Surgical Correction of Epicondylitis and Elbow Contractures
Key Takeaway
Surgical management of recalcitrant lateral and medial epicondylitis requires precise excision of angiofibroblastic tendinosis while preserving normal tissue. The modified Nirschl technique remains the gold standard, involving the meticulous release of the extensor carpi radialis brevis (ECRB) or flexor-pronator mass, decortication of the epicondyle, and robust repair. Concomitant elbow contractures may necessitate a lateral column procedure to restore functional range of motion.
Comprehensive Introduction and Patho-Epidemiology
Epicondylitis of the elbow, encompassing both lateral and medial variants, represents one of the most frequently encountered pathologies in the upper extremity clinic. Historically mischaracterized by the suffix "-itis," indicating an acute inflammatory cascade, the condition is now definitively understood to be a chronic degenerative tendinosis. This paradigm shift in our pathophysiological understanding is paramount for both non-operative management and surgical planning. The pathological hallmark, first eloquently described by Nirschl, is angiofibroblastic hyperplasia. This process is characterized by a failed healing response where normal, organized type I collagen is replaced by disorganized, immature type III collagen. Histological analysis consistently demonstrates fibroblastic proliferation, disorganized collagen matrices, and non-functional, neovascular formations without a significant presence of acute inflammatory cells such as macrophages or neutrophils. The presence of substance P and calcitonin gene-related peptide (CGRP) within this neural and vascular ingrowth is believed to be the primary driver of the nociceptive pain experienced by the patient.
Epidemiologically, lateral epicondylitis (tennis elbow) is substantially more prevalent than its medial counterpart (golfer's elbow), affecting approximately 1% to 3% of the general population, with a peak incidence occurring in the fourth and fifth decades of life. While it is classically associated with racket sports, the vast majority of patients are non-athletes who engage in repetitive occupational or recreational activities involving forceful wrist extension and forearm supination. Medial epicondylitis accounts for less than 20% of all epicondylitis cases and is intrinsically linked to repetitive valgus stress and wrist flexion. This is predominantly observed in overhead throwing athletes, such as baseball pitchers and javelin throwers, as well as in occupational settings requiring heavy lifting and repetitive pronation. The dominant arm is affected in over 75% of cases for both conditions, underscoring the mechanical and repetitive use etiology.
Concurrently, the management of elbow contractures represents a distinct but frequently overlapping challenge in orthopedic surgery. The elbow is notoriously unforgiving following trauma, prolonged immobilization, or chronic inflammatory arthritides. The joint capsule of the elbow is highly sensitive to injury, rapidly developing dense fibrotic adhesions and profound thickening. The patho-epidemiology of elbow stiffness is broadly categorized into extrinsic and intrinsic causes. Extrinsic contractures involve structures outside the articular cartilage, including the capsule, collateral ligaments, and surrounding musculature, frequently accompanied by heterotopic ossification (HO). Intrinsic contractures involve articular derangement, such as osteochondral defects, post-traumatic step-offs, and advanced degenerative joint disease.
Understanding the interplay between tendinopathy and joint mechanics is critical. Chronic pain from epicondylitis can lead to guarding and secondary extrinsic stiffness, while primary joint contractures alter the biomechanical force vectors across the elbow, potentially predisposing the common extensor or flexor origins to excessive shear stress and subsequent tendinosis. Therefore, a comprehensive understanding of both the degenerative tendinopathic processes and the fibrotic capsular cascades is required for the modern orthopedic surgeon to effectively restore pain-free, functional range of motion to the compromised elbow.
