Advanced Arthroscopic Interventions of the Elbow: Synovectomy, Contracture Release, and Fracture Management
Key Takeaway
Arthroscopic management of elbow pathology, including rheumatoid synovectomy, arthrofibrosis release, and intraarticular fracture care, requires meticulous portal placement and a thorough understanding of neurovascular anatomy. This guide details the Baker and Cummings technique for contracture release, emphasizing ulnar nerve protection, osteophyte resection, and rigorous postoperative rehabilitation protocols utilizing continuous passive motion and static progressive splinting to optimize functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The evolution of elbow arthroscopy has transitioned the modality from a purely diagnostic tool to a highly efficacious therapeutic intervention for a myriad of complex intraarticular pathologies. Historically, the elbow was considered an unforgiving joint for arthroscopic intervention due to its constrained osseous anatomy and the intimate, unforgiving proximity of major neurovascular structures. However, advancements in high-definition optics, specialized instrumentation, and a deeper understanding of portal anatomy have revolutionized the orthopedic surgeon's ability to manage pathology with minimally invasive techniques. Today, advanced elbow arthroscopy encompasses a broad spectrum of procedures, ranging from extensive synovectomy and capsular contracture release to the management of recalcitrant olecranon bursitis and arthroscopically assisted intraarticular fracture fixation.
The patho-epidemiology of conditions necessitating advanced elbow arthroscopy is both diverse and complex. Inflammatory arthritides, such as rheumatoid arthritis (RA), primary synovial chondromatosis, and pigmented villonodular synovitis (PVNS), are characterized by aggressive synovial hypertrophy. In these conditions, the hypertrophic synovium acts as a locally destructive tissue, releasing proteolytic enzymes, matrix metalloproteinases (MMPs), and inflammatory cytokines that relentlessly degrade the chondral surface. The elbow is particularly susceptible to stiffness secondary to capsular fibrosis induced by this chronic inflammation. Without intervention, this pathologic cascade predictably leads to progressive articular cartilage destruction, secondary osteoarthritis, and profound functional impairment.
Posttraumatic arthrofibrosis and degenerative contractures represent another major epidemiologic cohort requiring advanced arthroscopic management. The elbow joint is notorious for its fibrotic response to trauma, immobilization, or surgical intervention. The pathophysiology of elbow stiffness involves a complex interplay of intraarticular hematoma organization, myofibroblast proliferation, and subsequent dense collagen deposition within the anterior and posterior joint capsules. This fibrotic transformation significantly reduces capsular compliance, restricting the normal arc of motion. Furthermore, degenerative changes often result in concomitant osseous impingement, typically manifesting as osteophyte formation in the olecranon and coronoid fossae, which mechanically blocks terminal extension and flexion.
The application of arthroscopy in acute elbow trauma is an evolving frontier that addresses the patho-epidemiology of intraarticular fractures. Fractures of the radial head and capitellum frequently result in mechanical blocks to motion due to displaced osteochondral fragments or intraarticular hematoma. While open reduction and internal fixation (ORIF) remains the gold standard for significantly displaced fractures, arthroscopy offers a profound advantage in managing localized, minimally displaced fractures or retrieving unfixable shear fragments. By minimizing soft tissue dissection and preserving the extensor origin and lateral collateral ligament complex, arthroscopic techniques mitigate the iatrogenic trauma that often exacerbates postoperative stiffness, thereby optimizing functional recovery in a carefully selected patient demographic.
Detailed Surgical Anatomy and Biomechanics
The highly constrained osseous anatomy of the ulnohumeral and radiocapitellar joints demands a rigorous, three-dimensional understanding of spatial orientation from the operating surgeon. The ulnohumeral articulation functions primarily as a modified hinge joint, providing inherent osseous stability through the deep articulation of the trochlear notch of the ulna with the trochlea of the humerus. The radiocapitellar joint contributes to both flexion-extension and forearm pronation-supination, while also acting as a critical secondary stabilizer to valgus stress. This intricate osseous architecture is enveloped by a complex capsuloligamentous network, including the medial ulnar collateral ligament (MUCL) and the lateral collateral ligament (LCL) complex, which must be meticulously preserved during arthroscopic interventions to prevent iatrogenic instability.
