Orthopedic Prometric MCQs - Chapter 3 Part 24

Orthopedic Prometric MCQs - Chapter 3 Part 24
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 18-year-old man comes to the office with a grade IV isthmic spondylolisthesis and severe left lower extremity discomfort. Which imaging study would best help identify the site of potential nerve root compression:
Explanation
Question 2
Some of the more common risk factors that could predispose a person to developing low back pain are listed below. Which risk factor has not been implicated:
Explanation
Question 3
When considering surgical intervention in the management of low back pain, it is crucial to try and identify the possible offending agent or pain generator. Based on awake anatomical stimulation studies, what percentage of patients should report significant discomfort when a nerve root is either compressed or stretched in an attempt to elicit pain:
Explanation
Question 4
Which disorder does not represent a rheumatologic/inflammatory condition associated with causing low back pain:
Explanation
Question 5
A 57-year-old man with known lung cancer and metastatic disease complains of increasing low back pain. How often is the lumbar spine involved when a patient has known spinal metastasis:
Explanation
Question 6
A 32-year-old man develops left lower extremity discomfort following a basketball game. A magnetic resonance image of the lumbar spine reveals a posterolateral disk herniation at the level of L4/L5. All of the following conditions could be associated with this except:
Explanation
Question 7
A 43-year-old man develops pain radiating down his left leg from a far- lateral disk herniation at the L5/S1 level. Which is the most likely nerve root contributing to his discomfort:
Explanation
Question 8
Which orthopedic test, designed to apply tension to the spinal cord producing pain, involves having the patient lie supine while the examiner flexes the patient's head to his chest:
Explanation
Question 9
A 52-year-old man sustained an L1 burst fracture after falling from a ladder 3 weeks ago. He was found neurologically intact after initial examination. He has been treated with conservative management since the accident, but he now complains of an inability to void along with numbness and tingling in both of his legs. Computed tomography scan shows worsening conus compression. On physical examination, you discover that he has weak anal sphincter tone. Your next step in the treatment of this patient should be:
Explanation
Question 10
A 27-year-old man comes in for examination. He complains of worsening pain in his lower back. He states that the pain started 4 days ago after lifting a heavy box. The patient's neurological exam is completely nonfocal. The initial management of this patient should include:
Explanation
Question 11
When trying to distinguish sciatic radicular pain from pain following a hamstring strain, it is important to know that pain from a hamstring strain usually only involves the posterior aspect of thigh. Sciatic nerve pain may also be associated with:
Explanation
Question 12
A 42-year-old man sustained a twisting injury to his low back 5 months ago. Since the injury, he has persistent low back pain that radiates into his right thigh and down to his posterior calf. The patient underwent a magnetic resonance imaging of his lumbar spine revealing a small posterolateral lumbar disk herniation at the L4L5 level. Over the past month, the patient states that his leg pain has been getting progressively better and has almost disappeared over the past week with the use of nonsteroidal anti- inflammatory medications and occasional bed rest. The next step in the management of this patient should be:
Explanation
Question 13
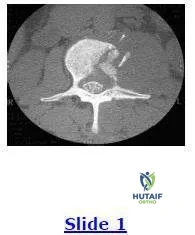
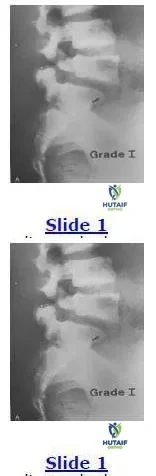
This radiograph shows a grade I spondylolisthesis of L5 on S1. This is due to a defect in what anatomical area:
Explanation
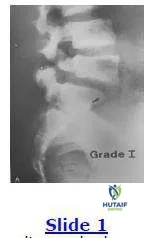 The anatomical region involved in a spondylolisthesis is the pars interarticularis that is located between the superior and inferior articular processes and is a high stress area of relatively thinner bone.
The anatomical region involved in a spondylolisthesis is the pars interarticularis that is located between the superior and inferior articular processes and is a high stress area of relatively thinner bone.
