Elbow Contracture Release: Medial Over-the-Top Approach Masterclass
Key Takeaway
This masterclass details the medial over-the-top approach for elbow contracture release. Fellows will learn intricate surgical anatomy, meticulous patient positioning, and a step-by-step intraoperative execution, including ulnar nerve management and capsule excision. We cover critical pearls, potential pitfalls, and comprehensive postoperative care, ensuring a thorough understanding of this challenging procedure for restoring elbow motion.
Comprehensive Introduction and Pathophysiology
Welcome, esteemed colleagues and surgical fellows, to this advanced masterclass on the operative management of the stiff elbow. Today, we delve into the intricacies of elbow contracture release utilizing the medial over-the-top approach. The human elbow is a highly constrained, complex hinge joint, and its propensity for extreme stiffness following trauma, inflammation, or degenerative processes is well documented in orthopedic literature. Restoring a functional arc of motion—widely accepted as 30 to 130 degrees of flexion-extension and 50 degrees of both pronation and supination—is paramount for a patient’s independence in activities of daily living. When nonoperative modalities have been exhausted, surgical intervention becomes necessary to meticulously address the extrinsic soft tissue and bony impediments that tether the joint.
The pathophysiology of elbow contracture is broadly categorized into intrinsic and extrinsic etiologies, though a combination of both is frequently encountered in chronic cases. Intrinsic stiffness arises from intra-articular pathology, such as articular cartilage degradation, intra-articular malunion, or loose bodies. Extrinsic stiffness, which the medial over-the-top approach is uniquely designed to address, stems from extra-articular structures. This includes severe capsular contracture, collateral ligament thickening, heterotopic ossification (HO), and periarticular osteophyte formation, particularly at the coronoid and olecranon processes. The fibrotic cascade following elbow trauma leads to a thickened, non-compliant capsule that mechanically blocks motion.
The medial over-the-top approach has revolutionized our ability to manage these complex extrinsic contractures. Historically, surgeons relied on limited medial or lateral windows, often requiring combined or bilateral incisions to adequately address both anterior and posterior pathology. The over-the-top technique provides unparalleled, extensile access to the anterior and posterior compartments of the ulnohumeral joint through a single medial incision. By elevating the flexor-pronator mass and anterior capsule off the distal humerus, we can access the anterior joint space; similarly, by tracking posteriorly, we can clear the olecranon fossa.
Critically, this approach offers direct visualization, neurolysis, and transposition of the ulnar nerve, which is often tethered or compressed in the setting of a stiff elbow. Furthermore, it allows for the meticulous preservation of the anterior bundle of the medial collateral ligament (AMCL), ensuring that post-release valgus stability is not compromised. Our goal throughout this procedure is not merely the blunt resection of tissue, but the anatomic restoration of the joint's kinematic envelope through precise, subperiosteal dissection and targeted osteophyte excision.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the medial elbow's surgical anatomy is the bedrock of a safe and effective over-the-top release. This region is a dense confluence of critical osteology, ligamentous stabilizers, dynamic muscle forces, and unforgiving neurovascular structures. The foundational bony landmark is the medial epicondyle, which serves as the origin for the flexor-pronator muscle mass and the medial collateral ligament. Extending proximally is the medial supracondylar ridge of the humerus, our primary gateway for initiating the subperiosteal, extracapsular dissection. Distally, the proximal ulna presents the coronoid process anteriorly and the olecranon posteriorly. Osteophytes frequently form at the tip of the coronoid, impinging in the coronoid fossa to block flexion, while posterior osteophytes on the olecranon impinge in the olecranon fossa to block extension.
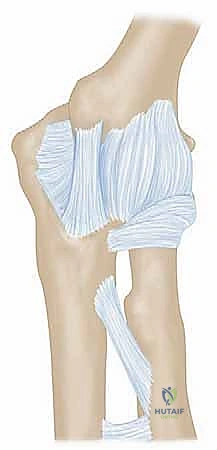
The ligamentous anatomy is dominated by the Medial Collateral Ligament (MCL) complex, the primary restraint to valgus stress. It is divided into three distinct bundles. The anterior bundle (AMCL) is the most critical structure to preserve during this approach. It originates from the anteroinferior surface of the medial epicondyle—distinct from the condylar elements of the trochlea—and inserts broadly onto the sublime tubercle of the coronoid process. The posterior bundle is essentially a thickening of the posterior capsule, becoming taut in flexion, while the transverse bundle (Cooper's ligament) spans from the olecranon to the coronoid and contributes minimally to overall stability. Identifying the exact footprint of the AMCL is mandatory before any capsular resection is performed.
