertebral bodies, bypassing the systemic venous circulation?
Explanation
Question 98
A 70-year-old man on chronic hemodialysis presents with severe back pain. MRI shows discitis at L3-L4. Blood cultures grow methicillin-resistant Staphylococcus aureus (MRSA). He is treated with IV vancomycin. What is the most important factor in determining the appropriate dosing of his antibiotic therapy?
Explanation
Question 99
Which of the following patient populations is most at risk for developing fungal vertebral osteomyelitis, particularly with Aspergillus species?
Explanation
Question 100
A patient undergoes a posterior spinal fusion. 10 days postoperatively, the wound demonstrates purulent drainage. Debridement is performed. In addition to Staphylococcus aureus, which gram-negative organism is a common culprit in post-operative spinal infections, especially in cases with prolonged intensive care stays or urinary catheter use?
Explanation
None