Question 14
A 16-year-old football lineman develops unrelenting low back pain for the past 3 months. Based on the magnetic resonance image shown, the next step in the management of this patient is:
Explanation
Question 15
A 50-year-old woman with 3 months of low back pain recently discovers a hard, painless lump in her breast. Due to the back discomfort, she undergoes plain radiography and subsequently a computed tomography scan (below). The most likely diagnosis is:
Explanation
Question 16
A 45-year-old construction worker with long standing low back pain now notices bilateral thigh and lower extremity discomfort for the past 6 months. He has undergone conservative treatment with little success including injection therapy. He cannot perform his work duties. Based on the lateral radiograph shown below, the next step in the management of the patient should consist of:
Explanation
Question 17
A 35-year-old woman presents with severe back pain. Radiographic evaluation reveals a thoracic curve of 70° and a loss of thoracic kyphosis. Surgery is recommended to correct the deformity. Which of the following tests must be ordered as part of the preoperative evaluation:
Explanation
Question 18
A calcified thoracic disk in the spinal canal is pathognomonic for:
Explanation
Question 19
Surgical treatment of thoracic disk herniation by a laminectomy is contraindicated because this procedure is associated with which of the following:
Explanation
Question 20
The most common presenting symptom of a patient with a thoracic disk herniation is:
Explanation
Question 21
A 68-year-old male presents with bilateral lower extremity aching and cramping that worsens with walking and improves when he leans forward on a shopping cart. Which of the following is the most characteristic clinical feature distinguishing this condition from vascular claudication?
Explanation
Question 22
A 42-year-old female presents with acute onset of low back pain radiating down the posterior thigh, lateral calf, and dorsum of the foot. Physical examination reveals weakness in extensor hallucis longus (EHL) and decreased sensation over the dorsal first web space. Which disc herniation is most likely responsible?
Explanation
Question 23
When evaluating a patient with spondylolisthesis, the Meyerding classification is commonly used to grade the severity of the slip. A Meyerding Grade III slip corresponds to what percentage of anterior translation of the superior vertebral body over the inferior one?
Explanation
Question 24
What is the primary anatomical defect responsible for the development of an isthmic spondylolisthesis?
Explanation
Question 25
On oblique lumbar radiographs, the posterior elements resemble a "Scotty dog". In the context of isthmic spondylolisthesis, a defect is often seen as a "collar" around the dog's neck. Which anatomical structure corresponds to the neck of the Scotty dog?
Explanation
Question 26
A 35-year-old male presents to the emergency department with severe acute low back pain and bilateral leg weakness. Which of the following is the most sensitive clinical finding for the early diagnosis of cauda equina syndrome?
Explanation
Question 27
A 50-year-old male is diagnosed with a far lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is most likely to be directly compressed by this specific herniation?
Explanation
Question 28
In a patient presenting with central lumbar spinal stenosis, which ligament undergoes characteristic hypertrophy and buckling, contributing significantly to dorsal compression of the thecal sac?

Explanation
Question 29
Discogenic low back pain is a common entity. The outer annulus fibrosus of the lumbar intervertebral disc is capable of nociception. Which nerve provides the primary innervation to the outer posterior third of the annulus fibrosus?
Explanation
Question 30
De novo degenerative lumbar scoliosis typically presents in older adults without a prior history of spinal curvature. What is the primary driving mechanism behind the development of this deformity?
Explanation
Question 31
A 65-year-old female presents with chronic lower back pain and neurogenic claudication. Radiographs demonstrate degenerative spondylolisthesis. Which vertebral level and direction of slip is most statistically common in this condition?
Explanation
Question 32
During a routine neurologic examination for back pain, the patient exhibits an absent Achilles tendon reflex but normal patellar reflexes. Motor testing shows weakness in plantar flexion. Which nerve root is primarily involved?
Explanation
Question 33
Waddell's signs are utilized during a physical examination to identify non-organic (psychological or behavioral) causes of back pain. Which of the following is NOT considered a positive Waddell's sign?
Explanation
Question 34
A 45-year-old male with persistent, severe lower back pain and L5 radiculopathy has a Grade II isthmic spondylolisthesis at L5-S1. He has failed extensive conservative management. What is the most appropriate surgical intervention?
Explanation
Question 35
A patient complains of lateral thigh and anterior knee pain. Examination reveals distinct weakness in knee extension against resistance and an absent patellar reflex. Sensation is decreased over the medial aspect of the lower leg. Which nerve root is most likely compressed?

