Elbow Arthroscopy: Loose Bodies & Osteochondritis Dissecans
Key Takeaway
Elbow arthroscopy is the gold standard for the removal of intra-articular loose bodies and the management of capitellar osteochondritis dissecans. This comprehensive guide details the biomechanical etiology, advanced imaging criteria, and step-by-step surgical techniques required for optimal outcomes. Emphasizing precise portal placement, fragment retrieval strategies, and evidence-based cartilage restoration, it provides orthopedic surgeons with a definitive framework for treating complex pediatric and adolescent elbow pathologies.
Comprehensive Introduction and Patho-Epidemiology
The advent and refinement of elbow arthroscopy have revolutionized the management of intra-articular pathology, transforming historically morbid open arthrotomies into minimally invasive, highly efficacious procedures. Among the myriad indications for elbow arthroscopy, the retrieval of intra-articular loose bodies and the management of osteochondritis dissecans (OCD) of the capitellum remain the most common and arguably the most successful applications. Patients afflicted by these pathologies typically present with a debilitating constellation of mechanical symptoms, including persistent deep-seated pain, intermittent catching, locking, and a mechanically blocked or globally limited range of motion (ROM). When these symptoms prove recalcitrant to conservative, non-operative management, a thorough diagnostic and therapeutic arthroscopic intervention is strictly indicated to restore joint kinematics and prevent progressive chondral wear.
Understanding the pathoanatomy and underlying etiology of loose bodies is paramount for comprehensive joint management. The operating surgeon must not merely extract the offending loose bodies but must meticulously identify and address the site of origin to mitigate recurrence and halt progressive joint degeneration. Osteocartilaginous loose bodies most frequently arise from discrete osteochondritic lesions—particularly OCD of the capitellum—or from osteochondral fractures resulting from acute lateral compression injuries, shear forces, or complex elbow dislocations. Alternatively, synovial pathologies such as primary synovial chondromatosis (a benign neoplastic process of the synovium) or secondary synovial chondromatosis (arising from underlying osteoarthritis) can generate dozens to hundreds of cartilaginous nodules that eventually ossify.
These loose bodies exhibit a distinct propensity to migrate and embed within the complex capsular recesses of the elbow. They are frequently sequestered in the dense fibrous tissue of the coronoid, radial, or olecranon fossae. Furthermore, minute loose bodies may remain occult within the tight confines of the olecranon-trochlear articulation or the radiocapitellar joint. Failure to systematically probe and clear these hidden recesses during arthroscopy invariably results in retained fragments, persistent postoperative mechanical symptoms, and the potential for iatrogenic third-body wear on the articular cartilage.
While both Panner disease and OCD affect the capitellum, they must be recognized as distinct clinical entities separated by patient demographics, underlying pathophysiology, and long-term prognostic outcomes. Panner disease is an idiopathic osteochondrosis characterized by diffuse involvement of the capitellum, occurring almost exclusively in pediatric patients aged 6 to 8 years. It involves a temporary, self-limiting disruption of the blood supply to the growing capitellum, leading to necrosis and subsequent complete regeneration with conservative management. In stark contrast, OCD develops in a more focal area of the capitellum in preadolescents or adolescents (typically 10 to 17 years old). At this developmental stage, the capitellum is approaching skeletal maturity, possesses a rapidly diminishing tenuous blood supply, and exhibits significantly less potential for spontaneous healing and remodeling, thereby frequently necessitating surgical intervention.
Biomechanics of Valgus Extension Overload
The etiology of capitellar OCD is intimately correlated with the biomechanics of the overhead throwing motion, specifically the phenomenon of "valgus extension overload." This condition is a hallmark injury in overhead athletes, including baseball pitchers, gymnasts, and racquet sport competitors. The pathophysiology is driven by the repetitive application of supraphysiologic forces across the elbow joint during specific phases of the throwing cycle.
During the late cocking and early acceleration phases of throwing, immense valgus torque is placed on the elbow. This torque generates significant medial tension, heavily stressing the anterior band of the ulnar collateral ligament (UCL). Concurrently, this valgus force translates into severe lateral compression, driving the radial head forcefully into the capitellum. The radiocapitellar joint, which normally acts as a secondary stabilizer to valgus stress, is forced to bear an excessive load, particularly if the UCL is attenuated or insufficient.
