Orthopedic Prometric MCQs - Chapter 3 Part 18
Orthopedic Prometric MCQs - Chapter 3 Part 18
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
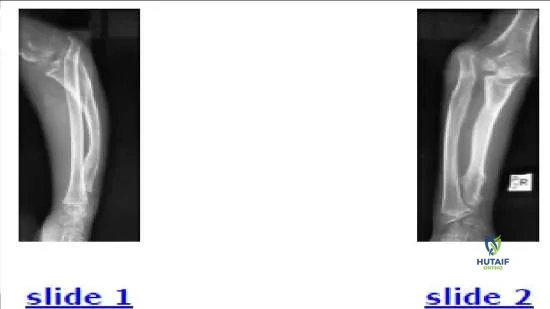
The parents of a 12-year-old boy notice an abnormal shape on their sonâ s forearm. He states that he does not feel any pain. Based on his radiograph (Slide), the most likely diagnosis is:
Explanation
Question 2
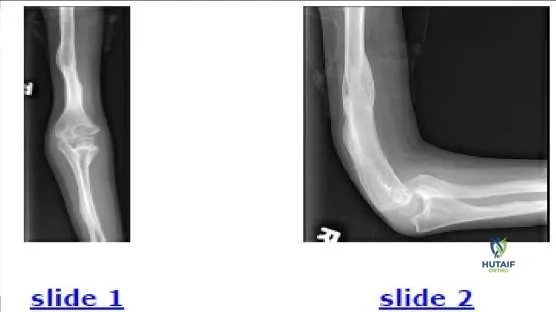
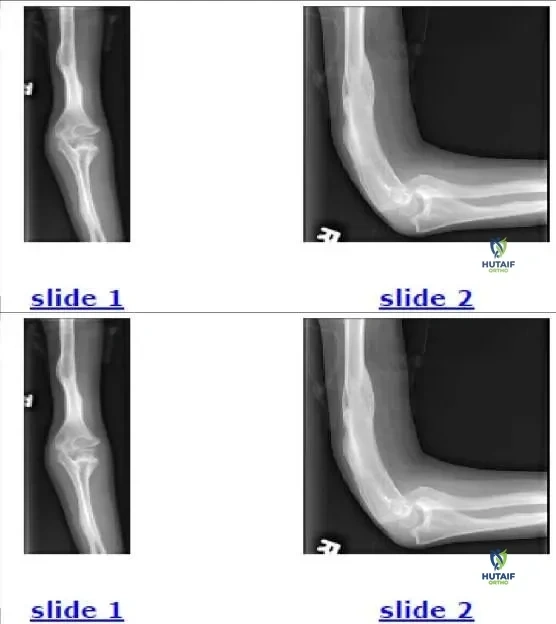
The 9-year-old patient presented in the radiographs (Slide 1, Slide 2) should be diagnosed with:
Explanation
and brother also have the condition bilaterally) as well as heterotopic calcification, osseous fragility, and scoliosis. Dislocation of the radial head occurs less often (0%-29%) in the other types of osteogenesis imperfecta and is linked to angular deformation of the long bones. The signs of osteogenesis imperfecta in this patient include thin long bones, several healed fractures, and angular deformations.