Explanation
Question 36
A 58-year-old diabetic patient presents with unremitting back pain, fevers, and elevated ESR and CRP. You suspect pyogenic vertebral osteomyelitis. What is the most sensitive and specific imaging modality to confirm this diagnosis?
Explanation
Question 37
A 60-year-old male with a 30-year history of ankylosing spondylitis presents to the emergency room with new-onset mechanical back pain after a minor fall from standing height. Neurological exam is normal. What is the most critical suspected diagnosis that must be ruled out?
Explanation
Question 38
The normal adult intervertebral disc is the largest avascular structure in the human body. How does the central nucleus pulposus primarily receive its essential nutritional supply?
Explanation
Question 39
An anteroposterior (AP) radiograph of the lumbar spine reveals the "winking owl" sign in a patient with a known history of breast cancer. This radiographic sign indicates the lytic destruction of which specific anatomical structure?
Explanation
Question 40
A 65-year-old male presents with bilateral leg pain exacerbated by walking and relieved by sitting or leaning forward over a shopping cart. Examination reveals normal peripheral pulses. Which imaging study is the gold standard for confirming the primary diagnosis in a patient without surgical hardware?
Explanation
Question 41
A 42-year-old female presents to the emergency department with acute onset of severe low back pain, bilateral sciatica, and perineal numbness. Her post-void residual bladder volume is 400 mL. What is the next most appropriate step in management?
Explanation
Question 42
According to the Wiltse classification of spondylolisthesis, a slip that occurs secondary to an elongation of the pars interarticularis without a frank defect is classified as which type?
Explanation
Question 43
A 60-year-old female presents with neurogenic claudication. Sagittal T2-weighted MRI demonstrates central canal stenosis at L4-L5.
Which posterior spinal element predictably undergoes hypertrophy and buckling, contributing significantly to this central canal stenosis?
Explanation
Question 44
A 35-year-old man presents with right lower extremity radiating pain. Examination reveals weakness in extensor hallucis longus (EHL) and numbness over the dorsum of the right foot. The Achilles and patellar reflexes are symmetric and intact. Which nerve root is most likely affected?
Explanation
Question 45
A 24-year-old man is brought to the trauma bay following a high-speed motor vehicle collision where he was wearing only a lap belt. Radiographs reveal a flexion-distraction injury of the thoracolumbar spine (Chance fracture). What concomitant injury is highly associated with this fracture pattern?
Explanation
Question 46
A 65-year-old woman presents with lower back and leg pain. Imaging shows an L4-L5 anterior translation with an intact pars interarticularis.
Which of the following structural characteristics most directly predisposes this specific spinal level to degenerative spondylolisthesis?
Explanation
Question 47
A 40-year-old male presents with chronic stiffness and back pain. Radiographs reveal bridging syndesmophytes and bilateral fusion of the sacroiliac joints.
This classic "bamboo spine" radiographic appearance is most highly correlated with which human leukocyte antigen (HLA)?
Explanation
Question 48
A 60-year-old diabetic patient presents with unrelenting back pain and fever. Blood tests show an elevated CRP and ESR. MRI of the lumbar spine is obtained. Which of the following MRI findings is most characteristic of pyogenic spondylodiscitis as opposed to a neoplastic process?
Explanation
Question 49
In evaluating a 12-year-old female with adolescent idiopathic scoliosis (AIS), which of the following combinations of factors represents the highest risk for curve progression?
Explanation
Question 50
According to the Denis three-column theory of the spine, a classic burst fracture is radiographically characterized by failure of which columns under axial loading?
Explanation
Question 51
A patient who underwent an uncomplicated posterior lumbar spinal fusion 10 days ago presents with increasing incisional pain, wound erythema, and a temperature of 38.5 C. There is purulent drainage from the incision. What is the most appropriate initial management?
Explanation
Question 52
A 45-year-old patient presents with acute right-sided L4 radiculopathy. MRI reveals a far lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is typically compressed by a far lateral disc herniation at this specific anatomical level?
Explanation
Question 53
A 15-year-old male gymnast presents with a 4-month history of localized low back pain exacerbated by extension. Oblique radiographs of the lumbar spine are obtained.
