Advanced Surgical Management of Elbow Contracture and Heterotopic Ossification
Key Takeaway
The surgical management of elbow contracture requires meticulous anterior and posterior capsulectomies to restore functional range of motion. Utilizing an extensile lateral Kocher approach, surgeons can safely elevate the brachialis and triceps to perform sequential releases. Early excision of heterotopic ossification, typically 3 to 6 months post-injury, is now recommended once fractures have united and local inflammation has resolved, optimizing postoperative rehabilitation and functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The elbow joint represents a highly constrained, exquisitely congruent articulation that is profoundly susceptible to post-traumatic stiffness. This propensity for contracture arises from its complex osseous architecture, dense capsuloligamentous network, and an aggressive, robust fibroblastic response to injury. The normal elbow possesses a physiological range of motion (ROM) extending from 0 degrees of full extension to approximately 140 to 150 degrees of flexion, coupled with 70 to 80 degrees of both pronation and supination. However, the functional arc of motion—as classically delineated by Morrey and colleagues—requires only 30 to 130 degrees of flexion and 50 degrees of both pronation and supination to perform the vast majority of activities of daily living (ADLs). When an elbow fails to achieve this functional arc, the patient experiences significant disability, severely limiting their independence and quality of life.
The pathophysiology of elbow stiffness is fundamentally rooted in a cascade of inflammatory and fibrotic events triggered by trauma, surgical intervention, or prolonged immobilization. At the cellular level, the initial hematoma and inflammatory phase flood the joint with cytokines, most notably transforming growth factor-beta 1 (TGF-β1), platelet-derived growth factor (PDGF), and interleukins. These mediators stimulate the differentiation of local fibroblasts into myofibroblasts, which are characterized by the expression of alpha-smooth muscle actin. These myofibroblasts aggressively synthesize disorganized type I and type III collagen, leading to profound capsular hypertrophy, contracture, and obliteration of the normal joint recesses. The anterior capsule, in particular, can thicken from a normal 1-2 mm to over 5-6 mm, acting as an unyielding tether against joint excursion.
Heterotopic ossification (HO) represents a distinct, yet frequently overlapping, patho-epidemiological entity characterized by the formation of mature lamellar bone within non-osseous soft tissues. The precise etiology of HO remains partially obscure but is universally recognized to involve the inappropriate osteoblastic differentiation of pluripotent mesenchymal stem cells. This process is driven by local inflammatory mediators (e.g., bone morphogenetic proteins [BMPs], prostaglandins) and amplified by systemic factors. Epidemiologically, HO is most frequently encountered following severe local trauma—such as the "terrible triad" of the elbow, complex distal humerus fractures, and massive fracture-dislocations. Furthermore, systemic conditions such as severe thermal burns (particularly those involving >20% total body surface area) and traumatic brain injuries (TBI) or spinal cord injuries dramatically upregulate the systemic osteogenic response, increasing the incidence of clinically significant periarticular elbow HO to as high as 20% to 30% in these specialized populations.
When conservative measures—including aggressive, supervised physical therapy, continuous passive motion, and static-progressive or dynamic splinting—fail to restore the functional arc after 6 months of dedicated effort, operative intervention is strongly indicated. The surgical release of an elbow contracture, often combined with the excision of heterotopic bone, demands a comprehensive understanding of elbow biomechanics, precise extra-articular and intra-articular soft-tissue handling, and a strategic, algorithmic approach to both the anterior and posterior compartments.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of elbow anatomy and biomechanics is the absolute prerequisite for safe and effective contracture release. The elbow is a complex hinge (ginglymus) and pivot (trochoid) joint comprised of three distinct articulations enclosed within a single synovial cavity: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The ulnohumeral joint provides the primary flexion-extension arc and is intrinsically stable due to the deep, highly congruent articulation between the trochlear notch of the ulna and the spool-shaped trochlea of the distal humerus. The radiocapitellar joint contributes to both flexion-extension and forearm rotation, while also serving as a critical secondary restraint to valgus stress, transmitting up to 60% of the axial load across the elbow.
