Femoral Neck Fracture Fixation: A Masterclass in Percutaneous Cannulated Screw Osteosynthesis
Key Takeaway
Step into the operating theater for a comprehensive masterclass on percutaneous cannulated screw fixation of femoral neck fractures. This guide covers detailed surgical anatomy, meticulous preoperative planning, and granular intraoperative execution, emphasizing precise guidewire and screw placement. Learn critical pearls, pitfalls, and postoperative care for optimal outcomes. Master the nuances of managing these challenging injuries with confidence.
Comprehensive Introduction and Patho-Epidemiology
Femoral neck fractures represent one of the most ubiquitous, yet persistently challenging, pathologies encountered in orthopedic traumatology. As orthopedic surgeons, we must approach these injuries not as routine cases, but as complex biomechanical and biological puzzles that demand a precise understanding of anatomy, meticulous surgical technique, and sound clinical judgment. The objective of this chapter is to provide an exhaustive masterclass in the principles and execution of closed reduction and percutaneous cannulated screw osteosynthesis for appropriate femoral neck fractures, ensuring we restore mechanical stability and optimize the biological environment for fracture union.
Epidemiologically, femoral neck fractures exhibit a classic bimodal distribution, presenting two distinct clinical entities that require highly tailored management strategies. The vast majority of these fractures occur in the geriatric population, specifically older, osteopenic or osteoporotic individuals. In this demographic, the injury is typically the sequela of low-energy trauma, such as a simple mechanical fall from a standing height. The pathogenesis here is intimately tied to the deterioration of bone microarchitecture, specifically the loss of primary compressive and tensile trabeculae within the proximal femur. The resulting fragility fracture is not merely an isolated orthopedic event, but often a sentinel indicator of declining overall health, carrying significant implications for one-year mortality and long-term morbidity.
Conversely, when femoral neck fractures occur in younger patients with normal, robust bone density, they are almost exclusively the result of high-energy trauma mechanisms. Motor vehicle collisions, falls from significant heights, and severe crush injuries generate the massive axial and shear forces required to fracture a healthy proximal femur. In these instances, the fracture is frequently associated with polytrauma, necessitating a multidisciplinary approach to patient resuscitation and stabilization. The degree of initial fracture displacement in both populations is the most critical prognostic factor influencing our treatment algorithms. Nondisplaced or valgus-impacted fractures often lend themselves favorably to percutaneous in situ fixation, whereas displaced fractures necessitate urgent anatomic reduction and stable fixation, or, in the physiologically older patient, arthroplasty.
The overarching goal of percutaneous cannulated screw fixation is the preservation of the native femoral head. This joint-preserving surgery is a delicate race against time, particularly in the young adult population, where the preservation of the native hip biomechanics is paramount to long-term functional outcomes. The natural history of untreated or inadequately stabilized femoral neck fractures is universally grim. Nondisplaced fractures, if left unfixed, possess a remarkably high propensity for secondary displacement due to the relentless torsional and shear forces exerted by normal hip musculature. For displaced fractures, the nonunion rate approaches absolute certainty without intervention, leading to profound limb shortening, debilitating pain, and catastrophic loss of ambulatory capacity.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the proximal femoral anatomy is the bedrock of successful osteosynthesis. When evaluating the osseous contours on standard anteroposterior (AP) and lateral radiographic projections, the normal femoral head and neck exhibit a characteristic, gentle S-curve. This smooth, symmetrical transition along the superior, inferior, anterior, and posterior cortical surfaces serves as our definitive radiographic benchmark for achieving an anatomical reduction. Any step-off, angulation, or disruption of this S-curve indicates an inadequate reduction that will inevitably subject the fixation construct to asymmetric, failure-inducing stresses.
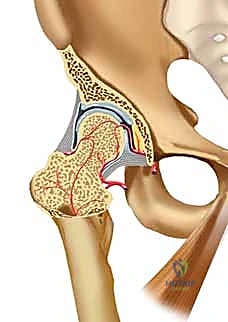
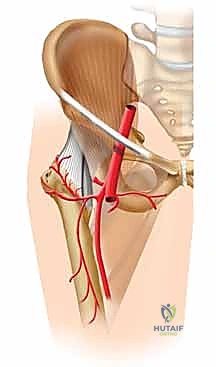
The vascular anatomy of the femoral neck is notoriously tenuous and represents the primary biological vulnerability in these injuries. The arterial supply to the mature femoral head is predominantly derived from the extracapsular arterial ring at the base of the femoral neck, which is primarily fed by the posterior branch of the medial femoral circumflex artery (MFCA). From this ring, the retinacular vessels of Weitbrecht ascend intracapsularly along the surface of the femoral neck to penetrate the articular cartilage margin, providing critical retrograde perfusion to the femoral head. A minor, highly variable contribution is provided by the foveal artery (artery of the ligamentum teres), originating from the obturator artery, though this is rarely sufficient to sustain the femoral head in isolation.