A profound command of portal anatomy and its relationship to major neurovascular structures is the cornerstone of safe elbow arthroscopy. The proximal anteromedial portal, typically established 2 cm proximal and 1 cm anterior to the medial epicondyle, places the median nerve and brachial artery at risk. These structures lie an average of 14 mm to 22 mm lateral to the portal tract, necessitating blunt dissection and the use of a switching stick to protect the neurovascular bundle. The anterolateral portal, located just anterior to the radiocapitellar joint, poses a risk to the radial nerve, which courses an average of 7 mm medial to the portal. The precise establishment of these anterior portals is critical, as any deviation can result in catastrophic neurovascular injury.
The posterior compartment is accessed via the posterolateral, direct posterior, and accessory posterior portals. The posterolateral portal is established just superior to the tip of the olecranon and lateral to the triceps tendon, providing excellent visualization of the olecranon fossa and the posterior radiocapitellar articulation. The direct posterior portal, created 3 cm proximal to the olecranon tip through the triceps tendon, serves as the primary working portal for posterior debridement and osseous resection. While the posterior portals are generally considered safer than their anterior counterparts, the ulnar nerve remains a critical structure of concern. The ulnar nerve courses through the cubital tunnel, intimately associated with the posteromedial capsule. Any aggressive instrumentation or thermal ablation in the posteromedial gutter without direct visualization of the capsular boundary carries a high risk of iatrogenic ulnar nerve transection or thermal neuropraxia.
Biomechanical considerations during elbow arthroscopy extend beyond static anatomy to include the dynamic effects of fluid management and capsular distension. The elbow capsule has a relatively small baseline volume, typically accommodating only 15 to 25 milliliters of fluid before reaching maximum distension. Intraarticular pressure must be carefully modulated, as excessive pump pressures can lead to rapid fluid extravasation into the fascial compartments of the forearm and upper arm. This extravasation alters the normal anatomic relationships, bringing neurovascular structures dangerously close to the portal tracts, and can precipitate acute compartment syndrome. Therefore, maintaining arthroscopic pump pressures at the lowest possible setting (typically 30-40 mm Hg) while relying on gravity or controlled flow is a paramount biomechanical principle in advanced elbow arthroscopy.
Exhaustive Indications and Contraindications
The decision to proceed with advanced arthroscopic interventions of the elbow requires a meticulous evaluation of the patient's pathology, functional demands, and the inherent risks of the procedure. Arthroscopic synovectomy is highly indicated as a joint-preserving procedure for patients suffering from inflammatory arthritides, such as rheumatoid arthritis, primary synovial chondromatosis, PVNS, and hemophilic arthropathy. Surgical intervention is specifically warranted when aggressive medical management, including disease-modifying antirheumatic drugs (DMARDs) and biologic therapies, fails to control localized synovial hypertrophy, and there is an impending risk of progressive articular cartilage destruction.
Arthroscopic contracture release is indicated for patients with posttraumatic arthrofibrosis or degenerative stiffness who have failed a comprehensive, minimum 6-month trial of conservative management, including static progressive splinting and aggressive physical therapy. The ideal candidate presents with a functional deficit—typically defined as an arc of motion less than 30 to 130 degrees—that significantly impairs activities of daily living. Arthroscopic-assisted intraarticular fracture care is indicated for the excision of small, unfixable capitellar or radial head shear fragments, arthroscopic radial head resection in highly comminuted fractures where arthroplasty is not indicated, and limited internal fixation of simple fracture patterns (e.g., Mason Type II radial head fractures) where anatomic reduction can be achieved percutaneously.
Contraindications to elbow arthroscopy must be strictly respected to avoid devastating complications. Absolute contraindications include active superficial or deep soft tissue infection, severe distortion of normal bony or neurovascular anatomy that precludes safe portal placement, and the presence of a disrupted medial capsule in the setting of acute trauma, which provides a direct pathway for massive fluid extravasation and subsequent compartment syndrome. Previous ulnar nerve transposition is a critical relative contraindication; if the exact location of the transposed nerve cannot be definitively ascertained preoperatively or intraoperatively, the risk of iatrogenic injury is unacceptably high, and an open approach should be strongly considered.