The capsular anatomy dictates the fundamental patterns of stiffness. The anterior capsule originates proximal to the radial and coronoid fossae and inserts onto the anterior aspect of the coronoid process and the annular ligament. It is the primary soft-tissue restraint to elbow extension. Conversely, the posterior capsule, which originates proximal to the olecranon fossa and attaches to the articular margins of the olecranon, restricts terminal flexion. A critical clinical pearl dictates that a comprehensive release almost universally requires addressing both the anterior and posterior compartments, regardless of whether the primary clinical deficit is predominantly in flexion or extension, due to the circumferential nature of the fibrotic response.
Ligamentous stability is governed by the medial collateral ligament (MCL) and the lateral collateral ligament (LCL) complexes. The anterior bundle of the MCL is the primary restraint to valgus stress and must be rigorously protected during any medial dissection. The LCL complex, specifically the lateral ulnar collateral ligament (LUCL), originates on the lateral epicondyle and inserts on the supinator crest of the ulna. The LUCL is the primary restraint to posterolateral rotatory instability (PLRI). During a lateral-based contracture release, the capsulectomy must remain strictly anterior to the LUCL footprint to prevent catastrophic iatrogenic instability.
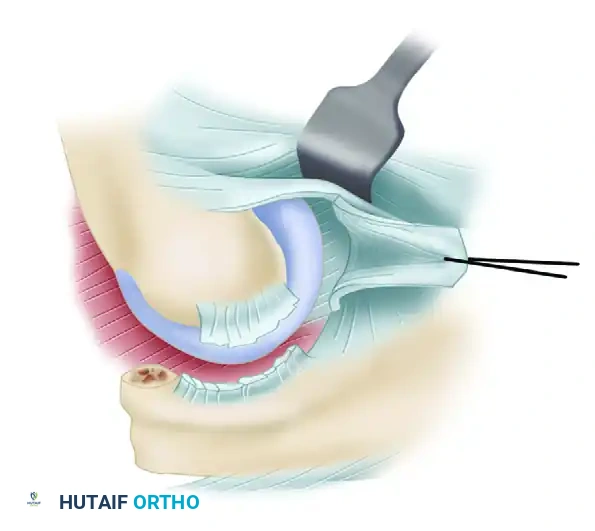
The neurovascular anatomy surrounding the elbow is notoriously unforgiving and intimately associated with the joint capsule. Anteriorly, the brachial artery and median nerve lie centrally, separated from the anterior capsule only by the brachialis muscle. The brachialis serves as a vital protective barrier; thus, subperiosteal elevation of the brachialis off the anterior capsule is a mandatory safety maneuver during anterior release. The radial nerve courses anterolaterally between the brachialis and brachioradialis, crossing the radiocapitellar joint before dividing into the superficial sensory branch and the posterior interosseous nerve (PIN). Posteriorly and medially, the ulnar nerve traverses the cubital tunnel, lying directly posterior to the medial epicondyle. It is highly susceptible to injury during posterior capsulectomy, medial osteophyte excision, or medial HO resection.
Exhaustive Indications and Contraindications
The decision to proceed with surgical management of elbow stiffness or heterotopic ossification requires a nuanced evaluation of the patient's functional deficit, the underlying etiology of the contracture, and the biological timing of the intervention. Operative release is generally considered when a patient exhibits a persistent, functionally limiting loss of motion that has plateaued despite a minimum of 6 months of aggressive, compliance-verified conservative therapy.
Surgical indications are broadly categorized into intrinsic and extrinsic causes. Extrinsic contractures, which involve the capsule, collateral ligaments, and extra-articular heterotopic bone, are highly amenable to open or arthroscopic release. Intrinsic causes, such as severe intra-articular step-offs, advanced post-traumatic osteoarthritis, or massive osteochondral defects, may not be adequately addressed by soft-tissue release alone and may necessitate interposition arthroplasty or total elbow arthroplasty (TEA) in the appropriately aged patient.