Fracture displacement directly jeopardizes this delicate vascular network through direct tearing, stretching, or kinking of the retinacular vessels. Furthermore, the intra-articular nature of the femoral neck means that bleeding from the fracture site results in a tense hemarthrosis within the unyielding hip capsule. This leads to a tamponade effect, further compromising venous outflow and arterial inflow. This profound vascular insult is the primary driver of avascular necrosis (AVN), a devastating complication that occurs in a significant percentage of displaced fractures. Additionally, the synovial fluid environment contains fibrinolysins that actively degrade the fracture hematoma, depriving the fracture site of the crucial initial scaffolding required for primary bone healing.
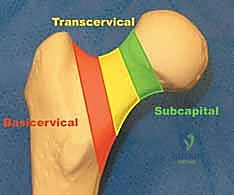
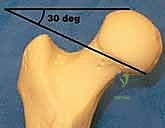
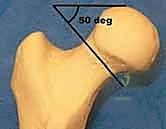
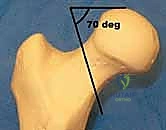
Biomechanically, we classify these fractures based on their anatomic location—subcapital, transcervical, or basicervical—and their orientation. The Pauwels classification remains biomechanically highly relevant for transcervical fractures, categorizing them by the angle of the fracture line relative to the horizontal axis. Pauwels Type 1 fractures (<30 degrees) experience primarily compressive forces, making them inherently more stable. Pauwels Type 2 (30-50 degrees) experience mixed forces. Pauwels Type 3 fractures (>50 degrees) are highly vertical and subject to massive shear forces, predisposing them to varus collapse and nonunion. High-angle fractures demand specific fixation strategies, often requiring at least one screw placed perpendicular to the fracture plane, or the utilization of a sliding hip screw construct to neutralize shear and promote controlled axial compression.
Exhaustive Indications and Contraindications
Patient presentation is typically characterized by a distinct traumatic event followed by an immediate inability to bear weight. Physical examination of a displaced fracture classically reveals a shortened, externally rotated lower extremity, with excruciating pain provoked by any attempted range of motion. However, in cases of nondisplaced or valgus-impacted fractures, the physical deformity may be entirely absent, and the patient may even present with a deceptively benign examination, complaining only of vague groin or thigh pain. This highlights the absolute necessity of rigorous radiographic evaluation.

The standard diagnostic imaging protocol mandates an AP view of the pelvis, alongside dedicated AP and cross-table lateral views of the affected hip. An AP traction radiograph with internal rotation is an invaluable adjunct, as it frequently elucidates the true fracture pattern, unmasks subtle comminution, and provides a preview of the fracture's reducibility. In instances where clinical suspicion remains high (e.g., elderly patient, groin pain, inability to ambulate) despite ostensibly negative plain radiographs, Magnetic Resonance Imaging (MRI) serves as the gold standard. MRI is highly sensitive and specific, capable of detecting occult trabecular microfractures and bone marrow edema within hours of the injury.