| Indication / Pathology | Arthroscopic Intervention | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Rheumatoid Arthritis / PVNS | Radical Synovectomy | Active localized infection | Severe end-stage joint destruction (requires arthroplasty) |
| Synovial Chondromatosis | Synovectomy & Loose Body Removal | Altered neurovascular anatomy | Extensive extra-articular disease extension |
| Posttraumatic Arthrofibrosis | Capsular Release & Osteophyte Excision | Disrupted medial capsule (fluid leak risk) | Prior ulnar nerve transposition (if location unknown) |
| Intraarticular Fractures | Fragment Excision / Limited Fixation | Massive capsular tearing / ligamentous disruption | Highly comminuted fractures requiring complex ORIF |
| Recalcitrant Olecranon Bursitis | Arthroscopic Bursectomy (Controversial) | Active overlying cellulitis | Immunosuppression (high risk of portal fistula/infection) |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the foundation of successful advanced elbow arthroscopy. Standard radiographic evaluation, including true anteroposterior, lateral, and oblique views, is mandatory to assess joint congruity, identify loose bodies, and evaluate the extent of degenerative osteophyte formation. For patients presenting with posttraumatic stiffness or complex intraarticular fractures, a fine-cut, three-dimensional computed tomography (3D CT) scan is highly recommended. The 3D CT scan allows the surgeon to precisely map the location and volume of impinging osteophytes within the olecranon and coronoid fossae, facilitating accurate intraoperative osseous resection. Magnetic resonance imaging (MRI) is invaluable in the evaluation of inflammatory conditions, providing detailed characterization of synovial hypertrophy, the extent of PVNS lesions, and the integrity of the collateral ligaments.
Patient positioning is a critical determinant of surgical access and intraoperative safety. While the lateral decubitus and supine suspended positions are utilized by some surgeons, the prone position, as championed by Baker and Cummings, is widely considered the optimal setup for advanced arthroscopic contracture release and posterior compartment work. Following endotracheal intubation and the administration of a regional block (if not contraindicated by the need for immediate postoperative neurologic assessment), the patient is carefully transitioned to the prone position on the operating table. The operative arm is supported by two rolled towels placed longitudinally under the humerus, providing a stable platform while allowing the elbow to flex and extend freely over the edge of the bolster.
The prone position offers several distinct biomechanical and technical advantages. It allows gravity to assist in maintaining the arm position, reducing the need for an assistant to constantly manipulate the limb. More importantly, it provides excellent, unobstructed access to the posterior compartment, which is often the primary site of pathology in the stiff elbow. The olecranon fossa, posterior radiocapitellar articulation, and the medial and lateral gutters can be visualized and instrumented with unparalleled clarity. A sterile tourniquet is applied high on the brachium to ensure a bloodless field, though it should be inflated only when necessary to minimize ischemic time.
Fluid management planning is equally critical during the preoperative phase. The surgeon must ensure that the arthroscopic pump system is calibrated to deliver the lowest effective pressure, strictly maintaining settings between 30 and 40 mm Hg. High-flow, low-pressure systems are preferred to maintain clear visualization while mitigating the risk of fluid extravasation. The surgical team must be briefed on the abort criteria, specifically the clinical signs of impending compartment syndrome, such as excessive swelling or tension in the forearm or upper arm compartments. Prophylactic measures, including the use of gravity-assisted fluid drainage and the avoidance of excessive capsular distension, must be meticulously planned and executed.
Step-by-Step Surgical Approach and Fixation Technique
Arthroscopic Synovectomy
Arthroscopic synovectomy requires a systematic, compartmentalized approach to ensure comprehensive eradication of diseased tissue while preserving the delicate articular cartilage and capsuloligamentous restraints. The procedure is initiated with the establishment of the proximal anteromedial portal, serving as the primary viewing portal for the anterior compartment. Following diagnostic insufflation, an aggressive full-radius shaver is introduced via the anterolateral portal. The surgeon meticulously resects the hypertrophic synovium overlying the anterior capsule, the coronoid process, and the anterior radiocapitellar articulation. In conditions like PVNS or rheumatoid arthritis, the synovium is often highly vascular and friable, necessitating the concurrent use of radiofrequency ablation to maintain hemostasis and clear visualization.
Once the anterior compartment is cleared, the arthroscope is transitioned to the posterolateral portal to address the posterior compartment. The direct posterior portal is established to introduce the shaver and ablation devices. The olecranon fossa, posterior radiocapitellar articulation, and the medial and lateral gutters are systematically debrided. In cases of synovial chondromatosis, the surgeon must be vigilant in identifying and extracting all loose bodies, which frequently sequester in the dependent recesses of the joint.
