Orthopedic Prometric MCQs - Chapter 3 Part 19
Orthopedic Prometric MCQs - Chapter 3 Part 19
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following groups is not at increased risk for community- acquired methicillin-resistant Staphylococcus aureus (C AMRSA):
Explanation
Question 2
Which of the following toxins is responsible for the virulence of community- acquired methicillin-resistant Staphylococcus aureus (C A-MRSA):
Explanation
Question 3
A 5-year-old girl presents to the emergency department with pain in her hip. Her temperature is 102° F, pulse is 96, and blood pressure is 104/60. Magnetic resonance imaging reveals edema in the obturator muscles. Blood cultures are negative. Ultrasound-guided aspiration reveals no abscess, but fluid obtained grows methicillin-resistant Staphylococcus aureus (MRSA). In addition to antibiotic treatment, what other treatment option is recommended:
Explanation
Question 4
A 5-year-old girl who presents to the emergency department has obturator muscle infection without abscess formation, which is seen on magnetic resonance imaging. She has no clinical evidence of sepsis. Aspiration yields methicillin-resistant Staphylococcus aureus (MRSA). Which of the following antibiotics is recommended:
Explanation
Question 5
A nonverbal 12-year-old patient with totally involved cerebral palsy and developmental delay has been in pain for the past week. The source of the pain cannot be localized. Pelvis radiographs and urinalysis are unremarkable. The next recommended study is:
Explanation
Question 6
A 2-month-old infant has a midshaft humeral fracture. The fracture has 45° angulation with an anterolateral apex and is 6 mm short. Recommended treatment includes:
Explanation
Question 7
A 23-month-old patient demonstrates intoeing. He walked at 21 months. His height is in the 3rd quantile, and he is cognitively normal. Possible diagnoses include all of the following except:
Explanation
Question 8
The most common form of rickets in the United States is:
Explanation
Question 9
The gene most likely to be associated with inherited rickets is:
Explanation
Question 10
Genetic testing performed for a patient reveals a defect in PHEX. The family history provided by the patient is most likely to include:
Explanation
Question 11
A toddler with bowing is suspected of X-linked hypophosphatemic rickets (XLH). The most likely laboratory abnormalities will include:
Explanation
Question 12
An 18-month-old patient is suspected of X-linked hypophosphatemic rickets. The clinical findings are most likely to include all of the following except:
Explanation
Question 13
A newborn is brought in for consultation due to a foot deformity. The left foot is dorsiflexed at the ankle, and the dorsum of the foot is able to be placed against the tibia. Neurologic and vascular examination is normal. Recommended treatment includes:
Explanation
Question 14
In a newborn, how much angulation is acceptable in a fracture of the humeral diaphysis:
Explanation
Question 15
Which of the following radiographic parameters remains essentially fixed throughout life:
Explanation
Question 16
A 6-year-old boy presents with a linear area of swelling in the region of the posterior paraspinous muscles. He has no history of weight loss or fevers. He also has bilateral great toe deformities consisting of valgus and shortening. The most likely diagnosis is:
Explanation
Question 17
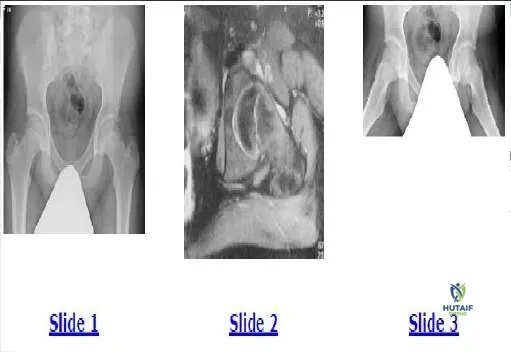
Based on the presented radiographs (Slide 1, Slide 2), what is the proper diagnosis of this 12-month-old female patient:
Explanation
Question 18
A 23-month-old patient is evaluated for intoeing. Based on his radiograph (Slide), what is the most likely diagnosis:
Explanation
Question 19
A 13-year-old boy has been experiencing hip pain for 1 month. The pain is worse with activity. The patient has no history of fever or weight loss, and both of his hips flex to 90°. Based on his radiograph (Slide 1) and magnetic resonance image (Slide 2), which of the following is the most likely diagnosis:
Explanation
Question 20
A 13-year-old boy has been experiencing hip pain for 1 month. The pain is worse with activity. The patient has no history of fever or weight loss, and both of his hips flex to 90°. , which of the following is the most likely diagnosis:
Explanation
Question 21
An 8-year-old boy has acute hematogenous osteomyelitis caused by community-acquired MRSA (CA-MRSA). Sensitivity testing shows the isolate is susceptible to clindamycin but resistant to erythromycin. Which test must be performed before initiating clindamycin therapy?