Question 3
Which has a lower risk of compartment syndrome or delayed detection in a patient with a supracondylar fracture of the humerus:
Explanation
Question 4
In a lateral radiograph of a childâ s elbow, the anterior humeral line should be located:
Explanation
Question 5
A 3-year-old boy falls on his upper extremity and shows sign of pain. His radiograph only shows a posterior fat pad sign of the elbow. What is the most likely diagnosis:
Explanation
Question 6
Which of the following is not an indication to urgently treat a supracondylar humerus fracture:
Explanation
Question 7
The lung attains half of its adult volume at what age:
Explanation
Question 8
Which of the following conditions is not associated with an increased risk of cavus foot:
Explanation
Question 9
Which of the following factors has not been proven to increase the risk of thermal necrosis to a limb with a cast:
Explanation
Question 10
Which shape of the olecranon apophysis correlates most closely with closure of the triradiate cartilage of the hips:
Explanation
Question 11
A 15-year-old female patient undergoes spine fusion from T2 to the pelvis for scoliosis associated with cerebral palsy. Her past medical history is remarkable for seizure disorder, ventriculoperitoneal shunt, baclofen pump, and gastrostomy tube. Her postoperative course is complicated by disorientation and visual hallucinations on postoperative day 3, whereas she had been communicative preoperatively. The most likely cause of this change is:
Explanation
Question 12
A 5-year-old patient with Legg-Calva-Perthes disease has lateral pillar B involvement. He has 15% epiphyseal extrusion. Treatment should consist of:
Explanation
Question 13
Which of the following characteristics is more commonly found in patients with Meyer dysplasia than in patients with Legg- C alvé-Perthes disease:
Explanation
Question 14
A 10-year-old girl is seen for limb-length inequality. She has 10° of valgus of the left knee and a shortened left fibula. Her projected shortening at maturity is 1 cm in the left femur and 2.1 cm in the left tibia. Her left foot is normal in shape but one-half size smaller than the right. Her overall height and maturity are at the median for her age. For this patient, recommended treatment for limb-length inequality is:
Explanation
Question 15
Which of the following is an accurate mean age for a motor milestone:
Explanation
Question 16
In the workup of scoliosis, what is/are the best method(s) to assess skeletal maturity during a patients peak height velocity (Risser grade 0):
Explanation
Question 17
Following triple arthrodesis, total ankle range of motion is:
Explanation
Question 18
Three years ago, a 20-year-old female patient underwent posterior spinal fusion for adolescent idiopathic scoliosis. She asks what would happen if the implants were removed. The surgeons most likely response will be:
Explanation
Question 19
Which of the following factors best predicts the risk of disk degeneration in young adults:
Explanation
Question 20
Which of the following treatments decreases hip subluxation in patients with cerebral palsy who have displaced hips:
Explanation
Question 21
A 6-year-old child presents with a pink, pulseless hand following a displaced supracondylar humerus fracture. After closed reduction and percutaneous pinning, the hand remains pink and pulseless. What is the next best step in management?
Explanation
Question 22
A 5-year-old sustains an isolated fracture of the proximal ulna. Radiographs reveal an anterior dislocation of the radial head. This injury is best classified as which Bado type?
Explanation
Question 23
In a pediatric patient with a displaced lateral condyle humerus fracture, which of the following is the most significant clinical risk if the fracture fails to unite?
Explanation
Question 24
Which of the following is an absolute indication for operative intervention in a pediatric medial epicondyle fracture?
Explanation
Question 25
A 7-year-old falls on an outstretched hand and sustains a radial neck fracture. Up to what degree of angulation is generally acceptable for non-operative management without manipulative reduction in this age group?
Explanation
Question 26
Which of the following pediatric physeal fractures carries the highest rate of premature physeal closure and subsequent growth arrest?
Explanation
Question 27
Based on the typical mechanism for pediatric lateral condyle fractures, which muscle group is responsible for the distraction and rotational displacement of the fracture fragment?
Explanation
Question 28
A 12-year-old boy presents with an altered gait and thigh pain. If the underlying diagnosis is Slipped Capital Femoral Epiphysis (SCFE), what is the anatomical direction of the epiphyseal slip relative to the femoral neck?
Explanation
Question 29
A 3-year-old child presents with progressive bowing of the legs. Radiographs demonstrate changes at the proximal medial tibia. Which radiographic measurement is most useful in differentiating infantile Blount disease from physiological bowing?
Explanation
Question 30
During the Ponseti serial casting technique for idiopathic clubfoot, which component of the deformity is corrected last?
Explanation
Question 31
During an open reduction of a Developmentally Dysplastic Hip (DDH) via a medial (Ludloff) approach in an 11-month-old, which structure is directly released to allow access to the joint and facilitate reduction?
Explanation
Question 32
A 4-month-old infant in a Pavlik harness for DDH develops an inability to actively extend the knee. This complication is most likely due to:
Explanation
Question 33
According to the Kocher criteria, which of the following is one of the independent predictors used to differentiate septic arthritis from transient synovitis of the hip in a pediatric patient?
