Orthopedic Prometric MCQs - Chapter 3 Part 14

Orthopedic Prometric MCQs - Chapter 3 Part 14
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 14-year-old boy sustains a hip dislocation in a motor vehicle accident. Recommended treatment is:
Explanation
Question 2
Which of the following has not shown a decrease in the success rate of flexible intramedullary nails for femur fractures in children:
Explanation
Question 3
Which of the following is the best starting point for inserting a rigid femoral intramedullary nail in a 13-year-old boy:
Explanation
Question 4
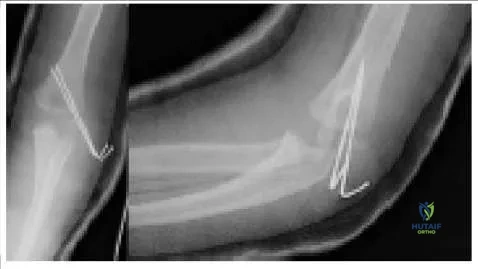
A patient had an elbow fracture that was openly reduced and internally fixed. The radiographs (Slide) from his first postoperative checkup are presented. Which of the following is a correct assessment:
Explanation
Question 5
Which of the following femur fractures is best treated with flexible intramedullary nails:
Explanation
Question 6
A mutation in the gene for peripheral myelin protein 22 causes which of the following disorders:
Explanation
Question 7
Which of the following statements is true of scoliosis in patients with C harcot-Marie-Tooth disease:
Explanation
Question 8
Risk factors for developmental dysplasia of the hip (DDH) include all of the following except:
Explanation
Question 9
In ultrasound of the infant hip, the alpha angle is defined as:
Explanation
Question 10
In a sonogram, the normal alpha angle of the neonatal hip measures:
Explanation
Question 11
Diagnosis of Duchenne muscular dystrophy in a female patient could be explained if the patient had which of the following:
Explanation
Question 12
Spinal muscular atrophy is due to a mutation in the gene for which of the following proteins:
Explanation
Question 13
Which of the following agents is contraindicated in children with open physes:
Explanation
Question 14
A 15-month-old toddler, who is neurologically intact, presents with a fracture (pic). Which of the following is the recommended treatment:
Explanation

Question 15
A 17-month-old toddler sustained a femur fracture (Slide) in a fall from a height. Which of the following is the best treatment method:
Explanation
Question 16
The lesion shown in the radiograph (pic) most likely represents which of the following processes:
Explanation
 An aneurysmal bone cyst is typically more septated and expansile in width, fibrous dysplasia has a more blurred zone of transition and ground-glass appearance, and a fibrous cortical defect is more eccentrically placed.
An aneurysmal bone cyst is typically more septated and expansile in width, fibrous dysplasia has a more blurred zone of transition and ground-glass appearance, and a fibrous cortical defect is more eccentrically placed.
Question 17
A clinical photograph (Slide 1) and radiographs (Slide 2) of a 13-year-old girl, who is neurologically normal, are presented. She does not report any pain. The most likely diagnosis is:
Explanation
 This patient has neurofibromatosis-1. She has a dystrophic scoliosis that is sharply angulated and involves only four vertebrae (Cobb levels T12-L3). The pedicles are thinned, and the endplates are scalloped. She also has subcutaneous neurofibromas.
This patient has neurofibromatosis-1. She has a dystrophic scoliosis that is sharply angulated and involves only four vertebrae (Cobb levels T12-L3). The pedicles are thinned, and the endplates are scalloped. She also has subcutaneous neurofibromas.
Question 18
An 11-year-old girl presents with a limp. She has no history of trauma, infection, or neurologic disorder. She does not report any pain. Recommended treatment includes:
Explanation
 This patient has untreated developmental dysplasia of the hip. Her limp cannot be eliminated. If she is not experiencing pain, then no treatment is indicated.
This patient has untreated developmental dysplasia of the hip. Her limp cannot be eliminated. If she is not experiencing pain, then no treatment is indicated.
Question 19
The foot pictured in this clinical photograph (pic) represents:
Explanation
 The foot presented in the clinical photograph represents congenital vertical talus. Note the equinus of the hindfoot, calcaneus of the forefoot, and the crease in the sinus tarsi. In patients with a calcaneovalgus foot, the hindfoot is in calcaneus, not equinus.
The foot presented in the clinical photograph represents congenital vertical talus. Note the equinus of the hindfoot, calcaneus of the forefoot, and the crease in the sinus tarsi. In patients with a calcaneovalgus foot, the hindfoot is in calcaneus, not equinus.
Question 20
Scapulothoracic fusion is most commonly indicated to help improve function in which of the following conditions:
Explanation
Question 21
A 2-year-old boy sustains a spiral midshaft femur fracture. He is otherwise healthy and no non-accidental trauma is suspected. What is the most appropriate initial management?