Over time, this repetitive microtrauma leads to focal subchondral bone ischemia within the capitellum. The subchondral bone undergoes microfragmentation, leading to a loss of structural support for the overlying articular cartilage. As the mechanical integrity of the subchondral plate fails, the cartilage undergoes fissuring, softening, and eventual detachment, creating an unstable osteochondral fragment. The resulting loose body and the corresponding capitellar defect profoundly alter the contact mechanics of the radiocapitellar joint, initiating a cascade of localized degenerative changes if left unaddressed.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of elbow surgical anatomy is the absolute prerequisite for safe and effective arthroscopy. The elbow is a highly congruent, constrained hinge joint comprised of three distinct articulations: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The osseous architecture is enveloped by a relatively non-compliant joint capsule with a remarkably small volumetric capacity, typically accommodating only 15 to 25 mL of fluid before capsular distension maximizes. This limited volume dictates strict fluid management protocols during arthroscopy to prevent catastrophic extravasation and subsequent neurovascular compromise.
The anterior compartment of the elbow houses the coronoid and radial fossae. The coronoid fossa, located proximal to the trochlea, accommodates the coronoid process during terminal flexion. The radial fossa, situated proximal to the capitellum, receives the radial head. These fossae are prime locations for loose body sequestration, often concealed by a hyperplastic synovial fringe or dense fibrous bands. The posterior compartment is dominated by the olecranon fossa, a deep depression on the posterior humerus that accommodates the olecranon tip during terminal extension. Osteophytes and loose bodies frequently populate this region in the setting of valgus extension overload, leading to posterior impingement and a mechanical block to extension.
Neurovascular Proximity and Portal Anatomy
The establishment of arthroscopic portals carries an inherent risk to the major neurovascular structures traversing the elbow. Precise anatomic landmarking and meticulous technique are non-negotiable.
The Proximal Anteromedial (PAM) Portal is typically established 2 cm proximal to the medial epicondyle, just anterior to the intermuscular septum. This portal provides an excellent panoramic view of the anterior compartment. The medial antebrachial cutaneous nerve and the median nerve are at risk; however, maintaining contact with the anterior humerus during trocar insertion minimizes this danger.
The Anterolateral (AL) Portal is located 3 cm distal and 1 cm anterior to the lateral epicondyle. It is the primary working portal for anterior compartment pathology. The radial nerve is the most vulnerable structure here, particularly if the joint is not adequately distended or if the trocar strays anteriorly or medially.
The Direct Posterior or Posterocentral Portal is placed 3 cm proximal to the olecranon tip, directly through the triceps tendon. It provides unparalleled access to the olecranon fossa and posterior gutter. The ulnar nerve, located in the cubital tunnel medially, is the primary structure at risk, necessitating careful palpation and avoidance of medial deviation during establishment.
The Posterolateral (PL) Portal is situated just proximal to the tip of the olecranon, along the lateral border of the triceps. This portal is utilized for visualization of the posterior compartment and the posterolateral gutter. The posterior antebrachial cutaneous nerve is in proximity, but major motor nerves are generally safe if standard landmarks are respected.
Exhaustive Indications and Contraindications
The decision to proceed with elbow arthroscopy for loose body removal or OCD management must be predicated on a rigorous clinical evaluation and a failure of appropriate non-operative modalities. While arthroscopy is highly successful, it is not without risk, and careful patient selection is critical.
Indications for arthroscopic loose body removal include persistent mechanical symptoms such as catching, locking, or a hard block to motion that significantly impairs activities of daily living or athletic participation. In the context of OCD, indications are heavily influenced by the stability of the lesion, the status of the capitellar physis, and the presence of radial head engagement. Stable OCD lesions in patients with open physes are typically managed conservatively with strict rest. However, unstable lesions, characterized by fluid interposition on MRI, articular collapse, or complete detachment, necessitate surgical intervention regardless of skeletal maturity.
Contraindications must be carefully weighed. Absolute contraindications include active localized or systemic infection, severe distortion of normal bony or soft tissue anatomy (which precludes safe portal placement), and an inability of the patient to comply with rigorous postoperative rehabilitation. Relative contraindications include a prior ulnar nerve transposition, which alters the predictable anatomy of the medial elbow and places the nerve at extreme risk during anteromedial portal establishment.