Detailed Surgical Anatomy and Biomechanics
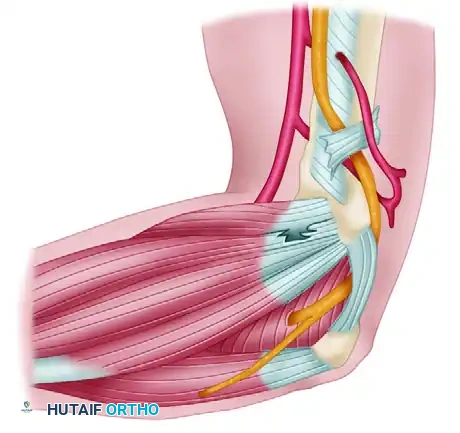
A profound understanding of the complex three-dimensional anatomy of the elbow is the foundation of successful surgical intervention and the avoidance of catastrophic iatrogenic complications. On the lateral aspect of the elbow, the common extensor origin is a confluence of tendinous structures originating from the lateral epicondyle and the lateral supracondylar ridge. The extensor carpi radialis longus (ECRL) originates most proximally on the supracondylar ridge and remains largely muscular at the level of the joint. Deep and distal to the ECRL lies the extensor carpi radialis brevis (ECRB), which is the primary site of pathology in lateral epicondylitis. The ECRB footprint is relatively small, taking its origin from the anterior aspect of the lateral epicondyle and blending intimately with the underlying joint capsule and the lateral ulnar collateral ligament (LUCL). Posterior to the ECRB is the extensor digitorum communis (EDC), followed by the extensor digiti minimi (EDM) and the extensor carpi ulnaris (ECU).
Biomechanically, the ECRB is uniquely susceptible to microtrauma. During the functional arc of motion, particularly in combined elbow extension and forearm pronation, the deep undersurface of the ECRB tendon is subjected to significant shearing forces against the prominent lateral edge of the capitellum. This mechanical attrition, combined with a relatively hypovascular zone at the tendon origin, creates an environment ripe for the initiation of angiofibroblastic degeneration. Furthermore, the LUCL, which originates from the isometric point on the lateral epicondyle and inserts on the supinator crest of the ulna, acts as the primary restraint to posterolateral rotatory instability (PLRI). The intimate anatomical relationship between the ECRB origin and the LUCL dictates that overzealous surgical debridement of the lateral epicondyle can inadvertently compromise the LUCL, leading to devastating iatrogenic instability.
Medially, the anatomy is dominated by the flexor-pronator mass and the medial ulnar collateral ligament (MUCL) complex. The flexor-pronator mass originates from the anterior aspect of the medial epicondyle and consists of the pronator teres (PT), flexor carpi radialis (FCR), palmaris longus (PL), flexor digitorum superficialis (FDS), and flexor carpi ulnaris (FCU). The primary pathology in medial epicondylitis typically localizes to the interface between the PT and the FCR. The biomechanics of the medial elbow are heavily influenced by valgus stress, particularly during the late cocking and early acceleration phases of the overhead throwing motion. The anterior bundle of the MUCL is the primary static stabilizer against valgus stress, originating from the anteroinferior surface of the medial epicondyle and inserting on the sublime tubercle of the ulna.
The neurologic anatomy surrounding the elbow is equally critical. Medially, the ulnar nerve courses posterior to the medial epicondyle within the cubital tunnel, roofed by Osborne's fascia. The proximity of the ulnar nerve to the medial epicondyle necessitates meticulous dissection and protection during medial epicondyle procedures. Additionally, the medial antebrachial cutaneous nerve (MABC) branches course anterior to the medial epicondyle and are highly susceptible to transection during surgical exposure, which can result in painful neuromas. Anteriorly, the radial nerve bifurcates into the superficial sensory branch and the posterior interosseous nerve (PIN) at the level of the radiocapitellar joint. The PIN courses deep to the supinator muscle (arcade of Frohse) and can be compressed in cases of radial tunnel syndrome, a condition that frequently mimics or coexists with recalcitrant lateral epicondylitis.
Exhaustive Indications and Contraindications
Surgical intervention for epicondylitis is rarely the first line of treatment. The natural history of the disease is often self-limiting, though it can run a protracted course of 12 to 18 months. Surgery is strictly indicated only after exhaustive, well-documented non-operative management has failed to provide functional relief. This non-operative regimen must include a minimum of 6 to 12 months of structured physical therapy emphasizing eccentric strengthening protocols, activity modification, counterforce bracing, nonsteroidal anti-inflammatory drugs (NSAIDs), and judicious use of biologic injections (such as Platelet-Rich Plasma) or, less favorably, corticosteroid injections. For elbow contractures, surgical release is indicated when the patient presents with a functional arc of motion less than 100 degrees (typically lacking the functional arc of 30 to 130 degrees of flexion) or a severe flexion contracture exceeding 30 to 45 degrees that is refractory to aggressive splinting and physical therapy.