Explanation
Question 22
When utilizing a rigid lateral entry intramedullary nail for a femur fracture in a 13-year-old, the starting point should be placed lateral to the tip of the greater trochanter primarily to avoid injury to which of the following structures?
Explanation
Question 23
An obese 12-year-old boy presents with left knee pain and inability to bear weight. Radiographs show a displaced proximal femoral epiphysis. According to the Loder classification, what is the primary risk associated with this specific presentation?
Explanation
Question 24
A 7-year-old girl is scheduled for Titanium Elastic Nailing (TENs) of a transverse midshaft femur fracture. What is the recommended formula for selecting the appropriate nail diameter?
Explanation
Question 25
A 9-year-old boy sustains a traumatic proximal femur fracture. Radiographs reveal a transepiphyseal fracture with dislocation of the femoral head. What is the Delbet classification and the associated risk of avascular necrosis (AVN)?
Explanation
Question 26
A 6-year-old girl sustains an acute traumatic posterior hip dislocation. What is the most critical factor in minimizing her risk of developing osteonecrosis of the femoral head?
Explanation
Question 27
A 9-year-old boy weighing 45 kg (99 lbs) sustains a highly comminuted, length-unstable midshaft femur fracture resulting in 4 cm of shortening. What is the most appropriate surgical treatment?
Explanation
Question 28
In a 6-month-old pre-ambulatory infant presenting with an isolated femur fracture, which of the following fracture patterns is most specific for non-accidental trauma (child abuse)?
Explanation
Question 29
Following conservative management of a midshaft femur fracture in a 5-year-old child, the treating orthopedic surgeon should anticipate the maximum amount of femoral overgrowth to occur within what timeframe post-injury?
Explanation
Question 30
A 6-year-old boy underwent Titanium Elastic Nailing for a femur fracture 6 months ago. The fracture has healed well, but he complains of localized pain and a palpable mass near the medial and lateral knee. What is the most likely cause?
Explanation
Question 31
A 15-year-old sprinter presents with acute groin pain after pushing off the starting blocks. Radiographs show an avulsion fracture of the anterior inferior iliac spine (AIIS). Which muscle is responsible for this injury?
Explanation
Question 32
A 3-week-old neonate sustains a midshaft femur fracture during a difficult breech delivery. What is the most appropriate and effective treatment?
Explanation
Question 33
A 13-year-old boy underwent in situ pinning of a stable slipped capital femoral epiphysis (SCFE) with a single cannulated screw. Postoperatively, he develops severe stiffness, loss of motion, and global joint space narrowing (< 3mm) on radiographs without osteonecrosis. What is the most likely diagnosis?
Explanation
Question 34
Which of the following physical examination findings is most indicative of an unrecognized sciatic nerve injury following a traumatic posterior hip dislocation in a 10-year-old child?
Explanation
Question 35
When utilizing flexible intramedullary nails for a pediatric femur fracture, what technical error is most likely to result in a loss of reduction and subsequent varus or valgus malalignment?
Explanation
Question 36
A 16-year-old water skier presents with acute buttock pain after a forced hyperflexion of the hip with the knee extended. Radiographs reveal an ischial tuberosity avulsion fracture. Surgical fixation is generally indicated if the displacement exceeds:
Explanation
Question 37
A 7-year-old boy presents with a significantly displaced subtrochanteric femur fracture. Treatment with flexible intramedullary nails is considered. What is the most common malalignment complication seen when treating this specific fracture pattern with flexible nails?
Explanation
Question 38
A 12-year-old sustains a Delbet Type III (cervicotrochanteric) fracture of the proximal femur. Which of the following complications is most frequently observed following this specific fracture pattern?
Explanation
Question 39
In a 7-year-old child treated non-operatively for a diaphyseal femur fracture, what is the maximum acceptable varus/valgus angulation?
Explanation
Question 40
A 6-year-old boy weighing 35 kg sustains a highly comminuted, length-unstable fracture of the femoral diaphysis after a fall from a tree. What is the most appropriate surgical intervention?
Explanation
Question 41
When planning flexible titanium intramedullary nailing for a pediatric transverse femur fracture, what is the optimal diameter sizing for each nail?
Explanation
Question 42
A 7-year-old child undergoes flexible intramedullary nailing for a femoral shaft fracture. What is the most common complication associated with this procedure?
Explanation
Question 43
A 12-year-old boy presents with a displaced transcervical (Delbet Type II) fracture of the proximal femur. Which of the following complications occurs with the highest frequency in this fracture pattern?
Explanation
Question 44
A 4-year-old girl sustains an isolated, closed midshaft femur fracture. Non-operative management with a spica cast is elected. What is the maximum acceptable varus/valgus angulation in this age group?