Table: Indications and Contraindications for Elbow Arthroscopy
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Absolute Indications | Mechanically symptomatic loose bodies | Prevents third-body wear and addresses locking/catching. |
| Unstable OCD lesions (ICRS Grade 3 or 4) | High risk of progression to advanced osteoarthritis; requires fixation or excision. | |
| Symptomatic synovial chondromatosis | Requires synovectomy and removal of cartilaginous nodules to prevent joint destruction. | |
| Relative Indications | Stable OCD lesions failing 6 months of rest | Prolonged conservative failure warrants marrow stimulation to induce healing. |
| Mild to moderate flexion/extension contractures | Arthroscopic capsular release can be performed concomitantly with loose body removal. | |
| Absolute Contraindications | Active intra-articular or periarticular infection | Risk of systemic dissemination and fulminant septic arthritis. |
| Severe anatomic distortion (e.g., massive heterotopic ossification) | Precludes safe portal establishment; high risk of iatrogenic neurovascular injury. | |
| Relative Contraindications | Prior ulnar nerve transposition | Unpredictable medial anatomy; requires mini-open nerve identification before medial portal placement. |
| Severe capsular contracture (<30 degrees total arc of motion) | Minimal capsular volume increases the risk of neurovascular injury during trocar insertion. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful elbow arthroscopy. Standard radiographic evaluation is the mandatory first line of diagnosis but possesses significant limitations regarding sensitivity. According to seminal data by Andrews and Carson, only approximately 38% of loose bodies are obvious on standard plain radiographs, largely due to their frequently cartilaginous nature or superimposition over complex bony structures. Radiographic examination of the adolescent elbow must include an anteroposterior (AP) view, a true lateral view, and an AP view with the elbow in 45 degrees of flexion to adequately profile the posterior aspect of the capitellum, where OCD lesions frequently manifest.

Figure 52-64 A: Lateral radiograph of the elbow demonstrating a large anterior loose body and an associated defect of the radial head.

Figure 52-64 B: Anteroposterior (AP) radiograph revealing a large loose body lodged within the coronoid fossa.
To enhance diagnostic accuracy, Computed Tomography (CT) arthrography is highly recommended, as it detects up to 72% of loose bodies, providing precise three-dimensional localization and characterizing the size and number of the fragments. Magnetic Resonance Imaging (MRI) remains the definitive imaging modality of choice, particularly for identifying purely cartilaginous bodies, evaluating the integrity of the articular surfaces, and determining the stability of OCD lesions.
Kijowski and DeSmet outlined four critical MRI findings that pathognomonically dictate an unstable OCD lesion requiring surgical intervention:
1. A line of high-signal intensity deep to the fragment on T2-weighted images, indicating synovial fluid interposition.
2. An articular fracture indicated by high-signal intensity passing completely through the subchondral bone plate.
3. A focal osteochondral defect presenting as an empty crater.
4. A fluid-filled subchondral cyst measuring 5 mm or greater deep to the lesion.
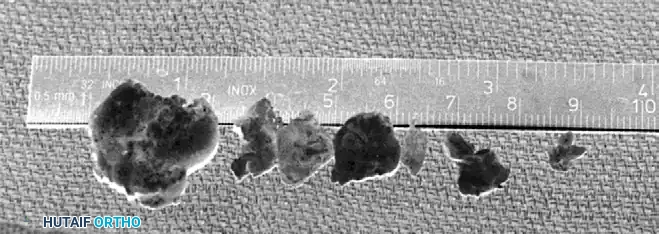
Figure 52-64 C: Postoperative radiograph following the successful removal of loose bodies and resection of the radial head defect.

Figure 52-64 D: Additional postoperative imaging confirming complete clearance of the anterior and posterior compartments.
Patient Positioning and Operating Room Setup
Patient positioning significantly influences surgical access, fluid dynamics, and the ease of intraoperative manipulation. The two most common positions are the lateral decubitus position and the prone position.
In the Lateral Decubitus Position, the patient is placed on their non-operative side. The operative arm is supported over a specialized bolster or an arm holder, allowing the elbow to hang freely at 90 degrees of flexion. This position provides excellent access to both the anterior and posterior compartments and allows for dynamic assessment of joint stability. A non-sterile tourniquet is applied high on the brachium.
The Prone Position is favored by many surgeons for its unparalleled access to the posterior compartment, which is particularly beneficial for extensive olecranon fossa debridement. The arm is draped over a radiolucent arm board. Regardless of the position chosen, all bony landmarks (medial and lateral epicondyles, olecranon, radial head) and the course of the ulnar nerve must be meticulously marked with a surgical pen prior to the instillation of fluid or the inflation of the tourniquet.