Explanation
Question 22
A 2-year-old child presents with a swollen, erythematous knee. Joint aspiration yields purulent fluid, but standard agar cultures are negative at 48 hours. What is the most appropriate method to identify the most likely atypical causative organism in this age group?
Explanation
Question 23
A 7-year-old boy presents with a limp, fever, and inability to bear weight. Hip range of motion is slightly limited at the extremes but relatively painless in the mid-arc. Inflammatory markers are elevated. MRI reveals abnormal marrow signal in the ilium.
What is the most appropriate initial management for uncomplicated acute pelvic osteomyelitis?
Explanation
Question 24
Methicillin resistance in Staphylococcus aureus (MRSA) is primarily mediated by which of the following molecular mechanisms?
Explanation
Question 25
Community-acquired MRSA (CA-MRSA) strains frequently produce a specific toxin that is highly associated with severe deep tissue infections and necrotizing pneumonia. Which toxin is this?
Explanation
Question 26
A 3-week-old neonate presents with a septic hip. Pending culture results, which of the following empiric intravenous antibiotic regimens is most appropriate?
Explanation
Question 27
A 6-year-old child with sickle cell disease presents with femoral osteomyelitis. While Staphylococcus aureus is highly prevalent, which organism is uniquely responsible for a disproportionately high percentage of osteomyelitis cases in this specific patient population?
Explanation
Question 28
According to the Kocher criteria, what is the predictive probability of septic arthritis in a child who presents with a fever of 38.6 degrees C, inability to bear weight, ESR of 45 mm/hr, and a serum WBC count of 13,000 cells/mm3?
Explanation
Question 29
A 9-year-old girl presents with recurrent episodes of clavicular and tibial pain. Radiographs show sclerotic and lytic lesions. Multiple bone biopsies have yielded no bacterial growth, and she has not responded to prolonged IV antibiotics. What is the most appropriate next step in management?
Explanation
Question 30
A 7-year-old boy from Massachusetts presents with a massive, painless right knee effusion. He is afebrile and active. Joint aspiration yields a WBC count of 45,000 cells/mm3 (predominantly neutrophils), but Gram stain is negative. What is the most appropriate diagnostic test?
Explanation
Question 31
An infant is diagnosed with septic arthritis of the hip. An emergent open arthrotomy is planned. Which surgical approach is most commonly utilized to provide safe and direct access to the pediatric hip joint?
Explanation
Question 32
A 14-year-old boy with a localized MRSA abscess develops sudden onset high fever, hypotension, and a diffuse macular erythroderma. Labs reveal acute kidney injury. This shock syndrome is mediated by which of the following mechanisms?
Explanation
Question 33
A 12-year-old boy presents with chronic, mild lower leg pain that worsens at night. Radiographs demonstrate a 2 cm radiolucent lesion in the distal tibial metaphysis with a thick rim of reactive sclerosis. Inflammatory markers are normal. What is the most likely diagnosis?
Explanation
Question 34
A 5-year-old child is treated for uncomplicated acute hematogenous osteomyelitis of the femur. After a week of intravenous antibiotics, the child is afebrile, and the CRP has normalized. What is the currently recommended total duration of antibiotic therapy (IV plus oral step-down)?
Explanation
Question 35
A patient with confirmed active pulmonary tuberculosis develops an acute, sterile polyarthritis primarily affecting the knees and ankles. Joint aspirates show no evidence of direct mycobacterial invasion. What is the term for this specific reactive arthritis?