Explanation
Question 45
A 13-year-old boy requires a rigid intramedullary nail for a midshaft femur fracture. To minimize the risk of iatrogenic avascular necrosis, the optimal starting point for nail insertion is:
Explanation
Question 46
A 3-year-old boy presents with a spiral midshaft femur fracture. The parents state he tripped while running on a carpeted floor. What is an essential component of the initial evaluation?
Explanation
Question 47
Which of the following scenarios is an absolute contraindication to the use of a Pavlik harness for the treatment of developmental dysplasia of the hip (DDH)?
Explanation
Question 48
A 13-year-old obese boy presents with an acute inability to bear weight on his right leg after a minor fall, diagnosed as a slipped capital femoral epiphysis (SCFE). According to the Loder classification, this inability to bear weight defines the slip as unstable. What is the approximate risk of avascular necrosis in this type of SCFE?
Explanation
Question 49
In the initial casting phase of the Ponseti method for a newborn with idiopathic clubfoot, the first step focuses on correcting which component of the deformity?
Explanation
Question 50
A 14-year-old boy is diagnosed with an unstable slipped capital femoral epiphysis (SCFE). To minimize the risk of avascular necrosis and optimize outcomes, what is the widely recommended surgical timing?
Explanation
Question 51
An 11-year-old boy presents with chronic knee pain. Radiographs reveal a classic osteochondritis dissecans (OCD) lesion. What is the most common anatomical location for this pathology?
Explanation
Question 52
An 8-year-old girl undergoes successful closed reduction of a traumatic posterior hip dislocation within 4 hours. A post-reduction CT scan identifies a 4 mm intra-articular osteochondral fragment. The joint space is clinically symmetric. What is the most appropriate management?
Explanation
Question 53
In a 6-year-old child treated non-operatively for a diaphyseal femur fracture, longitudinal overgrowth is expected. At what age range does this overgrowth phenomenon peak?
Explanation
Question 54
An 11-year-old boy sustains a Salter-Harris Type II fracture of the distal femur following a football tackle. Which of the following complications is most highly associated with this specific injury?
Explanation
Question 55
A 14-year-old girl sustains a Tillaux fracture of the ankle. Which quadrant of the distal tibial physis is the last to close, allowing for this specific avulsion fracture pattern?
Explanation
Question 56
What is the characteristic mechanism of injury that produces a pediatric triplane fracture of the ankle?
Explanation
Question 57
A 6-year-old boy with Legg-Calvé-Perthes disease is evaluated. According to the Herring lateral pillar classification, a Type C rating signifies which of the following?
Explanation
Question 58
A 13-year-old male athlete presents with localized pain, swelling, and tenderness over the tibial tubercle, which worsens with jumping. He is diagnosed with Osgood-Schlatter disease. What is the primary underlying pathology?
Explanation
Question 59
A 1-year-old child is diagnosed with congenital anterolateral bowing of the tibia. Radiographs demonstrate medullary sclerosis and early cystic changes at the apex of the bow. If left untreated, what is the most likely natural history of this condition?
Explanation
Question 60
A 13-year-old boy sustains a diaphyseal femur fracture. A rigid intramedullary nail is selected for fixation. To minimize the risk of iatrogenic avascular necrosis (AVN) of the femoral head, which of the following is the recommended starting point?
Explanation
Question 61
A 15-year-old boy presents with a posterior hip dislocation following a high-speed motor vehicle collision. Which of the following factors is the most significant predictor for the development of avascular necrosis (AVN)?
Explanation
Question 62
Which of the following factors is an accepted relative contraindication to the use of titanium elastic nails (TENs) for the treatment of a pediatric diaphyseal femur fracture?
Explanation
Question 63
A 4-year-old child sustains an isolated midshaft femur fracture. The child is placed in a one-and-a-half spica cast. What is the maximum acceptable amount of initial shortening in this patient?
Explanation
Question 64
An 8-year-old girl is treated with titanium elastic nails for a transverse midshaft femur fracture. What is the most commonly reported complication associated with this treatment modality?
Explanation
Question 65
A 9-year-old boy sustains a length-unstable subtrochanteric femur fracture. What is the most appropriate surgical intervention to provide stable fixation and minimize complications?
Explanation
Question 66
Which of the following describes the proper sizing technique for selecting titanium elastic nails (TENs) for a pediatric femur fracture?
Explanation
Question 67
A 10-year-old boy sustains a Delbet Type II (transcervical) femoral neck fracture. Following closed reduction and percutaneous pinning, the parents should be counseled that the child is at highest risk for which of the following complications?
Explanation
Question 68
A 5-year-old boy with a closed head injury (GCS 7) and a closed midshaft femur fracture is brought to the trauma bay. What is the primary advantage of early operative fixation of the femur in this polytraumatized child?
Explanation
Question 69
Which of the following injury patterns has the highest incidence of avascular necrosis in the pediatric population?