Fluid management is a critical safety parameter. The elbow capsule has a limited volume, and excessive fluid extravasation can rapidly lead to compartment syndrome or severe neuropraxia. The surgeon must maintain low pump pressures (typically 30-40 mmHg) and utilize gravity flow whenever possible. The use of an arthroscopic pump should be continuously monitored, and the procedure must be expedited if significant soft tissue swelling is observed.
Step-by-Step Surgical Approach and Fixation Technique
Elbow arthroscopy for loose body removal and OCD management demands meticulous portal placement, precise instrumentation, and an organized, systematic approach to joint evaluation.
Diagnostic Sweep and Loose Body Retrieval
The procedure commences with the establishment of the Proximal Anteromedial (PAM) portal. The joint is first distended with 15-20 mL of normal saline injected through the soft spot (center of the triangle formed by the lateral epicondyle, radial head, and olecranon). The PAM portal is then established using a "nick and spread" technique with a No. 11 blade, followed by blunt dissection with a hemostat to the capsule, and finally, the insertion of a blunt trocar. This minimizes the risk to the median nerve.
Once the arthroscope is introduced, a systematic diagnostic round of the anterior compartment is performed, evaluating the coronoid fossa, the anterior radiocapitellar joint, and the anterior capsule. An Anterolateral (AL) working portal is then established under direct intra-articular visualization using an outside-in spinal needle localization technique.
Loose bodies embedded in the coronoid or radial fossae often require the release of overlying hyperplastic fibrous tissue. An arthroscopic shaver or radiofrequency wand is utilized to carefully free these bodies from the synovium. When large bodies are located in difficult-to-reach sites, they must be mobilized.
The surgeon may employ the Uncoupling Technique: uncoupling the arthroscope from its sheath, retracting the scope a few millimeters, and using the blunt edge of the sheath to physically push the loose body into a favorable position. Additionally, fluid management is crucial; if fluid turbulence causes the loose body to float away from the grasper (the "snow globe effect"), the surgeon must reduce or completely turn off the inflow to allow the fragment to settle into the dependent portion of the joint.
Extraction strategies vary based on fragment size. Small fragments are easily removed via standard arthroscopic graspers through the working cannula. Large fragments occasionally prove too large to be extracted through a standard portal. These can be fragmented in situ using an arthroscopic burr and removed piecemeal. Alternatively, the Kocher Clamp Technique can be employed: large bodies are left in place until the conclusion of the intra-articular work. They are then removed by longitudinally extending the capsular incision and extracting the intact fragment with a Kocher clamp. This delayed extraction prevents premature fluid extravasation into the anterior soft tissues, thereby decreasing the risk of neurovascular compromise during the remainder of the procedure.

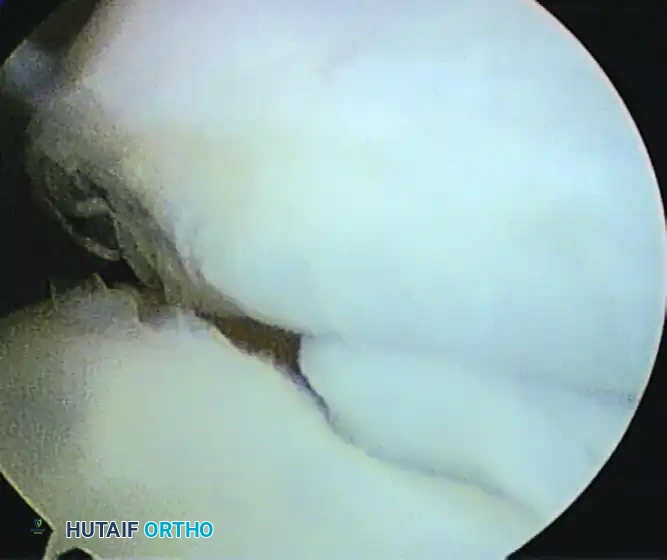
Figure 52-65 A: Arthroscopic view of a large, obstructing loose body situated in the anterior elbow compartment.

Figure 52-65 B: The anterior compartment visualized after successful extraction, demonstrating a decompressed and clear joint space.
Management of Osteochondritis Dissecans (OCD)
Following the clearance of loose bodies, attention is directed to the capitellum. Surgical decision-making relies heavily on accurate arthroscopic grading of the lesion, utilizing systems such as the International Cartilage Repair Society (ICRS) Grading scale.