A defect in which anatomical structure represents the collar on the "Scotty dog"?
Explanation
Question 54
A 62-year-old female presents with severe neurogenic claudication and a grade I degenerative spondylolisthesis at L4-L5. Which nerve root is most likely to be compressed in this condition?
Explanation
Question 55
A 16-year-old elite gymnast complains of lower back pain exacerbated by extension. Plain radiographs are normal. What is the most appropriate next imaging modality to detect an acute pars interarticularis stress reaction without radiation exposure?
Explanation
Question 56
Which of the following physical examination findings is NOT considered one of Waddell's signs for nonorganic back pain?
Explanation
Question 57
A 45-year-old male presents with acute severe back pain, bilateral leg radicular symptoms, and perineal numbness. What is the most sensitive clinical symptom or sign for the diagnosis of cauda equina syndrome?
Explanation
Question 58
A 50-year-old male is diagnosed with a far lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is most likely affected?
Explanation
Question 59
A 70-year-old male presents with neck and back stiffness. Radiographs demonstrate flowing anterior osteophytes over six contiguous vertebral bodies. Which of the following is a requisite radiographic criterion for the diagnosis of Diffuse Idiopathic Skeletal Hyperostosis (DISH)?
Explanation
Question 60
A 68-year-old woman complains of bilateral leg pain that worsens with walking and improves when sitting or leaning over a shopping cart. What is the most likely mechanism providing relief in this patient?
Explanation
Question 61
A 35-year-old male experiences acute radicular leg pain following heavy lifting. An MRI reveals a massive paracentral disc herniation at L5-S1. Which of the following physical examination findings is most anticipated?
Explanation
Question 62
Patients with ankylosing spondylitis who sustain minor trauma are at high risk for highly unstable spinal fractures. What unique associated complication is significantly more common in these patients following such fractures?
Explanation
Question 63
A 22-year-old male presents with axial back pain.
Based on a lateral lumbar spine radiograph showing isthmic spondylolisthesis, what is the primary anatomical defect responsible for this specific etiology?
Explanation
Question 64
A 65-year-old male presents with leg pain on walking.
MRI commonly demonstrates severe central canal stenosis. Which of the following anatomical structures is LEAST likely to be a primary contributor to acquired degenerative central spinal stenosis?
Explanation
Question 65
According to the Meyerding classification system for spondylolisthesis, what percentage of vertebral body slip defines a Grade III slip?
Explanation
Question 66
A 40-year-old male undergoes an Anterior Lumbar Interbody Fusion (ALIF) at L5-S1. Postoperatively, he has no motor or sensory deficits in his legs. What is a specific, well-documented risk uniquely associated with this surgical approach?
Explanation
Question 67
In evaluating adult spinal deformity, achieving appropriate sagittal balance is critical. Which of the following equations represents the fixed relationship between key pelvic parameters?
Explanation
Question 68
A 55-year-old intravenous drug user presents with fever, back pain, and progressive bilateral leg weakness over the last 12 hours. MRI shows a large posterior epidural fluid collection at T10 causing severe cord compression. What is the most appropriate management?
Explanation
Question 69
A patient develops severe back pain two weeks after a lumbar discectomy. MRI suggests postoperative discitis. Which laboratory marker is the most reliable and rapid indicator for monitoring response to antibiotic therapy?
Explanation
Question 70
A patient presents with a right-sided L5 radiculopathy due to a foraminal disc herniation at L5-S1. Which of the following motor functions is most predictably weakened?
Explanation
Question 71
An AP radiograph of the thoracic spine in a 60-year-old male with a history of prostate cancer reveals the "winking owl" sign at T9. What does this radiographic sign represent?
Explanation
Question 72
A 45-year-old presents with back pain and leg weakness.
If imaging demonstrates a large L4-L5 paracentral disc extrusion, which physical exam finding is most likely?
Explanation
Question 73
In evaluating a patient for lumbar spinal instability,
flexion-extension radiographs are obtained. Which translation distance in the lumbar spine is generally considered indicative of radiographic instability requiring stabilization?
Explanation
Question 74
A 45-year-old male presents with severe left anterior thigh pain and weakness in knee extension. MRI of the lumbar spine reveals an extraforaminal (far lateral) disc herniation at the L4-L5 level. Which nerve root is most likely compressed in this scenario?