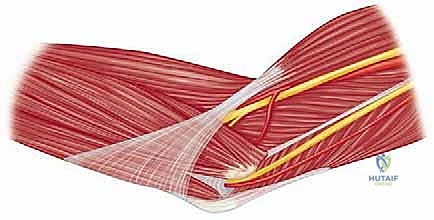
Overlying these static stabilizers is the dynamic flexor-pronator mass. From proximal to distal, this includes the pronator teres, flexor carpi radialis, palmaris longus, flexor carpi ulnaris (FCU), and the deeper flexor digitorum superficialis. The FCU is of particular surgical interest as it possesses two heads—a humeral head from the medial epicondyle and an ulnar head from the proximal ulna—between which the ulnar nerve passes to enter the cubital tunnel. During the over-the-top approach, parts of this musculature must be carefully elevated or retracted to expose the underlying capsule without devascularizing the tissue or compromising its functional integrity.

Neurovascularly, the ulnar nerve commands our utmost respect. It courses posterior to the medial intermuscular septum, rests in the retroepicondylar groove, and dives between the heads of the FCU. It is highly vulnerable to iatrogenic injury during medial elbow surgery, particularly in revision cases where it may be encased in scar tissue or distorted by heterotopic bone. Additionally, the medial antebrachial cutaneous nerve (MACN) presents a variable branching pattern in the subcutaneous tissue overlying the medial epicondyle. Failure to identify and protect the MACN during the initial exposure can lead to painful postoperative neuromas that severely compromise patient satisfaction.
Exhaustive Indications and Contraindications
Patient selection is the most critical preoperative variable in predicting the success of an elbow contracture release. The primary indication for surgical intervention is a persistent, functionally limiting loss of elbow motion that has proven refractory to a dedicated, protracted course of nonoperative management. Typically, we require a minimum of six months of conservative therapy—including static progressive splinting, dynamic bracing, and aggressive physical therapy—before considering surgical release. The medial over-the-top approach is specifically indicated when the contracture is primarily extrinsic in nature, driven by anterior and posterior capsular fibrosis, and accompanied by medial or anterior osteophytes.
This approach is the gold standard when the patient presents with concomitant ulnar neuropathy. The incidence of ulnar nerve symptoms in patients with severe elbow stiffness is notably high, as the nerve becomes tethered in the fibrotic cubital tunnel during flexion. The medial approach allows for a simultaneous, comprehensive ulnar nerve neurolysis and anterior transposition, addressing both the mechanical block to motion and the compressive neuropathy in a single surgical setting. Furthermore, it is indicated when the lateral compartment (radiohumeral joint) is largely spared from severe heterotopic ossification or degenerative changes, as the medial approach provides limited access to the lateral structures.
Conversely, there are strict contraindications to this procedure. Active joint infection is an absolute contraindication, requiring eradication prior to any reconstructive efforts. Severe, end-stage intrinsic joint destruction—such as advanced post-traumatic osteoarthritis with complete loss of the articular cartilage—is a relative contraindication for an isolated release; these patients are often better served by total elbow arthroplasty or interpositional arthroplasty, depending on their age and functional demands. Additionally, if the primary pathology is isolated to the lateral compartment, such as a massive lateral column heterotopic ossification bridge or severe radiohumeral impingement, an isolated medial approach will be insufficient, and a lateral or combined approach must be employed.
| Parameter | Indications for Medial Over-the-Top Approach | Contraindications |
|---|---|---|
| Clinical Status | Failure of >6 months of nonoperative management | Active local or systemic infection |
| Pathology Type | Extrinsic capsular contracture, prominent anterior/posterior osteophytes | Severe intrinsic articular destruction (requires arthroplasty) |
| Neurologic | Concomitant ulnar neuropathy requiring decompression/transposition | Isolated radial nerve pathology |
| Anatomic Focus | Predominantly medial, anterior, and posterior bony/soft tissue blocks | Massive lateral heterotopic ossification (requires lateral approach) |
| Patient Factors | Motivated patient, capable of strict postoperative rehabilitation | Non-compliant patient, severe uncontrolled spasticity |
Preoperative Planning, Imaging, and Patient Positioning
Before the patient enters the operating theater, meticulous preoperative planning serves as the blueprint for surgical success. The diagnostic workup begins with a comprehensive clinical assessment. We quantify the exact degrees of flexion, extension, pronation, and supination, noting a firm versus a soft endpoint, which helps differentiate between bony and soft-tissue blocks. A rigorous neurovascular examination is mandatory, with specific attention paid to the ulnar nerve. We assess for intrinsic muscle wasting, sensory deficits in the ulnar distribution, and a positive Tinel's sign at the cubital tunnel. Documenting these baseline deficits is crucial for both surgical planning and medicolegal protection.
