Orthopedic Prometric MCQs - Chapter 3 Part 29

Orthopedic Prometric MCQs - Chapter 3 Part 29
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following populations is most at risk for compression fractures of the spine:
Explanation
Question 2
Following an osteoporotic compression fracture, the risk of sustaining another compression fracture at a different level is increased by:
Explanation
Question 3
The following are all purported benefits of percutaneous intraosseous methylmethacrylate injection (vertebroplasty) for the treatment of osteoporotic compression fractures except:
Explanation
Question 4
Acute thoracic compression fractures should have the following signal characteristics on magnetic resonance imaging:
Explanation
Question 5
In this slide of a lumbar burst fracture, which column is disrupted to distinguish it from a compression fracture:
Explanation
Question 6
When evaluating thoracolumbar burst fractures, it is important to remember that the spinal cord ends in the conus medullaris, which typically is present at what level:
Explanation
Question 7
Canal compromise in burst fractures (Slide) is caused by:
Explanation
Question 8
A 16-year-old boy sustains a burst fracture of L2. Radiographs indicate loss of approximately 20% of vertebral height anteriorly and 10° of kyphosis. He is neurologically intact. Management should include:

Explanation
Question 9
The sagittal plumb line should fall:
Explanation
Question 10
Normal sagittal thoracic alignment is:
Explanation
Question 11
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. What questions from his history can help differentiate vascular from neurogenic claudication:
Explanation
Question 12
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. The patient is diagnosed with neurogenic claudication. What is the most likely source of his symptoms:
Explanation
Question 13
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. A magnetic resonance image (MRI) of the patient is obtained (Slide). What does the MRI show:
Explanation
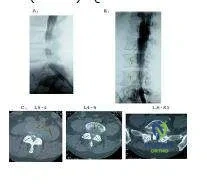
The MRI shows moderately severe lumbar stenosis at L3-L4 and L4-L5. While the degree or severity of stenosis remains subjective, terming this stenosis critical is an exaggeration. The section of the axial images at L5-S1 is not in plane with the disk, hence there appears to be lateral recess stenosis at this level also. The sagittal images, however, do not confirm this diagnosis. There is no evident lumbar disk herniation, and there are no findings indicative of lumbar metastatic disease.
Question 14
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. A magnetic resonance image (MRI) of the patient is obtained, as well as a myelogram (Slide). Conservative options in this patient include:
Explanation
Question 15
A 70-year-old man complains of severe, burning pain in both calves after he ambulates approximately one block. He denies significant back pain. He has long-standing, insulin-dependent diabetes mellitus and a history of coronary artery disease. The patient has smoked two packs of cigarettes each day for more than 30 years. Based upon the patientâ s history, magnetic resonance image (MRI) (Slide 1), and computed tomography (CT)-myelogram (Slide 2) available for your review, what is the correct diagnosis in this patient:
Explanation
Question 16
A 75-year-old woman presents with low back pain that is worse with motion and bilateral lower extremity pain that is worse with ambulation. She notes that the pain extends down the posterior aspects of her lower extremities, from the buttocks to the calves. The pain limits her activity â she can only ambulate approximately one block before having to rest. She reports that lumbar flexion, notably leaning over a walker or a shopping cart, considerably diminishes her lower extremity pain. She has a significant past medical history of coronary artery disease, and she has had previous angioplasty of her coronary vessels. On examination, her lower extremity pulses are easily palpable. What would you expect to find on this patientâ s neurological examination:
Explanation
Question 17
A 75-year-old woman presents with low back pain that is worse with motion and bilateral lower extremity pain that is worse with ambulation. She notes that the pain extends down the posterior aspects of her lower extremities, from the buttocks to the calves. The pain limits her activity â she can only ambulate approximately one block before having to rest. She reports that lumbar flexion, notably leaning over a walker or a shopping cart, considerably diminishes her lower extremity pain. She has a significant past medical history of coronary artery disease, and she has had previous angioplasty of her coronary vessels. On examination, her lower extremity pulses are easily palpable. What radiographic evaluation would you obtain to best establish her diagnosis:
Explanation
Question 18
A 75-year-old woman presents with low back pain that is worse with motion and bilateral lower extremity pain that is worse with ambulation. She notes that the pain extends down the posterior aspects of her lower extremities, from the buttocks to the calves. The pain limits her activity â she can only ambulate approximately one block before having to rest. She reports that lumbar flexion, notably leaning over a walker or a shopping cart, considerably diminishes her lower extremity pain. She has a significant past medical history of coronary artery disease, and she has had previous angioplasty of her coronary vessels. On examination, her lower extremity pulses are easily palpable. This patient is diagnosed with degenerative spondylolisthesis with significant lateral recess stenosis. Treatment of this patient could include:
Explanation
Question 19
The distinguishing phenotypic feature that differentiates a schwannoma from a neurofibroma is:
Explanation
Question 20
What is the advantage of performing a magnetic resonance image (MRI) to evaluate spinal tumors:
Explanation
Question 21
Which of the following represents an absolute contraindication to performing a percutaneous vertebroplasty for a painful osteoporotic compression fracture?