Explanation
Question 75
A 14-year-old female presents with severe mechanical back pain and a wide-based waddling gait. Radiographs reveal a Grade III L5-S1 isthmic spondylolisthesis with a slip angle of 55 degrees and a high pelvic incidence. What is the most appropriate surgical management?
Explanation
Question 76
A 50-year-old male with long-standing ankylosing spondylitis presents to the emergency department after a minor ground-level fall. He complains of new, severe lower cervical neck pain. Plain radiographs of the cervical spine show no obvious fracture. What is the most appropriate next step in management?
Explanation
Question 77
A 68-year-old male presents with bilateral neurogenic claudication. Based on a typical sagittal MRI of the lumbar spine showing central canal stenosis
, which of the following structures is the primary contributor to dorsal compression of the thecal sac?
Explanation
Question 78
A 42-year-old female presents with severe acute low back pain radiating to both legs. Which of the following is considered the most sensitive early clinical symptom or sign of cauda equina syndrome?
Explanation
Question 79
An 82-year-old male with severe COPD and coronary artery disease presents after a fall. Imaging reveals a non-displaced Type II odontoid fracture. Which of the following is the most appropriate initial management?
Explanation
Question 80
A 55-year-old male undergoes an MRI for chronic low back pain. The radiologist notes Modic Type 1 changes at the L4-L5 vertebral endplates. What do these changes represent histologically?
Explanation
Question 81
According to the Wiltse classification of spondylolisthesis, Type 1 (Dysplastic) is most commonly associated with which of the following anatomic abnormalities?
Explanation
Question 82
A comatose 25-year-old male is brought to the trauma bay after a high-speed motor vehicle collision. Radiographs
reveal a bilateral C5-C6 facet dislocation. What is the most appropriate next step in management prior to definitive reduction?
Explanation
Question 83
The Lenke classification system for Adolescent Idiopathic Scoliosis (AIS) utilizes a sagittal modifier. Which specific radiographic measurement determines this modifier?
Explanation
Question 84
During a posterior lumbar spinal fusion, the surgeon prepares for pedicle screw insertion using the intersection technique. The typical entry point for a lumbar pedicle screw is located at the intersection of the transverse process and which other anatomic landmark?
Explanation
Question 85
A 40-year-old patient undergoes emergency laminectomy and discectomy for cauda equina syndrome secondary to a massive L4-L5 disc herniation. Postoperatively, what is the most common long-term persistent deficit in these patients?
Explanation
Question 86
A 30-year-old male presents after a diving accident. Imaging
demonstrates a traumatic spondylolisthesis of the axis (Hangman's fracture). What is the classic mechanism of injury for this fracture pattern?
Explanation
Question 87
In the assessment of adult spinal deformity, Pelvic Incidence (PI) is a key morphological parameter that is fixed for each individual after skeletal maturity. It is mathematically defined as the sum of which two parameters?
Explanation
Question 88
According to the Thoracolumbar Injury Classification and Severity Score (TLICS), which of the following findings contributes the most points towards the indication for surgical intervention?
Explanation
Question 89
The Nurick classification for cervical spondylotic myelopathy is heavily utilized in clinical assessment. It is primarily based on which of the following patient features?
Explanation
Question 90
Following a rigid L4-S1 posterior spinal fusion, the adjacent L3-L4 segment is at risk for accelerated degeneration (adjacent segment disease). Which biomechanical alteration primarily occurs at this adjacent level?
Explanation
Question 91
A 60-year-old diabetic male with an L3-L4 pyogenic spondylodiscitis caused by Staphylococcus aureus has been on targeted IV antibiotics for 2 days. What is the primary absolute indication for urgent surgical decompression?
Explanation
Question 92
A 72-year-old male with severe pre-existing cervical spondylosis presents after a fall resulting in a hyperextension injury to his neck
. Examination reveals profound motor weakness in his upper extremities with relatively preserved strength in his lower extremities. What is the most likely diagnosis?
Explanation
Question 93
When evaluating a patient with lower extremity claudication symptoms, which of the following historical findings is most indicative of neurogenic claudication (due to spinal stenosis) rather than vascular claudication?
Explanation
None