Imaging is the cornerstone of our preoperative strategy. Standard anteroposterior (AP) and lateral radiographs provide an initial overview of joint congruity, the presence of loose bodies, and gross osteoarthritic changes. The lateral view is particularly valuable for identifying osteophytes on the coronoid process and the tip of the olecranon. However, plain films often underestimate the extent of heterotopic ossification. Therefore, a Computed Tomography (CT) scan with 3D reconstructions is considered indispensable for complex contractures. The CT scan allows for precise, three-dimensional mapping of osteophytes and heterotopic bone, enabling the surgeon to mentally template the exact volume and location of bony resection required to restore the kinematic envelope.
Patient positioning must be executed with flawless precision to ensure optimal exposure and prevent iatrogenic nerve injury during the prolonged procedure. Under general anesthesia, often supplemented with a regional brachial plexus block for postoperative analgesia, the patient is positioned supine. The operative arm is extended onto a specialized radiolucent hand table. We place two folded towels or a gel bump beneath the ipsilateral scapula; this slight elevation of the shoulder girdle allows the humerus to lie perfectly flat against the arm board, preventing the elbow from dropping into a dependent position and significantly improving access to the medial compartment.
A sterile tourniquet is applied high on the brachium to ensure a bloodless field, which is critical for identifying the ulnar nerve and microvascular structures. The shoulder must maintain free external rotation to allow the surgeon to access the posterior aspect of the elbow joint seamlessly. Finally, the fluoroscopy C-arm is positioned on the contralateral side of the table, ensuring it can be brought into the field smoothly to obtain true AP and lateral views intraoperatively. This real-time imaging is vital for confirming the complete excision of osteophytes and verifying that no subtle bony blocks remain at the extremes of motion.
Step-by-Step Surgical Approach and Technique
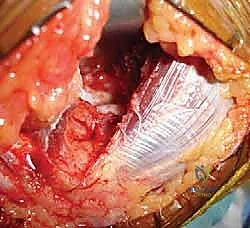
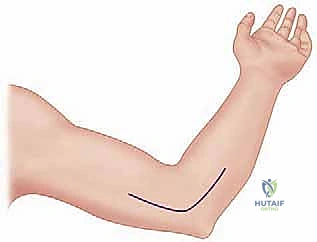
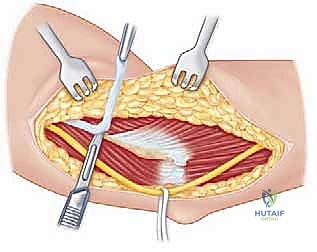
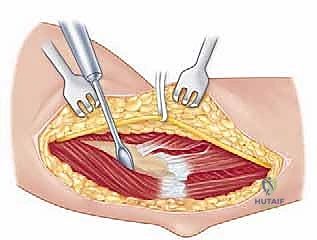
The execution of the medial over-the-top approach demands patience, meticulous hemostasis, and a deep respect for the regional anatomy. We begin with a longitudinal midline medial skin incision, centered over the medial epicondyle, extending approximately 6 to 8 centimeters proximally along the supracondylar ridge and an equal distance distally over the flexor-pronator mass. As we deepen the incision through the subcutaneous tissue, extreme care is taken to identify and mobilize the branches of the medial antebrachial cutaneous nerve (MACN). These branches are delicately dissected, protected with vessel loops, and retracted anteriorly to prevent painful postoperative neuromas.
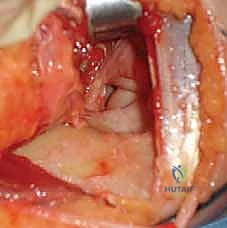
The first major definitive step is the identification and mobilization of the ulnar nerve. We locate the medial intermuscular septum proximally and trace it down to the epicondyle. The fascia overlying the cubital tunnel is incised, and the ulnar nerve is identified as it courses posterior to the septum. Using blunt dissection and tenotomy scissors, the nerve is carefully freed from its bed, extending proximally to the Arcade of Struthers and distally through the two heads of the flexor carpi ulnaris. Once fully mobilized, the nerve is protected with a Penrose drain. The medial intermuscular septum is then completely excised to prevent any kinking or tethering of the nerve when it is later transposed anteriorly.