Absolute contraindications to surgical intervention include active local or systemic infection, severe medical comorbidities precluding safe anesthesia, and the presence of complex regional pain syndrome (CRPS) in the affected extremity, as surgery will likely exacerbate the sympathetic dystrophy. Relative contraindications include patient non-compliance, active psychiatric disorders that would preclude participation in the rigorous postoperative rehabilitation protocols, and ongoing worker's compensation litigation, which has been statistically shown to correlate with poorer subjective surgical outcomes.
In the context of elbow contractures, severe intrinsic articular destruction (e.g., profound post-traumatic osteoarthritis with complete loss of the radiocapitellar and ulnohumeral joint spaces) is a relative contraindication to a simple capsular release. In such advanced cases, isolated soft tissue releases will fail to restore motion, and the surgeon must consider more complex reconstructive options, such as interposition arthroplasty, total elbow arthroplasty (TEA), or arthrodesis, depending on the patient's age and functional demands. Furthermore, unrecognized ligamentous insufficiency (e.g., chronic MUCL or LUCL tears) must be addressed concomitantly; performing a capsular release in the presence of gross instability will inevitably lead to a hypermobile, painful, and dysfunctional joint.
| Condition | Primary Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Lateral/Medial Epicondylitis | Failure of 6-12 months of exhaustive conservative therapy (PT, bracing, NSAIDs, injections). | Active local or systemic infection. | Ongoing worker's compensation litigation. |
| Unremitting pain severely limiting Activities of Daily Living (ADLs) or occupational duties. | Presence of Complex Regional Pain Syndrome (CRPS). | Poor patient compliance or inability to participate in rehab. | |
| MRI confirmation of high-grade partial tearing or profound tendinosis of ECRB or PT/FCR. | Medical comorbidities precluding anesthesia. | Concomitant untreated cervical radiculopathy. | |
| Elbow Contracture Release | Functional arc of motion < 100 degrees (normal functional requirement is 30-130 degrees). | Active joint infection (septic arthritis). | Severe intrinsic articular destruction (requires arthroplasty). |
| Severe flexion contracture > 30-45 degrees refractory to static progressive splinting. | Lack of functional musculature to control the joint post-release. | Unrecognized, untreated gross ligamentous instability. | |
| Extrinsic capsular contracture with preserved articular cartilage space on radiographs. | Non-compliant patient (immediate post-op CPM is mandatory). | Extensive, immature heterotopic ossification (HO). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative evaluation is the cornerstone of successful surgical outcomes. The clinical examination must systematically differentiate epicondylitis from other confounding pathologies. For lateral pain, provocative tests such as Cozen's test (resisted wrist extension with the elbow extended) and Maudsley's test (resisted extension of the middle finger) are highly sensitive. The surgeon must also palpate the radial tunnel and perform resisted forearm supination to rule out posterior interosseous nerve (PIN) entrapment. For medial pain, the moving valgus stress test and the milking maneuver are essential to assess the integrity of the medial ulnar collateral ligament (MUCL). A comprehensive neurologic examination is mandatory, with specific attention to the ulnar nerve, assessing for subluxation over the medial epicondyle during flexion, a positive Tinel's sign, and intrinsic muscle weakness.
Imaging modalities are critical for preoperative templating. Standard orthogonal radiographs (anteroposterior, lateral, and oblique views) are evaluated for traction osteophytes, intra-articular loose bodies, and calcifications within the tendon origins or collateral ligaments. For elbow contractures, a computed tomography (CT) scan with three-dimensional (3D) reconstruction is the gold standard. This allows the surgeon to meticulously map the location and volume of osteophytes, particularly those impinging within the olecranon and coronoid fossae, and to assess the congruity of the articular surfaces. Magnetic Resonance Imaging (MRI) is highly beneficial for epicondylitis, demonstrating T2 hyperintense signals indicative of edema, angiofibroblastic degeneration, or partial-thickness tearing of the ECRB or the flexor-pronator mass. MRI also aids in evaluating the integrity of the LUCL and MUCL prior to surgical debridement.