Explanation
Question 34
Which of the following is considered the most significant poor prognostic factor in Legg-Calvé-Perthes disease?
Explanation
Question 35
A juvenile Tillaux fracture involves an avulsion of the anterolateral distal tibial epiphysis. Which ligament is primarily responsible for this avulsion?
Explanation
Question 36
A 13-year-old sustains a twisting ankle injury. Radiographs reveal a fracture that appears as a Salter-Harris III on the AP view and a Salter-Harris II on the lateral view. What is the most likely diagnosis?
Explanation
Question 37
A child presenting with frequent fractures, blue sclerae, and dentinogenesis imperfecta is diagnosed with Osteogenesis Imperfecta. This condition is primarily caused by a defect in the synthesis of:
Explanation
Question 38
Which of the following genetic inheritance patterns and underlying mutations most accurately describes Achondroplasia?
Explanation
Question 39
A 6-year-old child sustains a posteromedially displaced supracondylar fracture of the humerus. Which nerve is most frequently injured due to this specific displacement pattern?
Explanation
Question 40
A 14-year-old girl presents with progressive wrist pain and limited range of motion. Examination reveals a prominent distal ulna and volar subluxation of the hand. The failure of growth in this specific deformity primarily occurs at which aspect of the distal radius?
Explanation
Question 41
Evaluate the provided clinical image.
A 13-year-old female presents with bilateral wrist deformities. What is the standard surgical intervention for symptomatic, severe manifestations of this condition when a Vickers ligament is identified?
Explanation
Question 42
An 8-year-old boy presents with an isolated pediatric lateral condyle fracture of the humerus. Radiographs show a Milch Type II fracture with 3 mm of displacement. What is the most appropriate management?
Explanation
Question 43
A 7-year-old sustains a traumatic fall. Radiographs demonstrate an anterior dislocation of the radial head with an associated diaphyseal fracture of the ulna that is apex-anterior. Which nerve palsy is most commonly associated with this specific injury pattern?
Explanation
Question 44
A 9-year-old boy presents with an obvious cubitus varus deformity 2 years after conservative management of a supracondylar humerus fracture. What is the primary pathophysiologic cause of this late deformity?
Explanation
Question 45
In treating a 10-year-old with a radially displaced and angulated radial neck fracture, at what degree of initial angulation is reduction definitively indicated to prevent significant loss of forearm rotation?
Explanation
Question 46
A 12-year-old baseball pitcher presents with chronic medial elbow pain. Radiographs reveal widening of the medial epicondylar apophysis. The biomechanical mechanism responsible for this condition is primarily:
Explanation
Question 47
Based on the elbow radiograph of a 5-year-old child presenting with acute trauma (
), what is the most significant long-term complication if a widely displaced lateral condyle fracture goes entirely unrecognized and develops into a nonunion?
Explanation
Question 48
A 3-year-old toddler is pulled by the arm by a sibling and subsequently refuses to use the right upper extremity, holding it in slight flexion and pronation. Which anatomic structure is primarily interposed in the joint in this condition?
Explanation
Question 49
A newborn is diagnosed with bilateral radial clubhands. Which of the following laboratory investigations is most critical to perform early to rule out a potentially fatal condition associated with this deformity?
Explanation
Question 50
A newborn has absent radii bilaterally, but both thumbs are distinctly present and well-formed. Blood tests reveal profound thrombocytopenia. This clinical picture is most characteristic of which syndrome?
Explanation
Question 51
A 14-year-old boy with a known diagnosis of Multiple Hereditary Exostoses (MHE) presents with a progressive forearm deformity. Which of the following describes the most classic forearm deformity seen in these patients?
Explanation
Question 52
What is the maximum acceptable angulation for a midshaft both-bone forearm fracture in a 5-year-old child?
Explanation
Question 53
A 13-year-old gymnast sustains a dislocated elbow with an associated medial epicondyle fracture. Following closed reduction of the elbow joint, what is the absolute indication for open reduction and internal fixation of the medial epicondyle?
