Orthopedic Prometric MCQs - Chapter 3 Part 15

Orthopedic Prometric MCQs - Chapter 3 Part 15
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 15-year-old girl is experiencing progressive weakness. She is unable to abduct her arms above 100° (pic). She has a progressive lordosis. Her facial expression is flat, and she cannot smile. Her mother has the same constellation of findings. No scoliosis is present. She and her mother are able to walk independently. The most likely diagnosis is:
Explanation
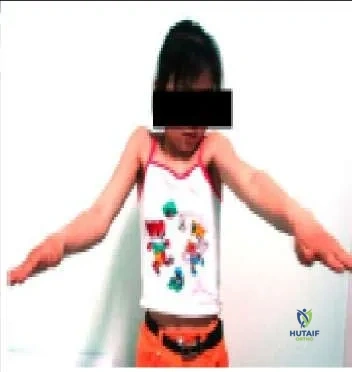 This patient most likely has facioscapulohumeral dystrophy. With a frequency of 1:20,000, it is a rare disorder inherited in an autosomal- dominant fashion. The genetic abnormality is found on chromosome 4, with a decreased number of D4Z4 tandem repeats, but this does not appear to code for a protein product. Scoliosis is not present. In this condition, selective weakness of the serratus anterior, trapezius, and rhomboid muscles is present. Therefore, the scapula is not effectively stabilized against the trunk during use.
This patient most likely has facioscapulohumeral dystrophy. With a frequency of 1:20,000, it is a rare disorder inherited in an autosomal- dominant fashion. The genetic abnormality is found on chromosome 4, with a decreased number of D4Z4 tandem repeats, but this does not appear to code for a protein product. Scoliosis is not present. In this condition, selective weakness of the serratus anterior, trapezius, and rhomboid muscles is present. Therefore, the scapula is not effectively stabilized against the trunk during use.
Question 2
A 10-year-old child, who has no history of fever, trauma, or infection, presents with minimal pain and a Trendelenburg gait on the left (Slide). Which of the following is the most likely diagnosis:
Explanation
Question 3
A patient who does not walk outdoors or independently but can walk with a walker in physical therapy is listed as what level according to the Gross Motor Function Measure (GMFM):
Explanation
Question 4
The patient shown in the clinical photograph (Slide 1) and radiograph (Slide 2) has which of the following conditions:
Explanation
 This patient has Klippel-Trenaunay-Weber syndrome. This syndrome is characterized by a triad of cutaneous nevi, varicose veins, and limb overgrowth in length and/or width.
This patient has Klippel-Trenaunay-Weber syndrome. This syndrome is characterized by a triad of cutaneous nevi, varicose veins, and limb overgrowth in length and/or width.
Question 5
An 8-year-old girl with no history of fever, illness, or weakness presents with an increasing spinal deformity. She was born in Asia. The patient is neurologically normal. Based on radiographs (Slide 1) and magnetic resonance images (Slide 2), the most likely diagnosis is:
Explanation
 This patient has congenital kyphosis. The relative disk destruction with vertebral preservation argues against tuberculosis. The anterior bony wedging is atypical for remote bacterial infection. Anterior fusion is not seen in patients with Scheuermann kyphosis (rarely after maturity) or in patients with compression fractures.
This patient has congenital kyphosis. The relative disk destruction with vertebral preservation argues against tuberculosis. The anterior bony wedging is atypical for remote bacterial infection. Anterior fusion is not seen in patients with Scheuermann kyphosis (rarely after maturity) or in patients with compression fractures.
Question 6
An 8-year-old boy presents with progressive deformity. Recommended management includes:
Explanation
This patient has a type II kyphosis (anterior bar). Because he is only 8 years old and the curve has progressed, further increase is likely. Observation is not indicated. Bracing has no influence on congenital curves. The kyphosis is >55° (78°) so a posterior fusion may not effectively halt the growth of these vertebral bodies in a posterior direction. Anterior and posterior fusion is the most likely procedure to control the curve.C orrect Answer: Anterior and posterior fusion 2291 A child with congenital below-elbow amputation is best fit with an active prosthesis at which age: A patient with congenital below-elbow amputation has sensation/proprioception in the limb and is able to perform most activities without assistance. Prostheses may interfere with crawling. Passive devices should not be started until walking begins, and active devices started at 2 to 4 years.