Patient positioning is dictated by the specific pathology and the planned surgical approach. For isolated lateral or medial epicondylitis, the patient is typically positioned supine on the operating table. The operative arm is abducted and placed on a radiolucent hand table. A sterile non-sterile pneumatic tourniquet is applied to the proximal brachium to ensure a bloodless surgical field, which is critical for identifying the subtle visual differences between healthy tendon and pathological angiofibroblastic tissue. The arm is prepped and draped in a standard sterile fashion, allowing for full, unrestricted range of motion of the elbow and wrist during the procedure.
For complex elbow contracture releases, particularly those requiring both anterior and posterior access (such as the lateral column procedure), the patient may be positioned in the lateral decubitus position. The operative arm is draped over a padded post (e.g., a Montreal positioner), allowing the elbow to rest at 90 degrees of flexion with gravity assisting in exposing the posterior compartment. Regardless of positioning, the use of regional anesthesia is highly recommended. An indwelling supraclavicular or axillary nerve catheter not only reduces intraoperative anesthetic requirements but also provides profound postoperative analgesia. This is exceptionally critical for contracture releases, as it allows the patient to tolerate immediate, aggressive continuous passive motion (CPM) and physical therapy on postoperative day one, thereby preventing the rapid reformation of intra-articular adhesions.
Step-by-Step Surgical Approach and Fixation Technique
Correction of Lateral Epicondylitis (Modified Nirschl Procedure)
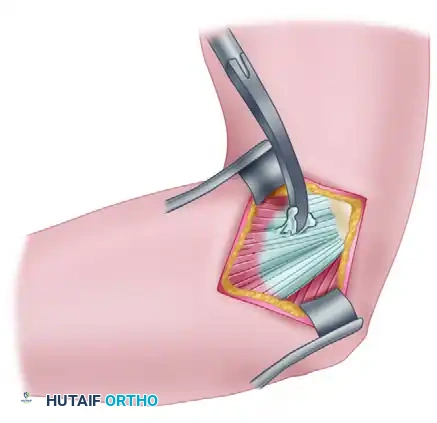
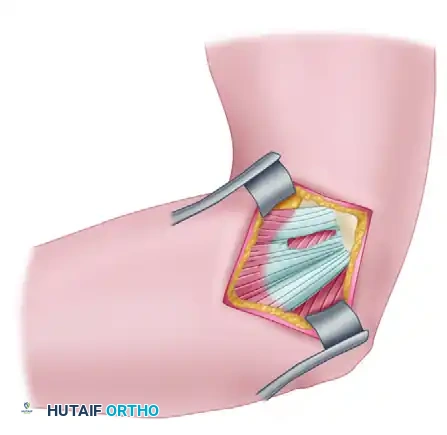
The modified Nirschl technique remains the gold standard for open surgical management. Following exsanguination and tourniquet inflation, a gently curved 5 cm incision is made centered just anterior to the lateral epicondyle. The deep fascia is incised in line with the skin. The critical first step is the accurate identification of the surgical interval between the extensor carpi radialis longus (ECRL) and the extensor digitorum communis (EDC).