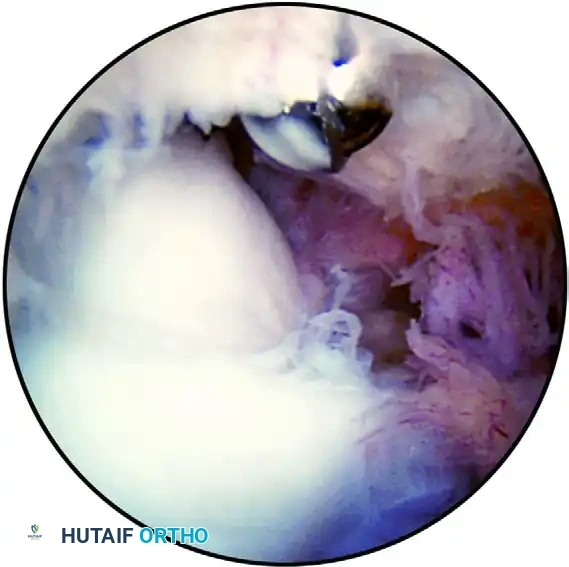
FIGURE 52-71 Extensive synovitis of the anterior compartment in a retired Major League pitcher presenting with persistent pain, popping, and swelling of the elbow. A partial synovectomy and removal of loose bodies were successfully performed.
Arthroscopic Contracture Release (Baker and Cummings Technique)
The arthroscopic release of posttraumatic arthrofibrosis and degenerative contractures is a highly technical procedure that demands a meticulous, step-wise approach to restore motion without compromising neurovascular integrity. The procedure begins with the preparation of the olecranon fossa. Dense scar tissue frequently obliterates this space in the stiff elbow; therefore, thorough debridement using a full-radius shaver is critical to establish baseline visibility. The arthroscope is then transitioned to the posterolateral portal, and an arthroscopic burr or osteotome is introduced through the direct posterior portal.
Osseous decompression is the next critical step. The surgeon systematically resects osteophyte formation from the tip of the olecranon and contours the olecranon fossa to eliminate bony impingement during terminal extension. Following osseous work, the posterior capsular contracture is carefully released. The surgeon employs blunt mobilization techniques, utilizing the shaver sheath without active suction or blades, to safely elevate and release the fibrotic capsule from the posterolateral and posteromedial gutters.
The most treacherous aspect of this procedure is the management of the posteromedial gutter due to the intimate proximity of the ulnar nerve. Mechanical shavers or thermal ablation devices must never be used in this region without direct visualization of the capsular boundary. If extensive posteromedial release is required, a posterior retractor portal is created approximately 2 cm proximal to the direct posterior portal. A small retractor-elevator is introduced to gently retract the medial capsule and soft tissues, providing a physical barrier that protects the ulnar nerve during burring or shaving.
Management of Olecranon Bursitis
The surgical management of recalcitrant olecranon bursitis remains a topic of significant debate within the orthopedic community. While the majority of cases resolve with conservative measures, chronic cases characterized by thickened bursal walls and persistent fluid accumulation necessitate excision. Historically, open bursectomy has been the gold standard, allowing for complete en bloc resection of the diseased tissue and meticulous layered closure to obliterate the dead space.
Arthroscopic bursectomy has been proposed as a minimally invasive alternative to circumvent the wound healing complications occasionally associated with open posterior incisions. However, the technique is fraught with significant concerns. The arthroscopic approach involves introducing a shaver into the bursal sac to morcellize and aspirate the tissue. This technique often fails to achieve complete resection of the thickened bursal walls. Furthermore, the literature highlights alarming complication rates associated with arthroscopic bursectomy. Studies by Kerr and Savoie have documented severe postoperative infections and the development of chronic, draining portal fistulas—complications that are notoriously difficult to manage over the extensor surface of the elbow. Consequently, the clinical consensus continues to favor open excision for recalcitrant olecranon bursitis, reserving the arthroscopic approach for highly selected cases under stringent indications.