Explanation
Question 70
A 12-year-old, 80-kg male sustains a transverse midshaft femur fracture. Based on his age and weight, what is the most appropriate fixation strategy?
Explanation
Question 71
A 14-year-old girl is diagnosed with a traumatic posterior hip dislocation. Closed reduction is performed in the emergency department within 2 hours. Post-reduction CT scan reveals a 2 mm intra-articular fragment. The joint is congruent. What is the next best step in management?
Explanation
Question 72
A 3-year-old girl presents with an isolated closed spiral fracture of the femoral diaphysis. There are no signs of non-accidental trauma, and the injury occurred from a twisting fall at a playground. What is the most appropriate initial treatment?
Explanation
Question 73
During the insertion of a rigid intramedullary nail for an adolescent femur fracture, the surgeon inadvertently uses a starting point at the tip of the greater trochanter instead of lateral to it. What growth disturbance is most likely to occur?
Explanation
Question 74
An 11-year-old boy presents with a displaced Salter-Harris II fracture of the distal femur following a football tackle. Which of the following complications occurs with the highest frequency following this specific injury?
Explanation
Question 75
A 6-month-old infant is diagnosed with an unstable midshaft femur fracture. Which of the following is the most appropriate treatment option?
Explanation
Question 76
What is the primary rationale for pre-bending titanium elastic nails (TENs) prior to insertion in a pediatric femur fracture?
Explanation
Question 77
An 8-year-old child sustains a highly comminuted midshaft femur fracture resulting from a gunshot wound. Soft tissues are viable but there is a 3 cm open wound laterally. Which of the following is the most appropriate fixation method?
Explanation
Question 78
A 10-year-old child treated with a hip spica cast for a femur fracture develops severe abdominal pain, nausea, and vomiting 2 days post-application. What is the most likely diagnosis?
Explanation
Question 79
A 2-year-old child is brought to the emergency department for refusal to walk. Radiographs show a nondisplaced spiral fracture of the distal third of the tibia. What is the classic mechanism for this injury?
Explanation
Question 80
A 10-year-old boy weighing 55 kg sustains a transverse midshaft femur fracture. Which of the following is the most significant risk factor for failure if treated with titanium elastic nails (TENs)?
Explanation
Question 81
When using a rigid intramedullary nail for a femoral shaft fracture in an adolescent with open physes, avoiding the piriformis fossa and instead utilizing a lateral trochanteric entry point primarily minimizes the risk of:
Explanation
Question 82
A 9-year-old boy weighing 40 kg sustains a comminuted, length-unstable subtrochanteric femur fracture after a fall.
Which of the following fixation methods is most appropriate to maintain length and alignment?
Explanation
Question 83
A 12-year-old sustains a traumatic posterior hip dislocation during a motor vehicle accident. Closed reduction is delayed and performed 8 hours after the injury. What is the most devastating complication directly related to this delay?
Explanation
Question 84
An obese 13-year-old boy presents with left knee pain and an obligatory external rotation of the left hip during flexion. Which of the following is the most appropriate initial imaging step?
Explanation
Question 85
During in-situ pinning of a slipped capital femoral epiphysis (SCFE), an unrecognized intra-articular pin penetration into the anterosuperior quadrant of the femoral head most commonly leads to:
Explanation
Question 86
In a patient diagnosed with Legg-Calvé-Perthes disease, which of the following factors is most strongly associated with a poor radiographic outcome and a spherical mismatch at skeletal maturity?
Explanation
Question 87
A 9-month-old non-ambulatory infant presents with a spiral fracture of the femoral shaft. The parents state the child 'rolled off the bed.' What is the most appropriate next step in management alongside immobilization?
Explanation
Question 88
When treating a diaphyseal femur fracture in a 2-year-old child with an early spica cast, what is the optimal acceptable initial overriding (shortening) to allow for expected growth stimulation?
Explanation
Question 89
A 4-week-old female undergoes a screening ultrasound for developmental dysplasia of the hip (DDH). The Graf alpha angle is reported as 65 degrees. What does this indicate?
Explanation
Question 90
A newborn is diagnosed with arthrogryposis multiplex congenita and bilateral developmental dysplasia of the hip. Why is a Pavlik harness contraindicated in the management of this patient?
Explanation
Question 91
A 4-year-old boy presents with right hip pain, a temperature of 38.8°C, an ESR of 50 mm/hr, and a WBC count of 14,000 cells/mm³. He refuses to bear weight. According to the Kocher criteria, what is the probability that he has septic arthritis?
Explanation
Question 92
A 10-year-old boy sustains a Salter-Harris type II fracture of the distal femur. What is the most common long-term complication specifically associated with this injury?
Explanation
Question 93
In which of the following patients presenting with a unilateral slipped capital femoral epiphysis (SCFE) is prophylactic pinning of the contralateral hip most strongly indicated?
Explanation
None