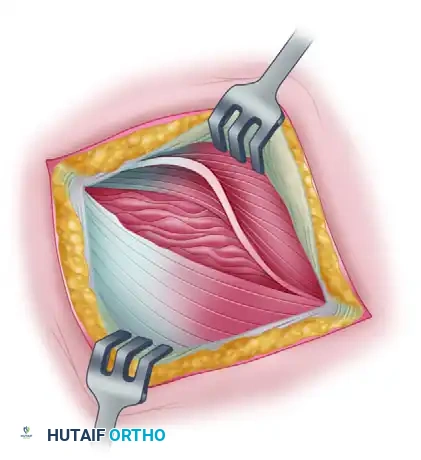
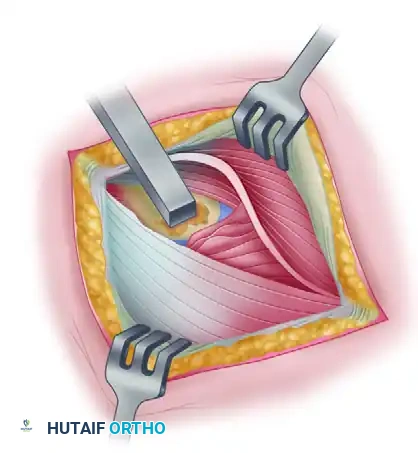
The ECRL is retracted anteriorly, revealing the deeper, centrally located origin of the extensor carpi radialis brevis (ECRB). The pathological ECRB tissue is visually distinct; it appears dull, grey, friable, and lacks the normal, organized longitudinal striations of healthy Sharpey's fibers.
The diseased ECRB tendon is meticulously excised. The surgeon must elevate the brevis portion of the conjoined tendon from the midportion of the lateral epicondyle, reflecting it distally. It is imperative to excise all angiofibroblastic tissue until healthy, bleeding tendon margins are reached. If the degenerative process extends anteriorly into the EDC origin, this involved tissue must also be resected. Crucially, the dissection must not violate the lateral ulnar collateral ligament (LUCL), which lies immediately deep and slightly posterior to the ECRB footprint.
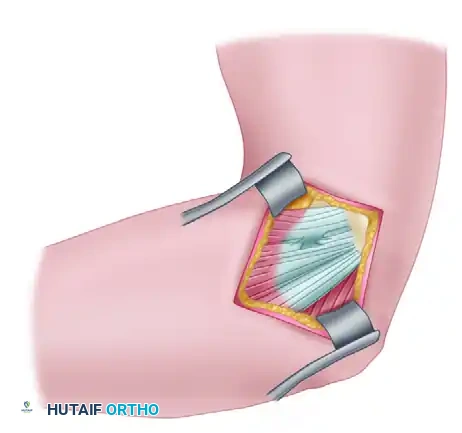
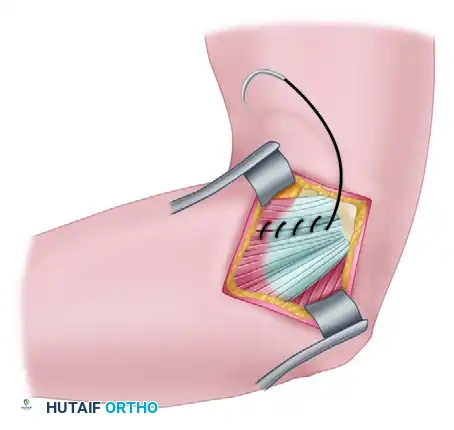
Following excision, epicondylar decortication is performed. Using a small rongeur, curette, or a 5mm osteotome, a localized area of the anterior lateral epicondyle is decorticated down to bleeding cancellous bone. This step is vital as it introduces mesenchymal stem cells, marrow elements, and growth factors into the surgical bed, facilitating a robust biological healing response. The remaining healthy ECRB tendon is then repaired. It can be sutured to the adjacent intact EDC fascia or anchored directly to the decorticated bone using transosseous drill holes or small suture anchors loaded with nonabsorbable suture. The ECRL-EDC interval is then meticulously closed over the repair with absorbable sutures to restore the fascial envelope.
Correction of Medial Epicondylitis (Nirschl Medial Approach)
Medial epicondylitis surgery demands rigorous attention to the surrounding neurovascular structures. A longitudinal incision is made centered over the medial epicondyle. Blunt dissection is utilized in the subcutaneous tissues to meticulously identify and retract the branches of the medial antebrachial cutaneous (MABC) nerve.
Once the common flexor origin is exposed, a longitudinal incision is made directly through the flexor-pronator mass, typically at the interval between the pronator teres and the flexor carpi radialis.
Retraction of the tendon edges exposes the underlying angiofibroblastic tissue. Similar to the lateral side, this tissue is grey, fibrillated, and avascular.