Contraindications must be strictly respected to prevent disastrous outcomes. Active joint infection is an absolute contraindication to contracture release; the infection must be eradicated prior to any reconstructive effort. Severe, acute complex regional pain syndrome (CRPS) is a strong relative contraindication, as surgical trauma can cause a catastrophic flare of the condition. Furthermore, a patient who is unable or unwilling to participate in the grueling, mandatory postoperative rehabilitation protocol is a poor candidate, as the elbow will inevitably re-stiffen, often worse than the preoperative state.
| Indication / Contraindication | Rationale / Underlying Mechanism | Clinical Caveats and Management Strategies |
|---|---|---|
| Indication: Failure of conservative management (>6 months) | Soft tissue remodeling has plateaued; splinting/PT will yield no further gains. | Ensure patient was truly compliant with static-progressive splinting before declaring failure. |
| Indication: Heterotopic Ossification causing ankylosis | Ectopic bone physically blocks the hinge mechanism or bridges the joint. | Early excision (3-6 months) is now favored over waiting 18 months, provided fractures are healed. |
| Indication: Ulnar neuropathy combined with stiffness | Fibrosis or HO entraps the ulnar nerve in the cubital tunnel, risking permanent denervation. | Requires simultaneous ulnar nerve decompression and possible anterior transposition during release. |
| Contraindication: Active periarticular infection | Surgical release will disseminate infection and guarantee failure of the procedure. | Must perform serial debridements and targeted antibiotic therapy before considering reconstructive release. |
| Contraindication: Acute Complex Regional Pain Syndrome (CRPS) | Surgical trauma exacerbates sympathetic dysregulation, worsening pain and stiffness. | Delay surgery; utilize aggressive pain management, sympathetic blocks, and gentle ROM until quiescent. |
| Contraindication: Non-compliant patient | Post-operative rehab is painful and demands daily adherence to splinting and ROM exercises. | Pre-operative psychological screening is vital. If the patient cannot commit to rehab, surgery is futile. |
Pre-Operative Planning, Templating, and Patient Positioning
A meticulous preoperative assessment is paramount to the success of an elbow contracture release. The surgeon must systematically differentiate between intrinsic and extrinsic causes of stiffness. The clinical examination must document the exact active and passive ROM, the presence of a firm versus a soft endpoint (indicating bony versus soft-tissue blocks), and a rigorous neurovascular assessment. Particular attention must be paid to the ulnar nerve; any preoperative subluxation, Tinel's sign, or intrinsic muscle weakness dictates the need for formal ulnar nerve exploration and transposition during the release.
Standard anteroposterior, lateral, and oblique radiographs are mandatory to assess joint congruency, identify osteophytes, and detect heterotopic ossification. However, plain films are often insufficient for complex cases. A computed tomography (CT) scan with 3D surface rendering is highly recommended and considered the gold standard for preoperative templating. The 3D CT precisely maps the location, volume, and anatomical relationships of ectopic bone. It allows the surgeon to evaluate the olecranon and coronoid fossae for subtle osseous impingement and precisely plan the extent of bony debridement required to restore the arc of motion.
Historically, surgical dogma dictated that excision of HO should be delayed for 12 to 18 months until the ectopic bone had fully "matured," as defined by a normal serum alkaline phosphatase level and a quiescent bone scan. This paradigm has shifted dramatically. Modern evidence-based orthopaedics strongly favors early surgical excision (typically 3 to 6 months post-injury). Criteria for early excision include complete union of all associated fractures, complete healing of all initial surgical or traumatic wounds, and resolution of local soft-tissue inflammation. Early excision prevents the profound secondary soft-tissue contractures and articular cartilage degradation that occur with prolonged joint immobilization.
Patient positioning is a critical step that facilitates the extensile exposures required for complete release. The patient is placed in the supine position on a standard operating table. A sandbag or a rolled towel is positioned under the ipsilateral scapula to elevate the shoulder, allowing the arm to rest comfortably across the chest. A sterile tourniquet is applied high on the brachium to ensure a bloodless surgical field, which is essential for identifying critical neurovascular structures and delineating tissue planes. The extremity is draped free, allowing full, unencumbered manipulation of the elbow through its maximum arc of motion during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The extensile lateral approach, popularized by Morrey, is the workhorse technique for addressing severe elbow contractures. It allows simultaneous, panoramic access to both the anterior and posterior compartments while preserving the critical medial structures, provided the dissection meticulously respects the anatomic boundaries.
The Extensile Lateral (Kocher) Approach
The surgical exposure begins with an extensile modification of the classic Kocher approach, designed to provide comprehensive access to the lateral column of the distal humerus, the radiocapitellar joint, and the anterior/posterior capsules.
Make an extensive longitudinal skin incision, approximately 15 cm in length. Begin proximally along the lateral supracondylar ridge of the humerus, continue the incision distally passing directly over the lateral epicondyle, and terminate it over the subcutaneous border of the proximal ulna.