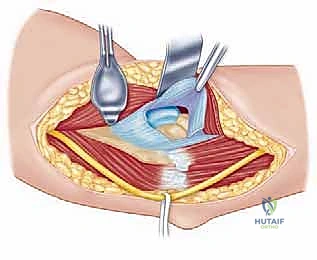
With the ulnar nerve safe, we commence the "over-the-top" dissection. We identify the anterior border of the flexor-pronator mass at its origin on the medial epicondyle. Using a periosteal elevator or a scalpel, we carefully elevate the anterior capsule and the brachialis muscle off the anterior aspect of the distal humerus, working subperiosteally from medial to lateral. This dissection sweeps across the anterior humerus, effectively going "over the top" of the joint. Retractors are placed anteriorly to protect the brachial artery and median nerve. We then perform a comprehensive anterior capsulectomy, excising the thickened, fibrotic capsule to expose the anterior joint space, the radiocapitellar joint, and the coronoid process.


Once the anterior joint is visualized, we address the bony blocks. Osteophytes on the coronoid process and within the coronoid fossa are meticulously excised using a combination of rongeurs, osteotomes, and a high-speed burr. Throughout this anterior release, the surgeon must be acutely aware of the anterior bundle of the MCL, which lies just inferior to our dissection plane. The AMCL must remain pristine and attached to the sublime tubercle. Following the anterior release, attention is turned posteriorly. The triceps is elevated off the posterior humerus, and a posterior capsulectomy is performed. The olecranon fossa is cleared of all fibrotic tissue and heterotopic bone, and the tip of the olecranon is frequently resected to ensure full extension.


After both anterior and posterior releases are complete, the elbow is gently manipulated to assess the newly achieved range of motion. We aim for a smooth, unimpeded arc from 0 degrees of extension to at least 130 degrees of flexion. Fluoroscopy is utilized to confirm the adequacy of the bony resections. The ulnar nerve is then transposed anteriorly, typically into a subcutaneous or subfascial pocket, ensuring it lies without tension or kinking throughout the full arc of motion. Meticulous hemostasis is achieved following tourniquet deflation, a closed suction drain is placed, and the wound is closed in a layered fashion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, elbow contracture release carries a recognized profile of postoperative complications. The surgeon must be prepared to identify and manage these effectively. The most frequent and concerning complication is ulnar neuropathy, which can occur in up to 10-15% of cases, even with careful neurolysis and transposition. This can result from excessive traction during the procedure, devascularization of the nerve, or compression within the new transposition bed due to hematoma or tight fascial slings. Prevention relies on extensive proximal and distal mobilization and ensuring a tension-free transposition. If postoperative neuropathy occurs and fails to improve with observation and steroids, a revision exploration may be mandated.
Heterotopic ossification (HO) recurrence is another significant threat, particularly in post-traumatic stiff elbows or patients with central nervous system injuries. The surgical trauma of the release itself can stimulate a new wave of osteogenesis. To mitigate this risk, meticulous surgical technique—specifically minimizing muscle trauma and achieving absolute hemostasis—is required. Postoperatively, prophylaxis is strongly recommended for high-risk patients, utilizing either a course of non-steroidal anti-inflammatory drugs (NSAIDs) like Indomethacin or single-dose localized radiation therapy within 72 hours of surgery.
Iatrogenic instability is a devastating complication resulting from the inadvertent transection or over-release of the anterior bundle of the medial collateral ligament (AMCL). This manifests as gross valgus instability and a loss of the ulnohumeral articulation's congruity. The surgeon must constantly orient themselves to the medial epicondyle and the sublime tubercle to protect this structure. If the AMCL is compromised intraoperatively, it must be immediately repaired using suture anchors or transosseous tunnels. If instability is noted postoperatively, the patient may require a formal MCL reconstruction using an autograft.