Question 7
Which of the following is the most specific feature of congenital vertical talus that distinguishes it from other deformities:
Explanation
Question 8
A 14-year-old boy sustains a hip dislocation in a motor vehicle accident. With closed reduction, he is at risk for all of the following except:
Explanation
Question 9
A 12-year-old boy sustains a distal diaphyseal femur fracture with a large butterfly fragment. He weighs 110 lb. Which of the following treatments is most appropriate and best able to preserve alignment:
Explanation
Question 10
Which of the following risks is associated with inserting a rigid femoral intramedullary nail through the piriformis fossa in a 10- to 14-year-old child:
Explanation
Question 11
Which of the following is a description of a closed kinetic chain exercise:
Explanation
Question 12
The action of bisphosphonates is primarily upon which component of bone:
Explanation
Question 13
Which of the following is not a common finding in patients with Prader- Willi syndrome:
Explanation
Question 14
Which of the following disease processes is demonstrated in the radiograph (Slide):
Explanation
Question 15
Which of the following accurately describes this radiograph (Slide):

Explanation
Question 16
An 11-year-old girl presents with bilateral painful flatfeet. A computed tomography image is shown (Slide). The most likely diagnosis is:

Explanation
Question 17
Which of the following is not a common feature of constriction band syndrome:
Explanation
Question 18
An 8-year-old child presents with a mass on the posteromedial side of the popliteal fossa. The mass, which has been present for more than 1 month, is nontender and moderately soft. The knee examination is stable. No knee effusion is present, and the patient has no signs or symptoms of infection. Radiographs are normal. Which of the following is the next step to aid in diagnosis:
Explanation
Question 19
Which of the following features is not associated with congenital muscular torticollis:
Explanation
Question 20
A 3-month-old female infant presents with the dorsum of the foot almost in contact with the anterior tibia. She has no pain with movement; plantar flexion and inversion of the feet are not restricted, but there is difficulty in manipulating the foot to the neutral position. She is normal otherwise. Which of the following treatments is most appropriate:
Explanation
Question 21
A 6-year-old child with spastic diplegic cerebral palsy requires the use of a wheeled walker for mobility indoors and outdoors. They are transported in a manual wheelchair for long distances in the community. What is the appropriate Gross Motor Function Classification System (GMFCS) level?
Explanation
Question 22
A 4-year-old boy presents with frequent falls and difficulty climbing stairs. On examination, he exhibits pseudohypertrophy of the calves and a positive Gowers sign. Which of the following is the most definitive diagnostic test for this condition?
Explanation
Question 23
A 7-year-old boy is diagnosed with Legg-Calve-Perthes disease.
Which of the following radiographic findings is considered a "head-at-risk" sign described by Catterall?
Explanation
Question 24
A 2-year-old child with Spinal Muscular Atrophy (SMA) type II presents for scoliosis evaluation. Which of the following medical therapies has recently revolutionized the treatment of SMA by modifying the SMN2 gene splicing to produce functional SMN protein?
Explanation
Question 25
During computerized gait analysis of a child with spastic diplegic cerebral palsy, the kinematic data reveals excessive knee flexion during the stance phase (crouch gait). Which of the following interventions is most likely to exacerbate this specific gait abnormality?
Explanation
Question 26
A 12-year-old boy with Charcot-Marie-Tooth disease presents with a progressive rigid cavovarus foot deformity.
Examination reveals a positive Coleman block test indicating hindfoot flexibility. The deformity is primarily driven by the relative overactivity of which muscle?

Explanation
Question 27
A 13-year-old obese boy underwent in situ pinning for a stable slipped capital femoral epiphysis (SCFE) 6 months ago. He now complains of progressive hip stiffness and pain. Radiographs reveal a narrowed joint space with periarticular osteopenia. What is the most likely cause of this complication?