Explanation
Question 22
When evaluating an elderly patient with a suspected acute osteoporotic vertebral compression fracture, which MRI sequence is most reliable for differentiating an acute fracture from a chronic, healed deformity?
Explanation
Question 23
Compared to vertebroplasty, balloon kyphoplasty generally offers which of the following biomechanical or procedural advantages?
Explanation
Question 24
What is the most common serious systemic complication associated with the injection of polymethylmethacrylate (PMMA) during vertebroplasty?
Explanation
Question 25
Which anatomic region of the spine is the most common site for osteoporotic vertebral compression fractures?
Explanation
Question 26
Kummell disease is a recognized complication following a vertebral compression fracture. Which of the following best describes its classic radiographic presentation?
Explanation
Question 27
In an elderly patient with severe osteoporosis requiring posterior spinal instrumentation for instability, which technique is most effective for maximizing pedicle screw pullout strength?
Explanation
Question 28
A 75-year-old female presents with multiple severe thoracic osteoporotic compression fractures. Which of the following physiologic consequences is most likely to be found on her clinical evaluation?
Explanation
Question 29
A 72-year-old female presents with severe back pain 2 weeks after a minor fall. Radiographs show a T12 compression fracture with 20% anterior height loss. MRI confirms acute edema without spinal canal compromise. Neurological exam is intact. What is the most appropriate initial management?
Explanation
Question 30
Teriparatide therapy reduces the risk of future vertebral compression fractures primarily through which mechanism of action?
Explanation
Question 31
A 45-year-old male presents with a spontaneous L1 compression fracture. He has no history of trauma, long-term steroid use, or known systemic medical conditions. What is the most critical next step in his medical workup?
Explanation
Question 32
Following an initial osteoporotic vertebral compression fracture, the risk of sustaining a subsequent vertebral fracture at an adjacent level is highest during which time frame?
Explanation
Question 33
Which of the following conditions represents an absolute medical contraindication to initiating oral bisphosphonate therapy in a patient with an osteoporotic compression fracture?
Explanation
Question 34
A major biomechanical consequence of an uncorrected wedge compression fracture in the mid-thoracic spine is:
Explanation
Question 35
The rapid and significant pain relief observed following a successful vertebroplasty is primarily attributed to mechanical stabilization of the microfractures and:
Explanation
Question 36
An 80-year-old female with known osteoporosis presents with severe back pain and an acute L2 compression fracture. Under what specific circumstance would open operative decompression and stabilization be indicated over percutaneous cement augmentation?
Explanation
Question 37
According to the World Health Organization (WHO) criteria, severe (or established) osteoporosis is defined by a fragility fracture and a Dual-energy X-ray absorptiometry (DEXA) T-score of:
Explanation
Question 38
Denosumab is highly effective for patients with severe osteoporosis and recurrent vertebral fractures. What is its precise mechanism of action?
Explanation
Question 39
In a patient with a neurologically intact, acutely painful osteoporotic compression fracture, what is the generally recommended minimum duration for a trial of optimal conservative management before considering vertebroplasty?
Explanation
Question 40
During a percutaneous vertebroplasty, extravasation of PMMA cement into the neural foramen most commonly manifests clinically as:
Explanation
Question 41
Compared to percutaneous vertebroplasty, balloon kyphoplasty has been shown to have which of the following characteristics when used for the treatment of osteoporotic vertebral compression fractures?
Explanation
Question 42
A 75-year-old female presents with severe, unremitting back pain after a fall from standing height. MRI shows an acute L1 compression fracture. She has failed 6 weeks of conservative management. What is an absolute contraindication to performing a vertebroplasty?
Explanation
Question 43
A 72-year-old female sustains a T12 osteoporotic compression fracture. Which of the following MRI sequences is most sensitive for determining whether the fracture is acute or chronic?
Explanation
Question 44
An 80-year-old male presents with acute back pain. Imaging shows a pathological vertebral compression fracture.
Which of the following MRI findings is most indicative of a malignant compression fracture rather than a benign osteoporotic fracture?
Explanation
Question 45
Which medication provides the most rapid, specific analgesic effect for acute osteoporotic vertebral compression fractures within the first few weeks of injury?
Explanation
Question 46
A 68-year-old woman with a T-score of -3.0 sustains a T11 compression fracture. She is started on a daily subcutaneous medication that acts as an anabolic agent to stimulate bone formation. What is the mechanism of action of this medication?
Explanation
Question 47
Following a successful percutaneous vertebroplasty for a painful L1 osteoporotic compression fracture, the patient is at increased risk for developing which of the following complications in the surrounding anatomy?