Proximally, the dissection is carried sharply down to the lateral supracondylar ridge. The surgeon must identify the interval between the triceps posteriorly and the brachioradialis anteriorly. Distally, the deep fascia is incised along the lateral margin of the triceps, developing the internervous plane between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (innervated by the posterior interosseous nerve).
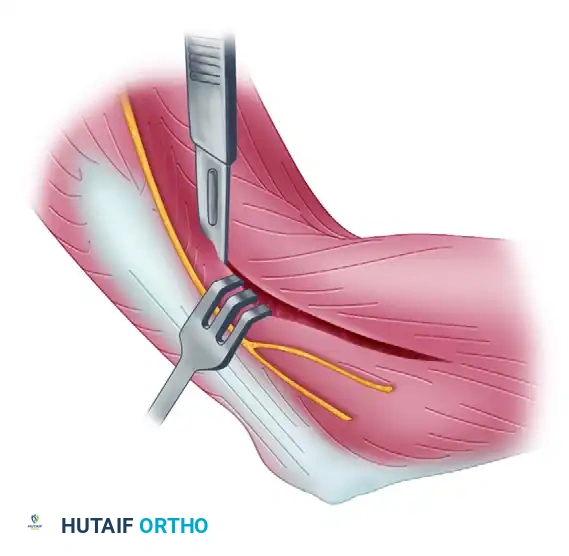
Deep Dissection and Anterior Capsulectomy
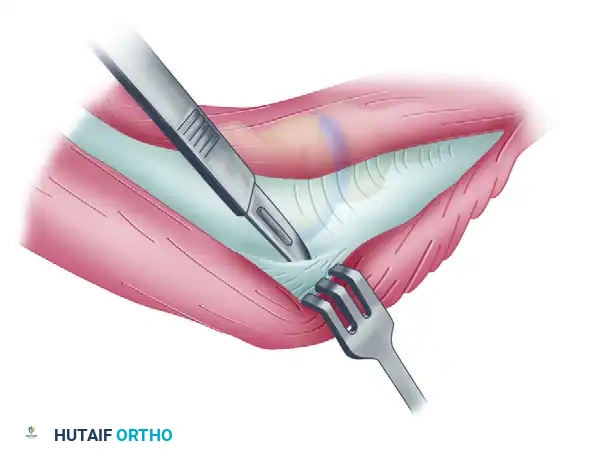
The primary goal of the anterior dissection is to safely separate the neurovascular structures from the anterior capsule before performing the capsulectomy. The brachialis muscle belly is carefully elevated subperiosteally off the anterior joint capsule. This maneuver is critical, as the brachialis serves as a protective barrier for the brachial artery and the median nerve. Blunt retractors (such as right-angle or Hohmann retractors) are placed deep to the brachioradialis and brachialis muscles to safely retract the anterior neurovascular bundle, exposing the underlying, thickened anterior joint capsule.
A comprehensive anterior capsulectomy is then performed, proceeding systematically from lateral to medial. The surgeon must identify and preserve the lateral collateral ligament (LCL) complex, specifically the LUCL. The capsulectomy must stay strictly anterior to the LCL origin on the lateral epicondyle to prevent iatrogenic posterolateral rotatory instability (PLRI). When extending the anterior capsulectomy medially, the dissection must remain strictly within the capsular plane to avoid injury to the median nerve anteriorly and the ulnar nerve medially.
Posterior Dissection and Capsulectomy
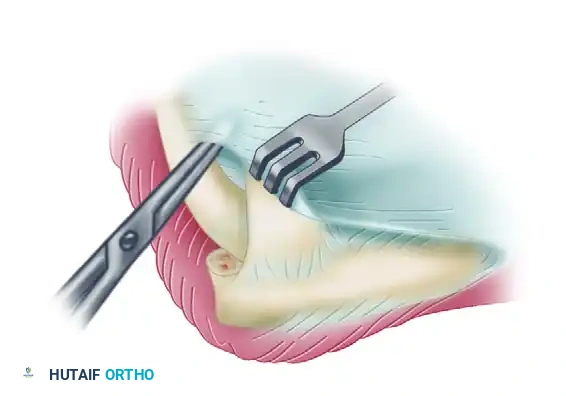
Once the anterior release is complete, attention is turned to the posterior compartment to restore terminal elbow flexion. To preserve periosteal continuity and optimize triceps function postoperatively, the triceps tendon is elevated subperiosteally from the posterior aspect of the humerus and the tip of the olecranon.