The indications for percutaneous cannulated screw fixation are highly specific. The ideal candidates are patients with nondisplaced (Garden I and II) femoral neck fractures, regardless of age, and physiologically young patients with displaced fractures where native joint preservation is an absolute priority. Valgus-impacted fractures are also classically treated with in situ fixation to prevent secondary displacement. The goal is to provide rigid, stable fixation that allows for early mobilization while minimizing the surgical footprint and preserving the residual blood supply to the femoral head.
| Clinical Scenario | Indication Status for Percutaneous Fixation | Rationale / Alternative |
|---|---|---|
| Young Patient (<60 yrs), Displaced | Strong Indication (Urgent) | Joint preservation is paramount. Requires perfect closed or open reduction prior to fixation. |
| Any Age, Nondisplaced/Valgus Impacted | Strong Indication | High risk of secondary displacement if untreated. In situ fixation yields excellent outcomes. |
| Elderly Patient (>70 yrs), Displaced | Contraindicated | High rates of AVN and nonunion. Arthroplasty (Hemi or THA) allows immediate weight-bearing and definitive treatment. |
| Basicervical Fracture Pattern | Relative Contraindication | Biomechanically unstable for screws alone. Better treated with a Sliding Hip Screw (SHS) or Cephalomedullary Nail. |
| Severe Pre-existing Hip Osteoarthritis | Contraindication | Fixation will not resolve arthritic pain. Total Hip Arthroplasty (THA) is the definitive treatment. |
Nonoperative management is severely restricted to a highly select cohort of patients. This includes individuals who are entirely non-ambulatory at baseline, those with profound neurological impairment precluding rehabilitation, or patients who are moribund and in extremis, where the physiologic insult of anesthesia and surgery would be immediately fatal. In these tragic scenarios, the treatment paradigm shifts entirely to palliative comfort care, stringent pain management, and rigorous nursing protocols to prevent decubitus ulcers, pulmonary complications, and deep vein thrombosis.
Pre-Operative Planning, Templating, and Patient Positioning
The success of a percutaneous femoral neck fixation is largely dictated before the surgical incision is ever made. Meticulous preoperative planning begins with the medical optimization of the patient. In the geriatric population, these fractures are often complicated by a myriad of medical comorbidities, including dehydration, electrolyte derangements, undiagnosed cardiac ischemia, and coagulopathies. While rapid surgical intervention is desired to minimize the complications of recumbency, a brief window of 24 to 48 hours is generally acceptable, and often necessary, to correct reversible medical derangements and optimize the patient for anesthesia.

Radiographic templating is an indispensable step. High-quality digital radiographs of the contralateral, uninjured hip are utilized to template the native femoral neck-shaft angle, estimate the required screw lengths, and determine the optimal thread length. Standard cannulated screws are typically 6.5mm, 7.0mm, or 7.3mm in diameter. Selecting the appropriate thread length (usually 16mm or 32mm) is critical; the threads must entirely bypass the fracture line and purchase exclusively in the dense subchondral bone of the femoral head. If threads span the fracture site, the screw will act as a lag strut, actively preventing the interfragmentary compression necessary for primary bone healing.
Patient positioning is arguably the most technically demanding aspect of the initial setup. The procedure is overwhelmingly performed on a specialized orthopedic fracture table, which allows for precise, controlled application of traction and rotational forces while maintaining unobstructed fluoroscopic access. The patient is placed supine, and both lower extremities are secured in traction boots. The perineal post must be meticulously padded to prevent devastating pudendal nerve palsies or soft tissue necrosis. The contralateral limb is typically placed in a hemilithotomy position or extended down and away (scissor configuration) to allow the C-arm to swing freely for the lateral projection.