Explanation
Question 36
An 8-year-old girl is ready for discharge following surgical drainage of a CA-MRSA soft tissue abscess. She is prescribed an oral step-down antibiotic. Which of the following is an appropriate oral agent for MRSA that does NOT require routine monitoring for myelosuppression?
Explanation
Question 37
Which of the following is NOT one of the classic Kocher criteria used to differentiate septic arthritis of the hip from transient synovitis in children?
Explanation
Question 38
A 2-year-old girl presents with a warm, swollen knee and refusal to walk. Aspiration yields purulent synovial fluid, but standard agar cultures remain sterile at 48 hours. What is the optimal method for isolating the most likely causative organism in this age group?
Explanation
Question 39
A 9-year-old boy presents with severe right thigh pain, fever, and inability to bear weight.
MRI reveals a large subperiosteal abscess. If blood cultures grow Community-Acquired MRSA (CA-MRSA), which of the following complication screening protocols is highly recommended?
Explanation
Question 40
A 10-year-old boy develops osteomyelitis of the calcaneus after stepping on a rusty nail that penetrated his rubber-soled sneaker. Which organism must be specifically covered by empiric antibiotic therapy?
Explanation
Question 41
A 6-year-old girl with sickle cell disease presents with high fever, severe right arm pain, and localized swelling over the humerus. Which of the following is the most appropriate empiric antibiotic regimen while awaiting cultures?
Explanation
Question 42
A 2-week-old neonate is brought to the clinic for decreased spontaneous movement of the left arm. She is afebrile with normal inflammatory markers. Examination reveals crying with passive motion of the shoulder. What is the most likely diagnosis?
Explanation
Question 43
A 9-year-old girl has a 6-month history of recurrent multifocal bone pain. Radiographs show lytic lesions with sclerotic borders in her clavicle and distal femur. Multiple bone biopsies have shown only sterile acute and chronic inflammation. Which of the following is the recommended initial management?
Explanation
Question 44
In children, the blood supply to the epiphysis directly communicates with metaphyseal vessels across the physis. This transphyseal vascular connection, which allows metaphyseal osteomyelitis to easily spread into the joint, typically obliterates by what age?
Explanation
Question 45
A 3-year-old boy presents with refusal to walk and a recent history of irritability. He refuses to pick up toys from the floor and maintains a rigidly straight back. ESR is elevated, but WBC is normal. What is the most accurate diagnostic imaging modality for the suspected condition?
Explanation
Question 46
The Panton-Valentine leukocidin (PVL) toxin is a major virulence factor in Community-Acquired MRSA. What is its primary pathogenic mechanism in orthopedic infections?
Explanation
Question 47
A 16-year-old female presents with acute knee swelling, migratory polyarthralgia, and painless vesiculopustular skin lesions on her extremities. Gram stain of the synovial fluid is likely to reveal which of the following?
Explanation
Question 48
A 13-year-old boy complains of dull, aching pain in his distal tibia, which frequently wakes him at night and is relieved by ibuprofen. MRI demonstrates a metaphyseal intraosseous abscess with a hyperintense inner ring on T1-weighted imaging. What is this MRI finding called?
Explanation
Question 49
A 14-year-old is prescribed a prolonged 6-week course of oral linezolid for a complex MRSA osteomyelitis. Which of the following complications requires routine monitoring during the duration of therapy?
Explanation
Question 50
A 7-year-old boy from Massachusetts presents with a swollen, warm right knee, but no fever or signs of systemic toxicity. He has full range of motion of the knee without severe pain. What is the most appropriate initial diagnostic test for the suspected etiology?
Explanation
Question 51
A 10-year-old boy presents with fever, limp, and severe tenderness over his mid-thigh. MRI reveals a large, rim-enhancing fluid collection within the vastus intermedius, but the adjacent femoral marrow shows normal signal intensity. What is the most common causative organism for this condition in temperate climates?
Explanation
Question 52
In a child being treated for uncomplicated acute hematogenous osteomyelitis (AHO) with intravenous antibiotics, which of the following criteria is most widely accepted for safely transitioning to oral antibiotics?
Explanation
Question 53
A 9-year-old girl presents with vague buttock pain, fever, and a noticeable limp. Hip range of motion is full but painful at the extremes, and the FABER test is markedly positive. Plain radiographs are normal. What is the most appropriate next step in management?