The pathological tissue is sharply excised down to the bleeding cortical bone of the medial epicondyle. The surgeon must exercise extreme caution to preserve the surrounding normal, healthy tendinous structures of the flexor mass to maintain the structural integrity of the medial elbow.
A partial medial epicondylectomy may be performed to enhance the healing bed and remove traction osteophytes. However, this resection must be strictly limited to the anterior 20% to 25% of the epicondyle. Excessive resection will detach or compromise the origin of the anterior bundle of the MUCL, leading to catastrophic valgus instability.
Following debridement and bony preparation, the defect in the flexor-pronator origin is securely closed. Heavy absorbable or nonabsorbable sutures are used to anchor the healthy tendon margins back to the prepared bony bed, ensuring a watertight closure. If the patient exhibited preoperative ulnar neuropathy, a concomitant ulnar nerve decompression and anterior transposition (subcutaneous or submuscular) is performed at this stage.
Surgical Management of Elbow Contractures (The Lateral Column Procedure)
For severe extrinsic contractures, the lateral column procedure provides unparalleled access. An extensile lateral incision is utilized, extending proximally along the lateral supracondylar ridge and distally over the radial head. The interval between the triceps posteriorly and the ECRL/brachioradialis anteriorly is developed. The common extensor origin and the anterior joint capsule are elevated off the anterior humerus. A comprehensive anterior capsulectomy is performed, excising the thickened, fibrotic capsule from the radial fossa to the coronoid fossa, meticulously protecting the anterior neurovascular bundle (brachial artery and median nerve) with a blunt retractor (e.g., a Homan retractor placed carefully over the brachialis muscle).
To address flexion deficits, the posterior compartment is accessed through the same lateral incision by elevating the triceps off the posterior humerus. The posterior capsule is excised, and any dense fibrous tissue or heterotopic ossification within the olecranon fossa is aggressively debrided using a high-speed burr or rongeurs. The tip of the olecranon may be resected if it is impinging within the fossa. Triceps tenolysis is performed to free any adhesions between the deep surface of the triceps and the posterior humerus. The elbow is then manipulated through a full range of motion under direct visualization to ensure all extrinsic tethers have been released and that there is no bony impingement.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the surgical management of epicondylitis and elbow contractures can occur and require prompt, decisive management. The most devastating complication following lateral epicondylitis surgery is iatrogenic posterolateral rotatory instability (PLRI). This occurs due to inadvertent transection or over-debridement of the lateral ulnar collateral ligament (LUCL) during the excision of the ECRB origin. Patients present with lateral elbow pain, a sense of "giving way," and a positive pivot-shift test. Salvage management requires formal LUCL reconstruction, typically utilizing a palmaris longus or gracilis autograft, passed through isometric transosseous tunnels in the lateral epicondyle and the supinator crest of the ulna.
Similarly, medial epicondylitis surgery carries the risk of iatrogenic valgus instability if the medial epicondylectomy is overly aggressive, compromising the medial ulnar collateral ligament (MUCL). Neurologic complications are also more prevalent on the medial side. Injury to the medial antebrachial cutaneous (MABC) nerve can result in a painful neuroma, which may require surgical excision and burying of the nerve stump into the adjacent muscle belly. Ulnar nerve irritation or subluxation can occur if the nerve is not adequately protected or transposed during the procedure. If postoperative ulnar neuritis develops and fails to resolve with conservative measures, a revision decompression and submuscular transposition is indicated.