Explanation
Question 28
A newborn with a myelomeningocele at the L4 level is evaluated in the nursery. What is the most likely hip pathology expected in this patient over time?
Explanation
Question 29
Which of the following patients with Cerebral Palsy is the most ideal candidate for Selective Dorsal Rhizotomy (SDR)?
Explanation
Question 30
A 3-year-old girl is diagnosed with a neglected unilateral developmental dysplasia of the hip (DDH).
The femoral head is dislocated superiorly. What is the most appropriate surgical management?
Explanation
Question 31
In a patient diagnosed with a unilateral slipped capital femoral epiphysis (SCFE), which of the following is an absolute indication for prophylactic pinning of the contralateral asymptomatic hip?
Explanation
Question 32
A 16-year-old boy presents with slowly progressive proximal muscle weakness. Muscle biopsy reveals reduced, but not absent, levels of dystrophin. He is diagnosed with Becker muscular dystrophy (BMD). What is the genetic transmission pattern of this disease?
Explanation
Question 33
According to consensus guidelines for hip surveillance in children with cerebral palsy, at what Gross Motor Function Classification System (GMFCS) level is the risk of hip displacement the highest, necessitating the most frequent radiographic screening?
Explanation
Question 34
A 12-year-old child with spastic diplegic cerebral palsy presents with a progressive crouch gait. Which of the following prior surgical interventions is the most common iatrogenic cause of this gait pattern?
Explanation
Question 35
A 13-year-old boy presents with a rigid flatfoot and frequent recurrent ankle sprains. Radiographs reveal a continuous 'C-sign' on the lateral foot view. Which of the following physical examination findings is most characteristic of this condition?
Explanation
Question 36
A 6-week-old female infant is placed in a Pavlik harness for a dislocated left hip (Ortolani positive). After 3 weeks of strict full-time harness wear, ultrasound shows the hip remains persistently dislocated. What is the most appropriate next step in management?
Explanation
Question 37
A 12-year-old obese boy presents to the emergency department unable to bear weight on his right leg after a minor fall. Radiographs confirm a severe, unstable slipped capital femoral epiphysis (SCFE). Which blood supply to the femoral head is most at risk of injury in this acute, unstable scenario?
Explanation
Question 38
In the Ponseti method for treating idiopathic clubfoot, what is the correct sequence of deformity correction?
Explanation
Question 39
A 4-year-old girl with blue sclerae, dentinogenesis imperfecta, and multiple prior long bone fractures is diagnosed with osteogenesis imperfecta. This condition is most commonly caused by a mutation affecting which of the following?
Explanation
Question 40
According to the Herring Lateral Pillar classification for Legg-Calve-Perthes disease, a hip in which the lateral pillar maintains between 50% and 100% of its original height is classified as:
Explanation
Question 41
A 2-year-old child with achondroplasia presents with delayed motor milestones, hypotonia, and sleep apnea. Which of the following is the most critical anatomical area to evaluate immediately?
Explanation
Question 42
A 9-year-old boy with Duchenne muscular dystrophy is referred for progressive neuromuscular scoliosis. At what point in the disease progression is posterior spinal fusion typically indicated?
Explanation
Question 43
A 7-year-old boy with spastic diplegic cerebral palsy presents with worsening crouch gait. He previously underwent isolated heel cord lengthening at age 4. Physical exam shows tight hamstrings and excessive ankle dorsiflexion. What is the most likely iatrogenic cause of his crouch gait?
Explanation
Question 44
A 4-year-old girl with cerebral palsy (GMFCS Level IV) undergoes routine radiographic hip surveillance. The AP pelvis radiograph demonstrates a Reimers' migration percentage of 45%. What is the most appropriate next step in management?
Explanation
Question 45
A 12-year-old boy weighing 90 kg presents with acute on chronic left knee and groin pain. He is unable to bear weight. Radiographs show a posterior and inferior displacement of the proximal femoral epiphysis. What is the most serious complication associated with the appropriate initial surgical treatment of this condition?