Explanation
Question 54
Kingella kingae is a common cause of pediatric septic arthritis. A thorough history from the parents of an affected child will most likely reveal which of the following antecedent events?
Explanation
Question 55
Rapid destruction of articular cartilage in bacterial septic arthritis of the hip is primarily caused by which of the following mechanisms?
Explanation
Question 56
When interpreting culture susceptibilities for a methicillin-resistant Staphylococcus aureus (MRSA) isolate from a pediatric osteomyelitis case, a positive "D-zone test" indicates which of the following?
Explanation
Question 57
Community-acquired MRSA is characterized by the presence of Panton-Valentine leukocidin (PVL). What is the primary mechanism of action of this virulence factor?
Explanation
Question 58
Community-acquired MRSA (CA-MRSA) typically contains which of the following staphylococcal cassette chromosome mec (SCCmec) elements compared to hospital-acquired MRSA (HA-MRSA)?
Explanation
Question 59
A 9-year-old boy with severe community-acquired MRSA (CA-MRSA) tibial osteomyelitis experiences persistent tachycardia and swelling in the affected limb despite adequate surgical debridement and IV vancomycin. What is the most likely associated complication?
Explanation
Question 60
A 2-year-old child presents with an acute monoarticular knee effusion, low-grade fever, and refusal to bear weight. Aspiration yields purulent fluid, but standard agar plates show no growth at 48 hours. Which of the following is the most appropriate method to isolate the most likely causative organism?
Explanation
Question 61
A 15-year-old female develops rapid-onset fever, hypotension, and a diffuse macular erythroderma following knee arthroscopy. Blood cultures are sterile. The condition is mediated by a toxin that exerts its effect through which of the following mechanisms?
Explanation
Question 62
A 2-week-old neonate presents with irritability, poor feeding, and pseudoparalysis of the right lower extremity. Ultrasound shows a right hip effusion. Aspiration reveals purulent fluid. Empiric antibiotic coverage must include agents effective against Staphylococcus aureus and which of the following organisms?
Explanation
Question 63
Which of the following laboratory parameters is a component of the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score?
Explanation
Question 64
A 14-year-old boy is recovering from an uncomplicated CA-MRSA skin and soft tissue infection that was surgically drained. He is to be discharged on oral antibiotics. The isolate is sensitive to trimethoprim-sulfamethoxazole, clindamycin, and tetracyclines. Which of the following antibiotics is known to also inhibit bacterial toxin production?
Explanation
Question 65
A 7-year-old boy presents with a 3-day history of fever, limp, and severe right thigh pain. Blood cultures are drawn.
Based on the likely diagnosis of deep infection, what is the most appropriate next step in management after initiating empiric antibiotics?
Explanation
Question 66
In chronic orthopedic implant infections, Staphylococcus epidermidis evades host defenses primarily through the production of a glycocalyx biofilm. Which of the following phases of biofilm formation involves "quorum sensing"?
Explanation
Question 67
A 6-year-old child with sickle cell disease presents with bilateral tibial pain and fever. Ultrasound shows no subperiosteal fluid collections. Blood cultures are pending. Which of the following imaging modalities is most specific for differentiating acute osteomyelitis from bone infarction in this patient?
Explanation
Question 68
A sexually active 21-year-old female presents with migratory polyarthralgia, tenosynovitis of the wrist, and sparse painless pustular skin lesions. Joint aspiration of her knee yields a WBC count of 45,000 cells/mm3. Gram stain is negative. What is the most common underlying host defect associated with disseminated infection by this organism?
Explanation
Question 69
A 9-year-old boy from Connecticut presents with a massive, minimally painful effusion of his right knee. He denies recent trauma or fever. He had a transient rash on his thigh six months ago. Which of the following is the standard two-tiered testing protocol to confirm the diagnosis?
Explanation
Question 70
A 25-year-old construction worker stepped on a rusty nail that penetrated deeply through the rubber sole of his work boot into his foot. Seven days later, he develops signs of osteomyelitis of the calcaneus. In addition to S. aureus, which organism must be covered by empiric antibiotics?