| Complication | Estimated Incidence | Preventative Strategy | Salvage / Management |
|---|---|---|---|
| Ulnar Neuropathy | 5% - 15% | Meticulous neurolysis, excision of intermuscular septum, tension-free transposition | Corticosteroids, gabapentinoids; Revision exploration/neurolysis if refractory |
| Recurrent Stiffness | 10% - 20% | Aggressive early CPM, static progressive splinting, adequate initial surgical release | Manipulation under anesthesia (rarely), Revision open/arthroscopic release |
| Heterotopic Ossification | 5% - 10% | Atraumatic tissue handling, Indomethacin (75mg SR daily x 3-6 weeks), Radiation (700 cGy) | Observation until mature (12-18 months), then revision excision if symptomatic |
| Iatrogenic Instability | < 2% | Strict identification and preservation of the AMCL footprint | Intraoperative primary repair; Postoperative formal MCL reconstruction |
| Wound Breakdown / Infection | 2% - 5% | Meticulous hemostasis, drain usage, layered closure, MACN protection | Local wound care, oral/IV antibiotics; Surgical debridement for deep infection |
Phased Postoperative Rehabilitation Protocols
The surgical release is only the first half of the battle; the ultimate success of an elbow contracture release is heavily dependent on a rigorous, highly structured postoperative rehabilitation protocol. The immediate postoperative phase (Days 0 to 7) is focused on pain management, edema control, and the immediate initiation of motion. We typically place the patient in a bulky, soft compressive dressing and initiate Continuous Passive Motion (CPM) within the first 24 hours. The CPM machine is utilized nearly continuously, pausing only for hygiene and active-assisted range of motion exercises. Adequate analgesia, often utilizing indwelling regional catheters, is essential to allow the patient to tolerate this early, aggressive mobilization.
Moving into the intermediate phase (Weeks 1 to 6), the focus shifts to maintaining the intraoperatively achieved arc of motion and combating the inevitable fibrotic healing response. Once the surgical wound is stable, we transition the patient to a static progressive splinting program. This involves the use of custom-molded, turnbuckle-style splints that alternate between pushing maximum extension and maximum flexion. Patients are instructed to wear the extension splint at night and the flexion splint during the day for defined intervals, interspersed with active physical therapy sessions. The goal is to provide a low-load, prolonged stretch to the healing tissues, which has been biomechanically proven to elongate collagen fibers effectively.
The late rehabilitation phase (Weeks 6 to 12 and beyond) concentrates on functional return, strengthening, and addressing any residual deficits. Active and active-assisted range of motion exercises continue, but we now introduce progressive resistance exercises for the biceps, triceps, and flexor-pronator mass. It is not uncommon for patients to experience a slight rebound in stiffness during the transition from CPM to splinting; this requires reassurance and strict adherence to the splinting protocol. Maximum medical improvement following a comprehensive open elbow release is typically not realized until 6 to 12 months postoperatively, underscoring the need for extensive preoperative patient counseling regarding the arduous nature of the recovery.
Pharmacologic adjuncts play a vital role throughout the rehabilitation timeline. As previously mentioned, heterotopic ossification prophylaxis with Indomethacin (typically 75mg sustained release daily) or Celecoxib is routinely prescribed for 3 to 6 weeks in high-risk individuals. Furthermore, we monitor closely for signs of complex regional pain syndrome (CRPS) or severe inflammatory flares, which may necessitate short courses of oral corticosteroids or specialized pain management interventions to keep the rehabilitation trajectory on track.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the medial over-the-top approach is deeply rooted in landmark orthopedic literature, which has continuously refined our understanding of elbow biomechanics and surgical efficacy. Foundational work by Morrey and colleagues at the Mayo Clinic established the critical parameters of the functional arc of motion and highlighted the severe disability associated with elbow contractures. Their early anatomical studies underscored the paramount importance of the anterior bundle of the MCL, dictating that any medial approach must prioritize its preservation to prevent catastrophic valgus instability.
Clinical outcome studies evaluating the medial over-the-top approach have consistently demonstrated excellent results in carefully selected patients. Mansat and Morrey published definitive series demonstrating that patients undergoing this comprehensive release achieve, on average, a 40 to 50-degree improvement in their total arc of motion. Furthermore, these studies validated the safety and efficacy of performing simultaneous ulnar nerve transposition, noting a high rate of resolution for preoperative neuropathic symptoms without compromising the overall motion gains. The literature firmly supports that addressing both the anterior and posterior compartments through a single medial window minimizes surgical trauma compared to combined medial and lateral incisions.
Comparative literature provides crucial guidelines on procedure selection. While arthroscopic elbow release has gained immense popularity for mild to moderate contractures—offering smaller incisions and potentially faster early rehabilitation—the open medial over-the-top approach remains the gold standard for severe, chronic stiffness, massive heterotopic ossification, and cases requiring complex ulnar nerve management. Kelly et al. demonstrated that for severe extrinsic contractures, the open approach provides a more reliable and complete excision of fibrotic tissue and osteophytes, leading to more durable long-term motion preservation.
In contemporary clinical practice, guidelines dictate a multidisciplinary approach to the stiff elbow. The decision to proceed with a medial over-the-top release should be made after a thorough review of 3D advanced imaging