Arthroscopic-Assisted Intraarticular Fracture Care
The application of arthroscopy in acute elbow trauma is an advanced technique reserved for specific, localized fracture patterns. Arthroscopy excels in the identification and excision of small, unfixable capitellar or radial head shear fragments that act as mechanical blocks to motion. In cases of highly comminuted radial head fractures where arthroplasty is contraindicated or unnecessary, arthroscopic radial head resection can be performed efficiently, minimizing the soft tissue trauma associated with an open lateral approach.
For larger, simple fracture patterns, such as Mason Type II radial head fractures or isolated capitellar fractures, arthroscopy can facilitate anatomic reduction. The surgeon utilizes the arthroscope to directly visualize the articular surface while manipulating the fracture fragments percutaneously using K-wires or specialized reduction tools. Once anatomic reduction is confirmed, limited internal fixation is achieved using headless cannulated screws inserted through percutaneous stab incisions.
However, the surgeon must remain acutely aware of the surgical pitfalls associated with arthroscopic fracture care. The procedure must never be attempted if a significant medial capsular injury has occurred, as the disrupted capsule provides a direct pathway for massive fluid extravasation into the forearm compartments. The surgeon must maintain a low threshold to convert to an open procedure and must immediately abort the arthroscopic approach if visualization is compromised by persistent hemarthrosis, if anatomic reduction cannot be definitively confirmed, or if there is any clinical evidence of fluid extravasation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, advanced elbow arthroscopy carries a distinct profile of potential complications that the operating surgeon must be prepared to manage. Neurologic injury is the most feared complication, with reported incidence rates ranging from 0.5% to 3% in large series. The ulnar nerve is particularly vulnerable during posteromedial capsular release and synovectomy, while the radial and median nerves are at risk during the establishment of anterior portals. Most neurologic injuries are transient neuropraxias secondary to fluid extravasation, tourniquet ischemia, or minor traction, and typically resolve with conservative management over several weeks to months. However, direct transection or severe thermal injury necessitates immediate microsurgical exploration and repair, often resulting in permanent functional deficits.
Fluid extravasation leading to compartment syndrome is a catastrophic complication unique to arthroscopic procedures utilizing pressurized fluid systems. The risk is significantly elevated in the setting of acute trauma with capsular disruption or during prolonged procedures with high pump pressures. Early clinical signs include excessive swelling, loss of skin wrinkling, and disproportionate pain in the forearm or upper arm. If fluid extravasation is suspected, the procedure must be immediately aborted, and the fluid source disconnected. The limb must be closely monitored; if compartment pressures remain elevated and clinical signs of compartment syndrome develop, emergent open fasciotomy of the affected compartments is mandatory to prevent irreversible ischemic necrosis.
Heterotopic ossification (HO) and recurrent stiffness are common complications following extensive arthroscopic contracture release, occurring in up to 10% to 15% of patients. The extensive soft tissue dissection and osseous resection create an environment highly conducive to ectopic bone formation. Prophylactic measures, including the administration of nonsteroidal anti-inflammatory drugs (NSAIDs) such as Indomethacin or Celecoxib, are critical in mitigating this risk. If significant HO develops and restricts motion, salvage management typically involves a delayed open or arthroscopic excision of the ectopic bone, performed only after the ossification has fully matured (typically 6 to 12 months postoperatively).
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Transient Neuropraxia | 1% - 3% | Fluid extravasation, traction, tourniquet time | Observation, physical therapy, gabapentinoids; usually resolves in 3-6 months. |
| Nerve Transection | < 0.5% | Direct iatrogenic injury (shaver/thermal device) | Immediate open microsurgical repair/grafting; poor prognosis for full recovery. |
| Compartment Syndrome | < 1% | Massive fluid extravasation via capsular tears | Emergent multi-compartment fasciotomy. |
| Heterotopic Ossification | 5% - 15% | Surgical trauma, inadequate prophylaxis | NSAID prophylaxis; delayed excision once bone is mature (6-12 months). |
| Portal Fistula / Infection | 1% - 2% | Poor wound healing (esp. in arthroscopic bursectomy) | Local wound care, oral/IV antibiotics; surgical debridement if refractory. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of any advanced arthroscopic intervention of the elbow, particularly contracture release, is inextricably linked to a rigorous, well-structured, and highly compliant postoperative rehabilitation program. The elbow joint is uniquely prone to rapid restiffening; therefore, the rehabilitation protocol must be initiated immediately and sustained with unwavering dedication. The protocol is generally divided into distinct phases, tailored to the specific procedure performed and the patient's individual tissue quality.