Explanation
Question 54
A 5-year-old sustains a completely displaced supracondylar humerus fracture. On arrival, the hand is pink but the radial pulse is absent. After successful closed reduction and pinning, the hand remains pink and warm with a capillary refill of 2 seconds, but the pulse remains absent. What is the most appropriate next step?
Explanation
Question 55
A 6-year-old girl is evaluated for asymmetric shoulder height. Examination reveals a high, hypoplastic left scapula with restricted shoulder abduction. Which of the following conditions is most frequently associated with this deformity?
Explanation
Question 56
A patient presents with generalized hypermobility, a delayed closure of fontanelles, and the ability to appose the shoulders anteriorly at the midline. This disorder is most commonly caused by a mutation in which gene?
Explanation
Question 57
Congenital pseudarthrosis of the clavicle is characterized by an absence of a history of trauma and presents as a painless mass. In nearly all typical cases without dextrocardia (situs inversus), which side is predominantly affected?
Explanation
Question 58
A 4-year-old sustains a trauma to the forearm. Radiographs demonstrate an accentuated bowing of the ulna without an obvious cortical breach, and an anterior dislocation of the radial head. The initial step in the reduction maneuver for the ulnar plastic deformation should involve:
Explanation
Question 59
A 6-year-old boy falls from the monkey bars and sustains a completely displaced extension-type supracondylar fracture of the humerus. On physical examination, he is unable to make an "A-OK" sign with his thumb and index finger. Sensation in the hand is intact. Which nerve is most likely injured?
Explanation
Question 60
A 5-year-old girl sustains a severely displaced supracondylar humerus fracture. Her hand is pink and well-perfused, but the radial pulse is absent on palpation. After closed reduction and percutaneous pinning, the hand remains pink and warm, but the pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 61
A 12-year-old boy presents with painless, hard, fixed masses near his distal radius and proximal tibia, along with progressive forearm bowing.
What is the most likely underlying genetic mechanism for his condition?
Explanation
Question 62
Which of the following is an absolute indication for open reduction and internal fixation of a medial epicondyle fracture in a 10-year-old child?
Explanation
Question 63
A 4-year-old child sustains a lateral condyle fracture of the humerus. The fracture is displaced by 4 mm. If left untreated, what is the most common long-term clinical deformity and potential neurological complication?
Explanation
Question 64
A 7-year-old child sustains a both-bone forearm fracture. During the remodeling process over the next few years, which of the following deformities has the LEAST potential to remodel?
Explanation
Question 65
A 6-year-old boy falls on an outstretched hand and sustains a Monteggia fracture-dislocation.
According to the Bado classification, which type is most common in the pediatric population and what is the direction of the radial head dislocation?

Explanation
Question 66
A 3-year-old girl is brought to the clinic because she keeps her right elbow partially flexed and pronated. Her father reports he pulled her up by the hand onto a sidewalk step. What is the pathophysiology of her suspected condition?
Explanation
Question 67
When attempting closed reduction of a typical extension-type supracondylar fracture of the humerus with medial comminution, which position of the forearm is utilized to tension the intact medial periosteal hinge and prevent varus malalignment?
Explanation
Question 68
A newborn infant presents with a short, bowed right upper extremity and an absent thumb. Radiographs confirm congenital radial clubhand. Which of the following tests is mandatory in the initial workup of this patient?
Explanation
Question 69
An 8-year-old aspiring baseball pitcher complains of lateral elbow pain. Radiographs reveal flattening and sclerosis of the capitellum. The physis is open. What is the most likely diagnosis?
Explanation
Question 70
A 2-year-old child presents with a right thumb that is locked in flexion at the interphalangeal joint. A nodule is palpable at the volar aspect of the MCP joint. What is the recommended initial management?
Explanation
Question 71
A 5-year-old boy sustains an ipsilateral supracondylar humerus fracture and a distal radius fracture (floating elbow). This injury pattern places the patient at highest risk for which of the following complications?
Explanation
Question 72
Congenital pseudarthrosis of the clavicle most frequently presents as a painless mass in the middle third of the clavicle. It almost exclusively occurs on the right side. If it is found on the left side, which associated condition must be strongly suspected?