Figure 52-66: Arthroscopic visualization of a partially detached osteochondritis dissecans (OCD) lesion of the capitellum, demonstrating articular cartilage fissuring and instability.
During arthroscopic evaluation, the size, containment, and radial head engagement of the lesion are the most critical prognostic factors dictating the specific surgical technique. To assess radial head engagement, the surgeon places the elbow in extension, pronates and supinates the forearm, and then ranges the elbow through a full arc of motion under direct visualization. If the radial head drops into the capitellar defect after initial debridement, the biomechanics of the joint are severely compromised, necessitating advanced reconstructive techniques.
Debridement and Microfracture: For smaller, contained lesions (involving <50% of the articular surface) without radial head engagement, debridement and marrow stimulation are indicated. The unstable fragment is excised, and the sclerotic base is aggressively debrided with a curette or burr to bleeding subchondral bone. Microfracture awls or a small drill are then used to penetrate the subchondral plate at 2-3 mm intervals. This stimulates a marrow-healing response, leading to the formation of a fibrocartilage patch that fills the defect.
Fragment Fixation: This is attempted if the fragment is large, acute, and possesses sufficient attached subchondral bone to allow for osseous union. The crater is debrided, the fragment is reduced, and fixation is achieved using headless compression screws or bioabsorbable darts. However, follow-up studies show variable success, as most fragments exhibit advanced chondral degeneration or lack adequate bone stock for secure fixation.
Osteochondral Autograft Transfer System (OATS): This advanced technique is strictly indicated for large lesions (>50% involvement), lesions with a loss of lateral containment, or those demonstrating radial head engagement. Transferring a cylindrical osteochondral plug (typically harvested from the non-weight-bearing periphery of the ipsilateral knee, such as the lateral femoral condyle above the sulcus terminalis) restores the articular congruity and lateral buttress. This prevents progressive degenerative joint changes and provides the best opportunity for the athlete to return to high-demand, overhead activities. The procedure requires specialized instrumentation to core out the capitellar defect and press-fit the harvested graft flush with the surrounding native cartilage.
Complications, Incidence Rates, and Salvage Management
While elbow arthroscopy is generally safe, the margin for error is exceptionally narrow. Complications can be devastating, primarily due to the dense concentration of neurovascular structures and the joint's propensity for postoperative stiffness.
The most feared complication is iatrogenic nerve injury. Neuropraxia can result from direct trocar trauma, excessive traction, or, most commonly, fluid extravasation leading to a localized compartment syndrome. The ulnar nerve is most frequently injured during the establishment of posteromedial portals or aggressive posterior capsular releases. The radial nerve is at risk during anterolateral portal placement, and the median nerve is vulnerable during anteromedial access.
Arthrofibrosis is another common complication, often resulting from inadequate postoperative rehabilitation, prolonged immobilization, or excessive intraoperative soft tissue trauma. Retained loose bodies are a frequent cause of persistent postoperative symptoms, highlighting the necessity of a systematic and exhaustive diagnostic sweep of all joint recesses.
In cases of catastrophic failure of OCD management, such as a failed OATS procedure or massive capitellar collapse, salvage options are severely limited. In older, low-demand patients, total elbow arthroplasty may be considered. In younger, high-demand patients, massive osteochondral allograft reconstruction or radiocapitellar arthroplasty remain the only viable salvage pathways, though both carry significant long-term limitations regarding weight-bearing and athletic participation.