Explanation
Question 46
A 6-week-old female infant is treated with a Pavlik harness for a dislocated left hip. After 3 weeks of strict harness wear, ultrasound reveals that the hip remains persistently dislocated. What is the most appropriate next step in management?
Explanation
Question 47
During the Ponseti method for clubfoot correction, the physician must sequentially correct the deformities. Which of the following describes the correct order of correction and the anatomical fulcrum used during manipulation?
Explanation
Question 48
A 13-year-old boy presents with progressive right hip pain and stiffness 6 months after in situ pinning of a stable slipped capital femoral epiphysis. Examination reveals significant restriction of all hip motions, particularly internal rotation and abduction. Radiographs show symmetric narrowing of the joint space. What is the most likely diagnosis?
Explanation
Question 49
A 6-year-old boy presents with a painless limp. Radiographs reveal fragmentation and sclerosis of the proximal femoral epiphysis. According to the lateral pillar classification for Legg-Calvé-Perthes disease, which radiographic finding constitutes a Group C categorization?
Explanation
Question 50
A 4-year-old boy presents with calf pseudohypertrophy, a waddling gait, and uses his hands to push on his legs to stand up from the floor. Genetic testing reveals a mutation in the dystrophin gene. Which of the following is the most appropriate initial orthopedic consideration?
Explanation
Question 51
A 3-month-old infant is diagnosed with achondroplasia. What is the most critical neurological complication to screen for during the first year of life?
Explanation
Question 52
A newborn presents with severe hypotonia, absent deep tendon reflexes, and paradoxical breathing. Genetic testing confirms a homozygous deletion of the SMN1 gene. What is the diagnosis and its inheritance pattern?
Explanation
Question 53
A 3-year-old child with blue sclerae, dentinogenesis imperfecta, and multiple fractures with minimal trauma is evaluated. She is diagnosed with Osteogenesis Imperfecta (OI). Which molecular defect is most likely responsible?
Explanation
Question 54
A 4-year-old boy presents with delayed motor milestones and uses his hands to walk up his thighs to stand. Laboratory testing reveals significantly elevated creatine kinase. A muscle biopsy would most likely show an absence of which protein?
Explanation
Question 55
According to best practice guidelines for cerebral palsy hip surveillance, how frequently should a non-ambulatory 6-year-old child (GMFCS Level V) undergo radiographic screening of the hips?
Explanation
Question 56
A 2-year-old boy has profound hypotonia, absent deep tendon reflexes, and fine fasciculations of the tongue. He is able to sit independently but cannot pull to stand or walk. Genetic testing reveals a deletion in the SMN1 gene. What is the most likely orthopedic complication he will develop?
Explanation
Question 57
A 12-year-old obese male presents with a 3-week history of left groin pain and a limp. Physical examination reveals obligate external rotation of the left hip during passive flexion. Based on the clinical presentation and image provided, what is the most appropriate initial management for this stable deformity?
Explanation
Question 58
An 8-year-old boy presents with a painless limp of 4 months duration. Anteroposterior pelvis radiograph demonstrates fragmentation of the capital femoral epiphysis with >50% loss of lateral pillar height. According to the Herring Lateral Pillar classification, what group does this represent?
Explanation
Question 59
A 14-year-old boy presents with frequent ankle sprains and rigid, painful flatfeet. Oblique radiographs of the foot reveal an "anteater nose" sign. What is the most appropriate initial surgical intervention if conservative management fails?
Explanation
Question 60
A 5-year-old boy presents with anterolateral bowing of the tibia and multiple café-au-lait macules. Radiographs demonstrate diaphyseal narrowing and a pseudarthrosis. What is the primary underlying cellular defect in the pseudarthrosis tissue?
Explanation
Question 61
A 3-year-old girl with achondroplasia develops worsening hypotonia, hyperreflexia in the lower extremities, and newly recognized central sleep apnea. What is the most crucial next step in management?
Explanation
None
