Orthopedic Prometric MCQs - Chapter 3 Part 40
Orthopedic Prometric MCQs - Chapter 3 Part 40
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The primary restraint to anterior translation of the abducted and externally rotated glenohumeral joint is the:
Explanation
Question 2
The quadriceps angle or Q angle is defined as the angle formed by a line connecting the:
Explanation
Question 3
Innervation to the anterior cruciate ligament is provided by a branch of the:
Explanation
Question 4
All of the following represent mechanisms of injury to the posterior cruciate ligament except:
Explanation
Question 5
Which of the following sets of compartment measurements confirms the diagnosis of exertional compartment syndrome:
Explanation
Question 6
The most common adverse side effect of dietary supplementation with creatine in athletes is:
Explanation
Question 7
When testing an elbow for insufficiency of the medial collateral ligament, valgus stress should be applied with the elbow positioned at:
Explanation
Question 8
Internal impingement of the shoulder between the posterosuperior glenoid rim and the rotator cuff typically occurs with the arm in this position:
Explanation
Question 9
The following structure is most responsible for anterior stability of the glenohumeral joint with the arm in 45° of abduction:
Explanation
Question 10
The following structure is most responsible for resisting inferior translation of the glenohumeral joint with the arm at the side:
Explanation
Question 11
Maximal external rotation of the shoulder occurs during which phase of pitching:
Explanation
Question 12
A 35-year-old avid rock climber complains of persistent anterior elbow pain with climbing, particularly when pulling himself up with his arms. The following muscle would most likely show increased activity on an electromyogram:
Explanation
Question 13
A 16-year-old baseball pitcher complains of dominant-sided elbow pain when pitching. He has recently been removed from the pitching rotation because of "control" problems. Physical examination reveals pain when a supinated, flexed, and valgus stressed elbow is brought into progressive extension. The most likely diagnosis is:
Explanation
Question 14
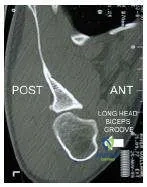
This slide is a computed tomogram of the shoulder of a 22-year-old rugby player. The most likely diagnosis is:
Explanation
Question 15
This slide is a computed tomogram of the dominant shoulder of a 45-year- old male tennis player. The most likely diagnosis is:

Explanation
Question 16
Weight training that employs constant resistance throughout the arc of motion is referred to as:
Explanation
Question 17
Weight training that employs a constant velocity and variable resistance is referred to as:
Explanation
Question 18
During arthroscopic repair of a medial meniscal tear, the following structure is at greatest risk for damage:
Explanation
Question 19
During arthroscopic repair of a lateral meniscal tear, the following structure is at greatest risk for damage:
Explanation
Question 20
A 15-year-old male football player is discovered to have a reproducible painless pop with meniscal testing during a routine preparticipation physical examination. The patient states that he has never experienced any knee problems other than an occasional audible pop. His family physician orders a magnetic resonance image. It shows a discoid lateral meniscus without evidence of tearing. Recommended management should include:
Explanation
Question 21
With the arm resting at the side in 0 degrees of abduction, what is the primary static restraint to inferior translation of the glenohumeral joint?
Explanation
Question 22
Which of the following statements correctly describes the functional biomechanics of the anterior cruciate ligament (ACL) bundles?
Explanation
Question 23
A 24-year-old male presents with a locked knee after a twisting injury during a soccer match. An MRI is obtained as shown below.
What is the most likely diagnosis?
Explanation
Question 24
During open kinetic chain knee extension, the "screw-home" mechanism ensures maximal joint congruency in terminal extension. This mechanism is primarily characterized by which of the following coupled kinematic motions?
Explanation
Question 25
A 22-year-old collegiate baseball pitcher presents with medial elbow pain during the acceleration phase of throwing. Physical examination reveals valgus instability at 90 degrees of elbow flexion. Which structure is most likely injured?