Explanation
Question 48
A 65-year-old female with osteoporosis is being treated conservatively for a T12 compression fracture. What is the expected role of orthotic bracing (e.g., TLSO or Jewett brace) in this patient?
Explanation
Question 49
In the Denis three-column classification of spinal injuries, a simple osteoporotic compression fracture is typically characterized by failure of which of the following?
Explanation
Question 50
What is the most common anatomical location for osteoporotic vertebral compression fractures?
Explanation
Question 51
During a kyphoplasty for an L2 compression fracture, the surgeon notices a sudden drop in the patient's blood pressure, tachycardia, and a decrease in oxygen saturation immediately after cement injection. What is the most likely cause?
Explanation
Question 52
A 78-year-old patient with severe osteoporosis presents with multiple wedge compression fractures.
According to the World Health Organization (WHO) definition, severe osteoporosis is diagnosed when a patient has a fragility fracture and a DEXA T-score of:
Explanation
Question 53
Which of the following factors most strongly indicates the need for formal surgical decompression and stabilization rather than percutaneous vertebroplasty for an acute osteoporotic vertebral fracture?
Explanation
Question 54
A 55-year-old male sustains an L1 fracture after a fall.
Which plain radiographic finding best differentiates a burst fracture from a simple compression fracture?
Explanation
Question 55
Kümmell disease is an eponym historically used to describe which of the following conditions following a spinal fracture?
Explanation
Question 56
When evaluating a patient's risk for future osteoporotic fractures using the FRAX tool, which of the following is NOT included as a primary variable in the calculation?
Explanation
Question 57
Romosozumab is a newer pharmacological agent used in patients with severe osteoporosis and multiple compression fractures. Its primary mechanism of action is:
Explanation
Question 58
The "intravertebral vacuum cleft sign" seen on radiographs or CT of a vertebral body compression fracture is highly indicative of:
Explanation
Question 59
A 70-year-old male with long-standing ankylosing spondylitis presents with back pain after a minor ground-level fall. Initial plain radiographs of the spine are reported as "unremarkable." What is the most appropriate next step in management?
Explanation
Question 60
For a patient undergoing kyphoplasty for an osteoporotic compression fracture, the polymethylmethacrylate (PMMA) cement should ideally be injected at which of the following consistencies to minimize the risk of venous extravasation?
Explanation
Question 61
A 75-year-old female presents with severe back pain after a fall. Plain radiographs show compression fractures at T11 and L1. Which MRI sequence is most specific for determining which fracture is acute?
Explanation
Question 62
A 68-year-old female presents with progressively worsening back pain 3 months after a minor fall. Radiographs show a T12 compression fracture with an intravertebral vacuum cleft that enlarges on an extension view. What is the most likely diagnosis?
Explanation
Question 63
Compared to percutaneous vertebroplasty, balloon kyphoplasty has been shown to have a lower rate of which of the following complications?
Explanation
Question 64
Which of the following is considered an absolute contraindication to performing a percutaneous vertebroplasty?
Explanation
Question 65
A 72-year-old female sustains an osteoporotic L1 compression fracture. She is neurologically intact but has severe pain. What is the recommended minimum duration of non-operative management prior to considering vertebral augmentation?
Explanation
Question 66
A 74-year-old female undergoes percutaneous vertebroplasty for a T12 compression fracture. Two hours postoperatively, she develops acute dyspnea, tachycardia, and pleuritic chest pain. What is the most likely etiology?
Explanation
Question 67
During the evaluation of a thoracic compression fracture, distinguishing between an osteoporotic etiology and a neoplastic process is critical. Which of the following radiographic findings is highly suspicious for a neoplastic etiology?
Explanation
Question 68
A 70-year-old female undergoes the procedure shown for a painful osteoporotic compression fracture. What is the primary theoretical mechanical advantage of this specific technique over standard cement injection?
Explanation
Question 69
A 65-year-old female with an acute L2 osteoporotic compression fracture is prescribed an orthosis. Which type of orthosis is biomechanically most appropriate for treating this injury?
Explanation
Question 70
A patient with multiple osteoporotic compression fractures is evaluated for teriparatide therapy. This medication is strictly contraindicated in patients with a history of which of the following conditions?
Explanation
Question 71
An elderly patient presents with severe back pain and the characteristic radiographic finding shown. Advanced imaging confirms a fluid-filled cleft within the vertebral body. Which of the following best explains the pathogenesis of this specific finding?
Explanation
Question 72
During a percutaneous vertebroplasty, what volume of PMMA injection is generally sufficient to achieve significant pain relief and stabilization in a typical thoracolumbar vertebral body?
Explanation
Question 73
A 71-year-old female presents with bilateral lower extremity weakness and hyperreflexia following a fall. Imaging shows a T8 osteoporotic compression fracture with retropulsion of bone causing severe spinal cord compression. What is the most appropriate management?