The mobilized triceps is retracted posteriorly and medially to expose the underlying posterior joint capsule and the olecranon fossa. A posterior capsulectomy is performed, again proceeding from lateral to medial. Extreme care must be taken not to venture too far medially during the posterior capsulectomy, as the ulnar nerve lies immediately posterior to the medial epicondyle. If extensive medial capsular release or medial HO excision is required, a separate medial incision to decompress and protect the ulnar nerve is strongly advised.
Bony Debridement and Impingement Clearance
Soft-tissue release alone is often insufficient if osseous impingement or HO exists. The surgeon must dynamically test the elbow and address any bony blocks. The elbow is completely extended; if extension remains incomplete despite a full anterior capsulectomy, the limitation is likely osseous. The olecranon fossa is debrided of any fibrotic scar tissue or loose bodies. The tip of the olecranon is resected using a sharp osteotome or rongeur, and any osteophytic enlargement along the margins of the olecranon fossa is cleared.
Next, the elbow is flexed. If flexion to 135 degrees is impossible, the anterior compartment is investigated for osseous impingement. Dense scar tissue, loose bodies, or osteophytes located in or around the coronoid fossa and the radial fossa are removed. Excision of the tip of the coronoid process may occasionally be necessary to maximize terminal flexion. Following complete release and debridement, the joint is assessed for stability, the lateral tissue sleeve is meticulously repaired, and the wound is closed in layers over a suction drain.
Complications, Incidence Rates, and Salvage Management
The surgical management of elbow contracture and heterotopic ossification is fraught with potential complications, even in the hands of experienced upper extremity surgeons. The intimate relationship between the joint capsule and major neurovascular structures, combined with the biological propensity of the elbow to form scar tissue, creates a highly challenging surgical landscape.
Neurologic injury, particularly to the ulnar nerve, is the most feared complication. The ulnar nerve is highly vulnerable during medial dissection, posterior capsulectomy, and excision of medial heterotopic bone. Iatrogenic instability, specifically posterolateral rotatory instability (PLRI), occurs if the lateral ulnar collateral ligament (LUCL) is inadvertently transected during the lateral approach or anterior capsulectomy. Recurrence of stiffness or HO is a constant threat, necessitating strict adherence to postoperative prophylaxis and rehabilitation.
| Complication | Estimated Incidence | Prevention and Salvage Management Strategies |
|---|---|---|
| Ulnar Neuropathy | 5% - 15% | Prevention: Prophylactic decompression/transposition if medial work is required. Avoid blind medial capsular release. Salvage: Postoperative EMG at 6 weeks if symptoms persist. Revision surgery for formal neurolysis and submuscular transposition if conservative management fails. |
| Recurrent Stiffness | 10% - 25% | Prevention: Meticulous hemostasis, use of surgical drains, immediate continuous postoperative ROM, and strict adherence to static-progressive splinting. Salvage: Re-evaluate patient compliance. Consider manipulation under anesthesia (MUA) within the first 6 weeks, or revision open/arthroscopic release after 6 months. |
| Recurrence of HO | 10% - 20% | Prevention: Mandatory prophylaxis with Indomethacin (75 mg SR daily x 3-6 weeks) OR single-dose localized radiation therapy (700-800 cGy) within 48 hours post-op. Salvage: Wait until soft tissues are completely quiescent (minimum 6 months), ensure normal inflammatory markers, and perform revision excision with dual prophylaxis. |
| Iatrogenic PLRI | 2% - 5% | Prevention: Keep anterior capsulectomy strictly anterior to the LUCL footprint on the lateral epicondyle. Repair any compromised lateral structures with suture anchors. Salvage: Bracing in pronation for 6 weeks. If symptomatic instability persists, formal LUCL reconstruction using a palmaris longus or triceps fascia autograft is required. |
| Postoperative Hematoma | 3% - 8% | Prevention: Deflate tourniquet prior to closure to achieve meticulous hemostasis. Routine use of closed suction drainage for 24-48 hours. Salvage: Early operative evacuation if the hematoma causes wound tension or severe pain, as retained blood acts as a potent scaffold for recurrent fibrosis and HO. |
Phased Post-Operative Rehabilitation Protocols
The technical success of an intraoperative elbow contracture release is entirely inextricably linked to the execution of the postoperative rehabilitation program. The biological tendency of the elbow is to rapidly form scar tissue; therefore, immediate, sustained, and aggressively managed motion is critical to maintaining the intraoperative gains.