Explanation
Question 26
During a pectoralis major tendon repair, a surgeon must restore normal anatomical footprints. How does the sternal head of the pectoralis major muscle normally insert on the humerus relative to the clavicular head?
Explanation
Question 27
In the setting of an acromioclavicular (AC) joint injury, which ligament functions as the primary static restraint to superior translation of the distal clavicle?
Explanation
Question 28
A 25-year-old overhead athlete complains of posterior shoulder pain and a subjective feeling of a "dead arm" during the late cocking phase of throwing. Based on the provided MRI finding,
which pathophysiologic mechanism best explains the development of this specific capsulolabral pathology?
Explanation
Question 29
The posterolateral corner (PLC) of the knee, consisting primarily of the fibular collateral ligament, popliteus tendon, and popliteofibular ligament, functions as the primary restraint to which of the following combined forces?
Explanation
Question 30
A physical therapist is designing a rehabilitation protocol for a patient with severe patellofemoral osteoarthritis. To minimize patellofemoral joint reaction forces during open kinetic chain (OKC) knee extension exercises, the patient should avoid which arc of motion?
Explanation
Question 31
A professional volleyball player presents with insidious onset of shoulder weakness. Examination reveals marked atrophy of the infraspinatus with isolated weakness in external rotation, but normal supraspinatus bulk and strength. Where is the most likely site of nerve compression?
Explanation
Question 32
Which of the following closely approximates the anticipated increase in contact stresses within the medial compartment of the knee following a complete medial meniscectomy?
Explanation
Question 33
During reconstruction of the medial patellofemoral ligament (MPFL), identifying the correct femoral origin is critical to ensure appropriate graft isometry. Radiographically, the anatomic femoral attachment (Schöttle's point) is located where?
Explanation
Question 34
A 21-year-old dancer suffers an acute inversion ankle sprain while "en pointe" (maximally plantarflexed). Which ligament serves as the primary restraint to inversion in this foot position and is most likely to be injured?
Explanation
Question 35
Posterolateral rotatory instability (PLRI) of the elbow typically follows a traumatic dislocation or iatrogenic injury. This condition is primarily characterized by insufficiency of which of the following ligamentous structures?
Explanation
Question 36
Which of the following ligamentous structures is the strongest in the human body and serves as the primary static restraint to hyperextension and external rotation of the hip joint?
Explanation
Question 37
In the assessment of anterior glenohumeral instability, the concept of the "glenoid track" is utilized to evaluate bone loss. An "engaging" Hill-Sachs lesion is best defined clinically and radiographically as a defect that:
Explanation
Question 38
The posterior cruciate ligament (PCL) provides the primary restraint to posterior tibial translation and is composed of two functional bundles. Which statement accurately describes the tension pattern of the anterolateral (AL) bundle?
Explanation
Question 39
Unlike the medial collateral ligament (MCL), the anterior cruciate ligament (ACL) possesses a notoriously poor intrinsic healing capacity following complete rupture. Which biological factor is a primary driver of this clinical observation?
Explanation
Question 40
To permit full active elevation of the arm overhead, the clavicle must undergo complex, coupled movements at the sternoclavicular and acromioclavicular joints. During this full elevation, the clavicle normally undergoes which essential motion?
Explanation
Question 41
The primary restraint to varus stress at 30 degrees of knee flexion is the:
Explanation
Question 42
During an acromioclavicular joint reconstruction, the surgeon reconstructs the conoid and trapezoid ligaments. The conoid ligament inserts onto the clavicle at what distance from the distal end of the clavicle?
Explanation
Question 43
Peak patellofemoral joint reaction forces during normal gait occur at which phase?
Explanation
Question 44
The anterolateral bundle of the posterior cruciate ligament (PCL) is most taut in which position?
Explanation
Question 45
Which of the following arteries is considered the principal blood supply to the articular segment of the humeral head?
Explanation
Question 46
Which of the following structures is NOT considered part of the boundaries or contents of the rotator cuff interval?
Explanation
Question 47
What is the primary difference in the vascularity of the medial and lateral menisci in an adult?