Explanation
Question 74
A well-documented complication following vertebral augmentation procedures is adjacent segment vertebral fracture. What is the most widely accepted biomechanical mechanism contributing to this complication?
Explanation
Question 75
During the vertebroplasty procedure shown, the surgeon visualizes sudden extravasation of cement tracking into the posterior epidural space on lateral fluoroscopy. What is the immediate next best step?
Explanation
Question 76
Which medical therapy has been shown to uniquely provide acute analgesic effects for osteoporotic vertebral compression fractures, in addition to its anti-resorptive properties?
Explanation
Question 77
When evaluating a patient with a suspected atraumatic osteoporotic compression fracture, obtaining which of the following laboratory values is critical to rule out multiple myeloma as a secondary cause?
Explanation
Question 78
The polymethylmethacrylate (PMMA) utilized in percutaneous vertebroplasty has which of the following distinct properties when compared to standard joint arthroplasty cement?
Explanation
Question 79
A 66-year-old female sustains a simple anterior wedge compression fracture of L1 with 20% height loss and no neurologic deficits. According to Denis' three-column spine concept, which columns are disrupted in this injury pattern?
Explanation
Question 80
An 80-year-old woman presents with acute back pain after lifting a box. Radiographs reveal a T12 compression fracture. What is the most appropriate initial management?
Explanation
Question 81
What is an absolute contraindication to performing a percutaneous vertebroplasty for an osteoporotic compression fracture?
Explanation
Question 82
A 75-year-old female with an acute osteoporotic compression fracture is prescribed an intranasal medication that provides both antiresorptive effects and analgesic properties for acute bone pain. What is the mechanism of action of this medication?
Explanation
Question 83
Which MRI sequence is most useful to differentiate an acute osteoporotic compression fracture from a chronic, healed compression fracture?
Explanation
Question 84
A 72-year-old male with a history of prostate cancer presents with a T8 compression fracture. Which of the following MRI findings most strongly suggests a pathologic fracture rather than a benign osteoporotic fracture?
Explanation
Question 85
Compared to percutaneous vertebroplasty, balloon kyphoplasty for the treatment of vertebral compression fractures is associated with:
Explanation
Question 86
A 68-year-old female undergoes a multilevel vertebroplasty. During the procedure, the patient suddenly develops tachycardia, hypotension, and hypoxia. What is the most likely cause?
Explanation
Question 87
In a patient with an osteoporotic vertebral compression fracture, what is the clinical significance of the intravertebral vacuum cleft sign (Kümmell disease)?
Explanation
Question 88
Which of the following factors most significantly increases the risk of an adjacent level fracture following percutaneous vertebroplasty?
Explanation
Question 89
A 45-year-old male falls from a height and sustains an L1 burst fracture with 40% canal compromise. He is neurologically intact, and MRI confirms an intact posterior ligamentous complex (PLC). What is the most appropriate management?
Explanation
Question 90
Look at the image provided
. In the setting of an acute traumatic spinal fracture, what is the primary purpose of meticulously assessing the posterior vertebral body wall on imaging?
Explanation
Question 91
What is the incidence of significant neurologic deficit directly associated with a simple, benign osteoporotic wedge compression fracture?
Explanation
Question 92
In the evaluation of a patient with long-standing ankylosing spondylitis who sustains a minor fall,
what is the classic fracture pattern expected?
Explanation
Question 93
A patient with a history of a distal radius fragility fracture sustains a vertebral compression fracture. Bone mineral density (BMD) testing reveals a T-score of -3.0. According to WHO criteria, this strictly defines:
Explanation
Question 94
Teriparatide is being considered for a patient with severe osteoporosis and multiple painful compression fractures. Which of the following is a recognized absolute contraindication to its use?
Explanation
Question 95
What is the primary mechanism of injury responsible for producing a Chance fracture of the thoracolumbar spine?
Explanation
Question 96
During a balloon kyphoplasty for an L2 compression fracture
, the surgeon notes a cortical breach of the medial pedicle wall during trocar advancement. What is the most immediate critical concern?
Explanation
Question 97
Which biomechanical change most directly accounts for the exponentially increased risk of adjacent vertebral compression fractures following severe kyphosis in the osteoporotic spine?
Explanation
Question 98
A 55-year-old male with known Diffuse Idiopathic Skeletal Hyperostosis (DISH) suffers a minor fall from standing and complains of new, severe back pain. Initial plain radiographs are reported as unremarkable. What is the most appropriate next step in management?
Explanation
Question 99
When comparing conservative treatment to percutaneous vertebroplasty for acute osteoporotic vertebral compression fractures, key randomized blinded controlled trials (e.g., INVEST and Buchbinder trials) have historically demonstrated:
Explanation
None