Following elbow contracture release, the most frequent complication is the recurrence of stiffness. The elbow joint is highly prone to rapid adhesion formation and heterotopic ossification (HO). The incidence of recurrent contracture can be as high as 20-30% in severe post-traumatic cases. Prevention is paramount and includes the immediate postoperative use of Continuous Passive Motion (CPM), aggressive physical therapy, and pharmacological prophylaxis (e.g., Indomethacin 75mg sustained-release daily for 3-6 weeks) or localized postoperative radiation therapy (single dose of 700 cGy within 48 hours of surgery) for high-risk patients. If severe stiffness recurs, a revision open release or distraction arthroplasty may be necessary.
| Complication | Estimated Incidence Rate | Primary Etiology | Salvage Management Strategy |
|---|---|---|---|
| Iatrogenic PLRI | < 1% - 2% (Lateral Release) | Inadvertent transection of the LUCL during ECRB debridement. | Open LUCL reconstruction using palmaris longus or gracilis tendon autograft. |
| MABC Neuroma | 2% - 5% (Medial Release) | Transection or traction injury to MABC branches during skin incision/exposure. | Excision of the neuroma and burying the proximal nerve stump deep into muscle. |
| Ulnar Neuritis | 3% - 7% (Medial Release) | Traction, scarring, or unrecognized subluxation of the ulnar nerve. | Revision decompression and anterior transposition (subcutaneous or submuscular). |
| Recurrent Stiffness | 15% - 30% (Contracture Release) | Inadequate initial release, failure of immediate rehab, or HO formation. | Revision capsular release, manipulation under anesthesia (early), HO excision, or distraction arthroplasty. |
| Infection (Deep) | < 1% | Contamination, hematoma formation, immunocompromised state. | Irrigation and debridement (I&D), culture-directed intravenous antibiotics. |
| Recalcitrant Pain | 5% - 10% (Epicondylitis) | Incomplete excision of angiofibroblastic tissue, incorrect initial diagnosis. | MRI evaluation, revision debridement, consideration of anconeus muscle flap rotation. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following elbow surgery requires a nuanced, phase-based approach that is strictly goal-dependent rather than merely time-dependent. The protocols for epicondylitis repair and contracture release are fundamentally opposed in their initial phases. Epicondylitis repair requires a period of tissue protection to allow the tendon-to-bone healing process to initiate, whereas contracture release demands immediate, aggressive mobilization to prevent the reformation of dense intra-articular adhesions.
Phase 1: Acute Phase (Weeks 0–2)
For epicondylitis (lateral and medial), the primary goals are the reduction of inflammation, protection of the surgical repair, and retardation of muscular atrophy. The elbow is typically immobilized in a posterior splint at 90 degrees of flexion for the first 5 to 7 days. Upon splint removal, modalities such as cryotherapy, high-voltage galvanic stimulation, and gentle soft tissue mobilization are initiated. Range of motion (ROM) exercises consist of gentle, passive, and active-assisted wrist extension/flexion, elbow extension/flexion, and forearm supination/pronation. Strict restrictions are placed on forceful gripping, lifting, or any movements that place eccentric tension on the repaired tissues.
Conversely, for elbow contracture releases, Phase 1 begins in the recovery room. The patient is frequently managed with an indwelling regional nerve block to provide profound analgesia. A Continuous Passive Motion (CPM) machine is applied immediately, and the patient is encouraged to achieve maximum flexion and extension limits. Active and active-assisted ROM exercises are performed multiple times daily under the supervision of a physical therapist. Static progressive splinting (e.g., turnbuckle splints) is utilized during periods of rest, alternating between maximum extension and maximum flexion to maintain the intraoperative gains.
Phase 2: Subacute Phase (Weeks 2–6)
In the management of epicondylitis, Phase 2 marks the transition to active tissue loading. The goals are to improve flexibility, increase muscular strength and endurance, and correct kinetic chain deficits. Strengthening programs emphasize concentric and, more importantly, eccentric loading of the involved muscle groups (wrist extensors for the lateral side; wrist flexors and pronators for the medial side). Proximal stabilization is critical; shoulder and scapular strengthening exercises are integrated to ensure that force generation is distributed throughout the entire upper extremity kinetic chain, rather than isolated at the elbow. A counterforce brace may be utilized during these activities to disperse forces away from the healing epicondylar origin.
For contracture releases, Phase 2 involves weaning from the CPM machine and maximizing active range of motion. Strengthening is introduced gradually, but the primary focus remains on capsular stretching and maintaining the terminal degrees of extension and flexion. Joint mobilization techniques (e.g., sustained glides) are employed by the physical therapist to