Explanation
Question 71
Which of the following complications is significantly more common in pediatric osteomyelitis caused by community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) compared to methicillin-sensitive Staphylococcus aureus (MSSA)?
Explanation
Question 72
In acute hematogenous osteomyelitis in a young child, what anatomical feature of the metaphyseal blood vessels strongly predisposes the metaphysis to bacterial seeding?
Explanation
Question 73
A 6-year-old child presents with a 4-day history of right thigh pain and high fever. Plain radiographs are unremarkable. An MRI is obtained.
Blood cultures are pending. Which of the following strictly dictates the need for urgent surgical debridement in this patient's condition?
Explanation
Question 74
A 4-year-old boy presents with a limp and right hip pain. He is afebrile (37.2°C) but refuses to bear weight on the right leg. Laboratory tests show a WBC of 10,500/mm3 and an ESR of 22 mm/hr. What is the approximate probability of septic arthritis according to the Kocher criteria?
Explanation
Question 75
An 8-year-old girl with homozygous sickle cell disease presents with fever and severe tibial pain. Blood cultures are drawn. Empiric antibiotic therapy should ideally include robust coverage for which two most common organisms in this specific population?
Explanation
Question 76
A 14-month-old child presents with acute onset of a limp and a swollen left knee. Arthrocentesis yields purulent fluid with 65,000 WBCs, but routine Gram stain and standard cultures are negative at 48 hours. Which of the following fastidious organisms is the most likely culprit?
Explanation
Question 77
A 10-year-old girl presents with recurrent episodes of multifocal bone pain. Radiographs reveal lytic lesions with sclerotic borders in the clavicle and distal tibia. Biopsy shows sterile, non-specific inflammation. Which of the following is the most appropriate initial treatment?
Explanation
Question 78
A 3-year-old boy presents with refusal to walk and crying when placed in a sitting position. He is afebrile. Examination shows loss of lumbar lordosis but no focal neurologic deficits. Radiographs of the spine are normal. What is the most appropriate next step in diagnostic imaging?
Explanation
Question 79
A 2-week-old neonate in the NICU is noted to have a swollen, immobile right shoulder. Ultrasound confirms an effusion, and aspiration is planned. In addition to Staphylococcus aureus, which organism is a highly prominent cause of septic arthritis specifically in this age group?
Explanation
Question 80
What is the primary pathophysiological mechanism leading to the development of avascular necrosis (AVN) of the femoral head following neglected septic arthritis of the infant hip?
Explanation
Question 81
In a 7-year-old child being treated for acute hematogenous osteomyelitis, which inflammatory marker is most useful for evaluating the response to antibiotic therapy and guiding the transition from intravenous to oral medications?
Explanation
Question 82
A 7-year-old boy presents with a massive knee effusion and a slight limp, but he retains full range of motion with only minimal pain. He is afebrile. Which of the following findings most strongly differentiates Lyme arthritis from pyogenic septic arthritis?
Explanation
Question 83
A 12-year-old steps on a rusty nail that pierces his rubber-soled sneaker, subsequently developing osteomyelitis in the foot. Following surgical debridement, what is the most appropriate empiric oral antibiotic choice for the most likely organism?
Explanation
Question 84
A 16-year-old male presents with dull, aching pain in his distal tibia for several months, typically worse at night. Radiographs show a well-circumscribed, radiolucent lesion with a thick sclerotic margin in the metaphysis. What is the most likely diagnosis?
Explanation
Question 85
When performing an ultrasound-guided anterior aspiration of the hip joint in a child for suspected septic arthritis, which important neurovascular structure lies immediately medial to the optimal needle trajectory?
Explanation
Question 86
A 5-year-old boy is brought to the ER with rapid onset of severe leg pain, fever, and lethargy following a minor skin abrasion. The skin is tense, erythematous, and exquisitely tender beyond the visible margins of redness. What is the most critical initial step in management?
Explanation
Question 87
A sexually active 17-year-old female presents with migratory polyarthralgias, pain along the flexor tendons of the wrist, and a few discrete pustular skin lesions on her extremities. She is afebrile. What is the most likely causative organism?
Explanation
None