Phase I: Immediate Postoperative (0-24 Hours)
The immediate postoperative phase is focused on maintaining the intraoperative gains in range of motion while controlling acute inflammation and hemorrhage. Following an arthroscopic contracture release, the elbow is typically splinted in maximal extension while the patient is still under anesthesia, as extension is notoriously the most difficult motion to regain and maintain. This initial maximal extension splint is left in place for the first 24 hours. A surgical drain, typically placed in the direct posterior portal to prevent hematoma formation (which can act as a scaffold for recurrent fibrosis), is closely monitored and usually removed on postoperative day 1.
Phase II: Early Motion and Bracing (Days 1-21)
Phase II marks the critical window for establishing and preserving the functional arc of motion. Gentle active and active-assisted range-of-motion (ROM) exercises are initiated immediately after the removal of the initial splint. The patient is transitioned to a custom-molded, removable extension splint, which is worn at all times between exercise periods and during sleep. In patients with extensive posttraumatic arthrofibrosis and severe preoperative loss of motion, the use of an elbow continuous passive motion (CPM) machine is highly recommended. The CPM device is utilized to maintain the arc of motion during the critical first 3 weeks, preventing the early formation of intraarticular adhesions.
At approximately 1 week postoperatively, static progressive bracing, such as the Joint Active System, is introduced. The patient utilizes the brace for 30 minutes, three times a day, alternating between maximal tolerated extension and flexion. This low-load, prolonged stretch is highly effective in permanently elongating the healing capsular tissues. A rigorous home exercise program is mandatory, with the patient performing active and passive ROM exercises for 20 minutes, four to five times a day. Formal, supervised physical therapy is continued three times a week to ensure compliance, perform joint mobilizations, and monitor progress.
Pharmacologic prophylaxis during this phase is absolutely critical. An aggressive anti-inflammatory regimen is prescribed, typically consisting of a nonsteroidal anti-inflammatory drug (NSAID) such as Indomethacin (75 mg sustained release daily) or Celecoxib (200 mg daily) for the first 3 to 4 weeks. This regimen serves a dual purpose: it significantly decreases acute postoperative inflammation, thereby reducing pain and facilitating early motion, and it acts as a proven prophylactic measure against the development of heterotopic ossification (myositis ossificans), a known and devastating complication following extensive elbow capsular release.
Summary of Landmark Literature and Clinical Guidelines
The foundation of advanced elbow arthroscopy is built upon a robust body of landmark literature and evolving clinical guidelines that dictate best practices and optimize patient outcomes. The pioneering work of Baker and Cummings in the late 1990s fundamentally altered the approach to elbow stiffness. Their description of the prone positioning technique and the systematic, arthroscopic release of posttraumatic arthrofibrosis demonstrated that minimally invasive techniques could achieve functional outcomes comparable to traditional open arthrotomies, with significantly reduced surgical morbidity and accelerated rehabilitation timelines. Their step-wise approach to olecranon fossa preparation and osseous decompression remains the gold standard technique utilized by arthroscopists today.
In the realm of olecranon bursitis management, the literature provides critical cautionary insights. The studies published by Kerr and Savoie are frequently cited as landmark papers that highlight the severe complications associated with arthroscopic bursectomy. Kerr's report of severe postoperative infections in immunosuppressed patients and Savoie's documentation of chronic, draining portal fistulas underscore the inherent risks of attempting minimally invasive resections over the poorly vascularized extensor surface of the elbow. These papers form the basis of the current clinical consensus, which strongly advocates for open excision as the definitive and safer treatment modality for recalcitrant olecranon bursitis.
The application of arthroscopy in intraarticular fracture management is guided by the foundational principles established by the Mason classification system for radial head fractures. Clinical guidelines currently support the use of arthroscopy for Mason Type II fractures where mechanical blocks to motion are present, allowing for precise fragment excision or limited internal fixation. However, the literature consistently emphasizes the absolute necessity of recognizing capsular integrity. Landmark biomechanical studies have demonstrated the rapid and catastrophic fluid extravasation that occurs in the presence of medial capsular disruption, establishing the definitive clinical guideline that arthroscopic fracture management is strictly contraindicated in the setting of severe soft tissue compromise or complex instability patterns.