Explanation
Question 48
The spring ligament (plantar calcaneonavicular ligament) primarily supports the head of the talus. Which of the following tendons provides dynamic support directly inferior to this ligament?
Explanation
Question 49
The artery of the ligamentum teres is a branch of which of the following arteries?
Explanation
Question 50
Which annular pulleys are most critical to preserve during flexor tendon surgery to prevent bowstringing?
Explanation
Question 51
Which of the following positions represents the close-packed position of the glenohumeral joint?
Explanation
Question 52
Evaluate the following image of a knee stress radiograph.
In an isolated posterior cruciate ligament (PCL) injury, the maximum posterior tibial translation observed at 90 degrees of flexion is typically:
Explanation
Question 53
During a classic deltopectoral approach to the shoulder, the cephalic vein is typically retracted in which direction to preserve its primary draining tributaries?
Explanation
Question 54
Consider the biomechanical principles shown in the diagram.
In the setting of a reverse total shoulder arthroplasty, lateralization of the glenosphere primarily achieves which of the following?
Explanation
Question 55
The primary stabilizer of the distal radioulnar joint (DRUJ) during forearm supination is the:
Explanation
Question 56
In the subaxial cervical spine, the greatest amount of flexion-extension occurs at which of the following segmental levels?
Explanation
Question 57
According to static biomechanical models of the hip during single-leg stance, the ratio of the force generated by the hip abductors to body weight is approximately:
Explanation
Question 58
Tendons are primarily composed of type I collagen. Which of the following proteoglycans is most abundant in the tensile-bearing regions of normal tendons?
Explanation
Question 59
The medial plantar nerve provides motor innervation to all of the following muscles EXCEPT the:
Explanation
Question 60
Following a diaphyseal fracture treated with rigid plate fixation (absolute stability), healing primarily occurs via which of the following mechanisms?
Explanation
Question 61
The primary restraint to inferior translation of the glenohumeral joint with the arm in 0 degrees of abduction is the:
Explanation
Question 62
During anterior cruciate ligament (ACL) reconstruction, non-anatomic anterior placement of the femoral tunnel will most likely result in a graft that is:
Explanation
Question 63
A 24-year-old baseball pitcher presents with medial elbow pain. Clinical evaluation demonstrates valgus instability of the elbow. The anterior bundle of the ulnar collateral ligament (UCL), which is the primary restraint to this stress, inserts onto which of the following structures?
Explanation
Question 64
Which of the following components of the posterolateral corner (PLC) of the knee is the primary restraint to external tibial rotation at 30 degrees of knee flexion?
Explanation
Question 65
A 28-year-old volleyball player has weakness in external rotation but normal abduction strength. An MRI shows isolated atrophy of the infraspinatus. Entrapment of the suprascapular nerve is most likely occurring at which location?
Explanation
Question 66
Which of the following structures forms the superior border of the quadrangular space, through which the axillary nerve and posterior circumflex humeral artery pass?
Explanation
Question 67
The anteromedial (AM) bundle of the anterior cruciate ligament (ACL) can be biomechanically differentiated from the posterolateral (PL) bundle by which of the following characteristics?
Explanation
Question 68
A 32-year-old male presents with recurrent patellar instability. The primary ligamentous restraint to lateral patellar translation at 0 to 30 degrees of knee flexion originates from a point strictly defined by radiographic landmarks. Where is this femoral origin located?
Explanation
Question 69
Regarding the menisci of the knee, which of the following statements most accurately describes their vascular supply and intrinsic healing potential?
Explanation
Question 70
A 21-year-old football player sustains a high-energy knee injury. Clinical examination reveals a positive dial test at 30 degrees of knee flexion but symmetric external rotation at 90 degrees. This pattern is pathognomonic for an isolated injury to which structure?
Explanation
Question 71
A 19-year-old athlete undergoes evaluation for shoulder instability.
Which of the following physical examination findings is most specific for a superior labrum anterior and posterior (SLAP) tear?