Explanation
Question 73
In a child with a typical Salter-Harris Type II fracture of the distal radius, what is the anatomical path of the fracture line?
Explanation
Question 74
Which of the following physical examination findings is most specific for diagnosing a severe Volkmann ischemic contracture in the upper extremity?
Explanation
Question 75
A 1-year-old child is diagnosed with complex syndactyly of the long and ring fingers. What is the fundamental difference between simple and complex syndactyly?
Explanation
Question 76
A 6-year-old boy undergoes a Woodward procedure for Sprengel deformity. What is the primary surgical objective of this procedure?
Explanation
Question 77
A 10-year-old child sustains a highly angulated, greenstick fracture of the radius and ulna. Following closed reduction, the surgeon decides to cast the arm. What physical principle governs the placement of a three-point mold in the cast?
Explanation
Question 78
Macrodactyly of the hand in a child is a rare congenital anomaly characterized by overgrowth of all tissue elements. Which nerve territory is most frequently affected, and what systemic condition must be ruled out?
Explanation
Question 79
A 5-year-old child presents with an extension-type supracondylar humerus fracture. Examination reveals an inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve is most likely injured?
Explanation
Question 80
Which of the following fracture patterns is considered highly specific for child abuse (non-accidental trauma) in an infant?
Explanation
Question 81
A 13-year-old boy presents with rigid flatfeet and a history of recurrent ankle sprains. Radiographs show an 'anteater nose' sign. Which of the following is the most likely diagnosis?
Explanation
Question 82
A 35-year-old man presents with progressive numbness in his ring and small fingers, and clawing of his hand. He has a history of an elbow fracture as a child and currently has a cubitus valgus deformity. Which of the following pediatric fractures is most likely responsible for his current condition?
Explanation
Question 83
In a 10-year-old child with an acute elbow dislocation and a medial epicondyle fracture, which of the following is an absolute indication for operative fixation?
Explanation
Question 84
A 6-year-old child sustains an elbow injury. A lateral radiograph
is obtained to evaluate the anterior humeral line. In a normal pediatric elbow, the anterior humeral line should intersect which portion of the capitellum?
Explanation
Question 85
A 9-year-old boy sustains a radial neck fracture with 45 degrees of angulation. Closed reduction in the emergency department fails. What is the most appropriate next step in management?
Explanation
Question 86
A 12-year-old obese boy presents with a 3-week history of left knee pain and an antalgic gait. Examination shows obligatory external rotation of the left hip during flexion. Which of the following is the most appropriate initial management?
Explanation
Question 87
During the Ponseti method for correcting congenital talipes equinovarus (clubfoot), which deformity is corrected LAST?
Explanation
Question 88
Which of the following parameters provides the greatest potential for remodeling in a pediatric diaphyseal both-bone forearm fracture?
Explanation
Question 89
According to the Kocher criteria, which of the following findings is NOT one of the four classic predictors used to differentiate pediatric septic arthritis of the hip from transient synovitis?
Explanation
Question 90
Which of the following is an absolute contraindication to the use of a Pavlik harness for the treatment of developmental dysplasia of the hip (DDH)?
Explanation
Question 91
A radiograph of a 7-year-old child's forearm
reveals an isolated fracture of the proximal ulna with apex anterior angulation. Which of the following is the most critical next step in evaluating this radiograph?
Explanation
Question 92
An 11-year-old boy sustains a proximal humerus fracture. What is the primary reason that large amounts of angulation and displacement can be treated non-operatively in this age group?
Explanation
Question 93
In the lateral pillar classification of Legg-Calvé-Perthes disease, which radiographic parameter is evaluated to determine the prognosis?
Explanation
Question 94
A 3-year-old girl is diagnosed with infantile Blount disease (tibia vara). Which of the following radiographic findings is characteristic of this condition?
Explanation
Question 95
A 10-year-old falls and sustains a fracture of the distal radius. Radiographs reveal a fracture line extending through the physis and exiting through the metaphysis, leaving a triangular metaphyseal fragment attached to the epiphysis. What is the Salter-Harris classification?
Explanation
None