Table: Complications, Incidence, and Salvage Management
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Transient Neuropraxia | 2% - 5% | Fluid extravasation; tourniquet palsy; mild retractor/trocar trauma. | Observation; typically resolves spontaneously within 3-6 months. Gabapentinoids for neuropathic pain. |
| Permanent Nerve Transection | < 0.5% | Direct laceration by scalpel, trocar, or aggressive motorized shaver use. | Immediate microsurgical nerve repair or grafting. Tendon transfers for permanent motor deficits. |
| Arthrofibrosis / Stiffness | 5% - 10% | Prolonged immobilization; inadequate physical therapy; severe preoperative contracture. | Aggressive physical therapy; dynamic splinting. If recalcitrant >6 months, open or arthroscopic capsular release. |
| Retained Loose Bodies | 1% - 3% | Failure to probe hidden recesses (e.g., radiocapitellar joint, olecranon fossa). | Repeat arthroscopy for extraction; mandatory use of 70-degree scope for blind spots. |
| OATS Graft Failure | 5% - 15% | Graft subsidence; avascular necrosis of the plug; failure of integration. | Revision with osteochondral allograft; radiocapitellar arthroplasty in severe, older cases. |
| Compartment Syndrome | < 0.1% | Excessive pump pressure (>50 mmHg); prolonged surgical time; capsular defects. | Immediate cessation of procedure; emergent open fasciotomies of the forearm and arm. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following elbow arthroscopy must be instituted immediately and progressed systematically to prevent arthrofibrosis, a notoriously common and debilitating complication following elbow trauma and surgery. The protocol is tailored based on the specific procedures performed; isolated loose body removal allows for rapid progression, whereas OCD microfracture or OATS requires a period of protected weight-bearing to ensure graft incorporation.
Immediate Phase (Days 1-7)
The primary goals of the immediate phase are the control of postoperative edema, pain management, and the early initiation of motion to prevent capsular adhesions. The patient is typically placed in a bulky, soft compressive dressing. For isolated loose body removal, the patient is encouraged to move the elbow actively within the confines of the dressing as soon as pain and swelling permit. Cryotherapy and elevation are utilized aggressively. For OCD procedures involving microfracture or OATS, ROM is permitted, but the joint is protected in a hinged brace locked to prevent terminal extension, thereby unloading the radiocapitellar joint.
Intermediate Phase (Weeks 2-6)
Sutures are removed at 10 to 14 days, and formal physical therapy is initiated. The focus shifts to restoring full active and active-assisted ROM. Joint mobilizations are employed to address any residual capsular tightness. Flexibility and progressive isometric strengthening exercises for the biceps, triceps, and forearm musculature are initiated once joint effusion and acute pain are sufficiently diminished. In patients who underwent OCD marrow stimulation, weight-bearing through the upper extremity (e.g., push-ups, heavy lifting) remains strictly prohibited to protect the maturing fibrocartilage clot.
Advanced Strengthening and Return to Play (Weeks 6-12+)
Once full, painless ROM is achieved, the protocol advances to isotonic and dynamic strengthening. For overhead athletes, a structured, interval throwing program is initiated around week 8 to 12, depending on the extent of the initial pathology and the surgical intervention. Return to competitive play is contingent upon the restoration of normal strength (compared to the contralateral limb), the absence of pain or effusion during sport-specific activities, and radiographic evidence of graft incorporation in cases of OATS. Premature return to throwing significantly increases the risk of recurrent valgus extension overload and catastrophic failure of the surgical intervention.
Summary of Landmark Literature and Clinical Guidelines
The evolution of elbow arthroscopy and the current standard of care for loose bodies and OCD are deeply rooted in several landmark studies that have shaped orthopedic clinical guidelines.
The seminal work by Andrews and Carson established the foundational understanding of the limitations of plain radiography in detecting cartilaginous loose bodies, demonstrating a mere 38% detection rate. This study unilaterally shifted the diagnostic paradigm toward the routine use of advanced imaging, specifically CT arthrography and MRI, for comprehensive preoperative planning.
In the realm of OCD management, Takahara et al. provided the definitive framework for surgical decision-making. In their comprehensive study of 106 patients, they validated the distinction between stable and unstable lesions. They demonstrated that stable lesions in patients with open physes have a high propensity for spontaneous healing with strict rest, whereas unstable lesions or those in patients with closed physes uniformly require surgical intervention to prevent progressive osteoarthritis.
Furthermore, Kijowski and DeSmet defined the critical MRI criteria for OCD instability, providing radiologists and surgeons with a reliable, non-invasive tool to predict which lesions will fail conservative management. Their identification of fluid interposition and subchondral cysts as pathognomonic signs of instability remains a cornerstone of modern clinical practice.
Finally, the prognostic factors dictating the choice of surgical intervention for OCD were elucidated by Ahmad et al. They identified that capitellar defects encompassing more than 50% of the articular surface, a loss of lateral buttress containment exceeding 6 to 7 mm, and, most critically, the engagement of the radial head into the defect are poor prognostic indicators for simple debridement and microfracture. This research directly supports the clinical guideline that large, uncontained, or engaging lesions mandate structural restoration via Osteochondral Autograft Transfer System (OATS) to restore joint kinematics and permit a return to high-demand activities.