Explanation
Question 72
The medial collateral ligament (MCL) of the knee consists of superficial and deep layers. The superficial MCL is the primary restraint to valgus stress. Where is its primary tibial insertion?
Explanation
Question 73
A 35-year-old male presents with posterolateral rotatory instability (PLRI) of the elbow after a traumatic dislocation. The primary ligamentous restraint deficient in this condition is the lateral ulnar collateral ligament (LUCL). What is the normal insertion site of the LUCL?
Explanation
Question 74
Which of the following combinations of structures accurately defines the contents of the rotator interval of the shoulder?
Explanation
Question 75
The posterior cruciate ligament (PCL) is the primary restraint to posterior translation of the tibia relative to the femur. At what degree of knee flexion does it provide the maximum percentage of this restraining force?
Explanation
Question 76
The medial patellofemoral ligament (MPFL) is recognized as the primary soft tissue restraint against lateral patellar translation. At what angle of knee flexion does it provide the greatest percentage of this restraining force?
Explanation
Question 77
The superior glenohumeral ligament (SGHL) provides the primary restraint to inferior translation of the humeral head in which of the following shoulder positions?
Explanation
Question 78
Which ligament acts as the primary restraint to anterior translation of the talus within the ankle mortise when the foot is positioned in plantar flexion?
Explanation
Question 79
During the late cocking phase of throwing, which elbow structure serves as the primary restraint against valgus stress?
Explanation
Question 80
The lateral meniscus differs from the medial meniscus in both morphology and mobility. Which of the following statements accurately describes the lateral meniscus?
Explanation
Question 81
The primary blood supply to the anterior cruciate ligament (ACL) is derived from which of the following vascular structures?
Explanation
Question 82
The scapholunate interosseous ligament is a C-shaped structure essential for proximal carpal row stability. Which portion of this ligament is the strongest and acts as the primary restraint to dorsal translation and diastasis?
Explanation
Question 83
In the setting of a massive rotator cuff tear involving the supraspinatus and infraspinatus, which intact anatomical structure limits superior translation (escape) of the humeral head?
Explanation
Question 84
The Achilles tendon is most susceptible to rupture in its distinct hypovascular "watershed" zone. This region is typically located what distance proximal to its insertion on the calcaneal tuberosity?
Explanation
Question 85
A 28-year-old overhead throwing athlete presents with deep posterior shoulder pain during the late cocking phase of throwing.
What is the primary stabilizing role of the superior labrum anterior to posterior (SLAP) complex during this motion?
Explanation
Question 86
The coracoclavicular (CC) ligaments provide the primary vertical stability to the acromioclavicular joint. Which of the following accurately describes the anatomic relationship between the two distinct ligaments comprising this complex?
Explanation
Question 87
The "screw-home" mechanism of the knee provides terminal extension stability, locking the joint. This mechanism is primarily driven by which inherent anatomical feature?
Explanation
Question 88
A 22-year-old female sustains a non-contact pivoting injury to her knee, reporting a loud pop.
Assuming an acute anterior cruciate ligament (ACL) rupture occurred, which associated meniscal injury is most commonly encountered in this acute setting?
Explanation
Question 89
Which of the following capsular ligaments is considered the thickest and strongest in the human body, serving as the primary restraint against hyperextension of the hip joint?
Explanation
Question 90
The anterolateral ligament (ALL) of the knee has been identified as a secondary restraint to internal tibial rotation. What is the typical anatomic insertion site of this ligament?
Explanation
Question 91
During a closed kinetic chain lower extremity exercise, such as a deep squat, patellofemoral joint reaction forces reach their peak at approximately which range of knee flexion?
Explanation
Question 92
During an arthroscopic inside-out repair of a posterior horn tear of the medial meniscus, aberrant suture passage poses the greatest iatrogenic risk to which of the following nerves?
Explanation
Question 93
In an adult patient, the intrinsic blood supply to the menisci of the knee is physiologically restricted to which anatomical zone?
Explanation
None