Phase I: Immediate Postoperative Period (Weeks 0-2)
Pain control is the cornerstone of early rehabilitation. Without adequate analgesia, the patient will guard the joint, rendering physical therapy impossible. The use of an indwelling regional anesthesia catheter (e.g., supraclavicular or infraclavicular block) for the first 48 to 72 hours is highly recommended to facilitate immediate, painless motion.
After the initial 24 to 48 hours of immobilization in full extension (to allow for wound sealing and hematoma prevention), the bulky surgical dressing is removed. Active and active-assisted range-of-motion exercises are initiated immediately. Historically, Continuous Passive Motion (CPM) machines were utilized for up to 12 hours a day during this phase. However, modern evidence-based studies suggest there is no significant long-term benefit to the use of CPM compared to structured, patient-driven active protocols. Between therapy sessions and at night, the elbow is splinted. Extension splinting is most commonly utilized, as terminal extension is notoriously the most difficult motion to maintain postoperatively.
Phase II: Intermediate Rehabilitation (Weeks 2-6)
During this phase, supervised physical therapy continues two to three times a week, focusing on active and active-assisted ROM, capsular stretching, and gentle isometric strengthening. The splinting regimen becomes dynamic or static-progressive. The position of the splint is alternated based on the patient's specific residual deficits. If the patient struggles with flexion, a flexion-assist splint is worn during the day, while an extension splint is worn at night. Edema control through compression garments and retrograde massage is emphasized to prevent fluid-induced tissue resistance.
Phase III: Late Functional Phase (Weeks 6-12 and beyond)
At the 6-week mark, daytime splinting is generally discontinued to encourage unencumbered functional use of the extremity in activities of daily living. Strengthening exercises are progressed to include isotonic and light resistance training. However, static-progressive night splinting is strictly continued for a minimum of 12 weeks, and sometimes up to 6 months, to prevent the late recurrence of the contracture as the collagen matrix continues to remodel. Serial measurements of ROM are documented to ensure the patient is not losing ground; any regression warrants an immediate intensification of the splinting protocol.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for elbow contracture and heterotopic ossification has been shaped by several landmark studies and shifting clinical paradigms. A thorough understanding of this literature is essential for the academic orthopaedic surgeon.
Morrey et al. (1981) established the foundational biomechanical baseline with their seminal paper on the functional arc of motion. By evaluating the ROM required for 15 activities of daily living, they defined the 100-degree arc (30 to 130 degrees of flexion) and 100-degree rotational arc (50 degrees pronation/supination) that remains the universal target for all elbow reconstructive procedures today.
Regarding the surgical approach, the extensile lateral column approach, extensively described and popularized by Morrey and later refined by Mansat and Morrey (1998), remains the gold standard. Their outcome studies demonstrated that a single lateral incision could safely address both anterior and posterior pathology in over 80% of cases, drastically reducing the need for dual incisions and lowering the risk of wound complications.
The management of heterotopic ossification has seen a massive paradigm shift, driven by the work of Hastings and Graham (1994), who not only provided the most widely used classification system for HO but also challenged the dogma of delayed excision. Subsequent landmark studies by Garland (1991) and more recent systematic reviews by Lindenhovius et al. (2007) definitively demonstrated that early excision of HO (at 3 to 6 months, once fractures are united) does not increase the rate of recurrence compared to late excision (12 to 18 months), provided appropriate prophylaxis is utilized. This shift has saved countless patients from months of unnecessary disability and secondary joint degradation.
Clinical guidelines for HO prophylaxis are firmly established based on randomized controlled trials. The use of non-steroidal anti-inflammatory drugs (NSAIDs), specifically Indomethacin, was validated by Burd et al. (2001), showing equivalence to radiation therapy in preventing HO following high-risk trauma. Current guidelines mandate either a 3-to-6-week course of Indomethacin or a single 700 cGy dose of localized external beam radiation within 48 hours of surgery, with the choice often dictated by patient comorbidities (e.g., gastrointestinal risk factors contraindicating NSAIDs) and institutional availability.