Fluoroscopic setup must be perfected prior to prepping and draping. The C-arm is brought in from the contralateral side. The surgeon must verify that a perfect, orthogonal AP view and a true, unobstructed lateral view of the femoral neck and head can be obtained effortlessly. The lateral view is often achieved by rolling the C-arm over the top of the patient. Any parallax or malrotation in the fluoroscopic imaging will invariably lead to misguided wire trajectories and suboptimal hardware placement. Time spent perfecting the imaging setup pays exponential dividends during the execution of the surgery.
Step-by-Step Surgical Approach and Fixation Technique
If the fracture is displaced, achieving an anatomical closed reduction is the absolute prerequisite for proceeding with percutaneous fixation. The classic reduction maneuvers, such as the Leadbetter or Whitman techniques, involve a sequence of controlled forces. Typically, the limb is slightly flexed and adducted to disengage the fracture fragments. Longitudinal traction is then applied to restore length, followed by smooth, controlled internal rotation to correct the retroversion deformity. Finally, the limb is brought into slight abduction to lock the fracture into the cortical contours of the femoral neck. The reduction must be critically evaluated on both AP and lateral fluoroscopic views. If an anatomical or slightly valgus reduction cannot be achieved closed, the surgeon must immediately pivot to an open reduction via a Watson-Jones or Smith-Petersen approach.


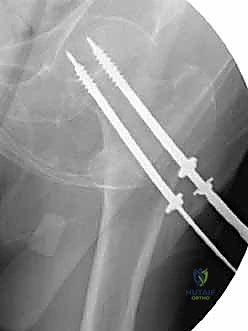
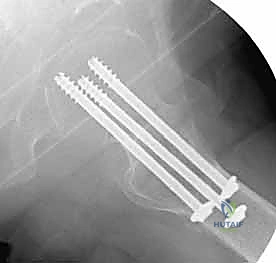
Once reduction is confirmed, the percutaneous approach begins. A strictly lateral incision, approximately 3 to 5 centimeters in length, is made over the proximal lateral thigh, corresponding to the level of the lesser trochanter. The fascia lata is incised, and the vastus lateralis is either split longitudinally or elevated anteriorly off the lateral intermuscular septum to expose the lateral femoral cortex. The classic, most biomechanically stable construct for a standard transcervical fracture is three parallel cannulated screws configured in an inverted triangle.



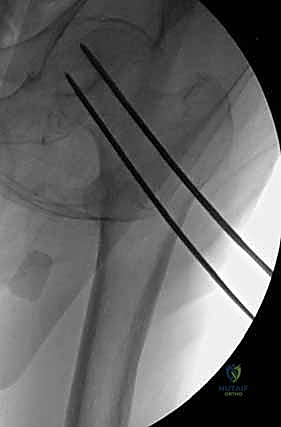
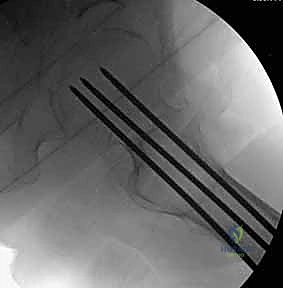
The placement of the first guide wire is the most critical step of the operation. This inferior (calcar) wire dictates the trajectory of the entire construct. The starting point on the lateral cortex must be at or slightly above the level of the lesser trochanter. Starting distal to the lesser trochanter creates a massive stress riser in the subtrochanteric region, significantly increasing the risk of an iatrogenic subtrochanteric femur fracture. The inferior wire is advanced under fluoroscopic guidance, hugging the dense cortical bone of the inferior femoral neck (calcar femorale) on the AP view, and centered in the neck on the lateral view. It is advanced until the tip sits precisely in the subchondral bone of the inferior femoral head.


Following the perfect placement of the inferior wire, the posterior-superior and anterior-superior wires are placed. The posterior wire is particularly dangerous; the surgeon must ensure it does not breach the posterior cortex of the femoral neck, which could tether or lacerate the critical retinacular vessels. Strict parallelism of the three guide wires is essential to allow the screws to act as a unified sliding construct, permitting controlled dynamic compression at the fracture site during weight-bearing.

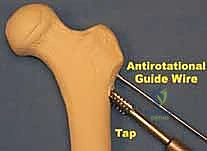
Once all three guide wires are confirmed to be parallel and appropriately positioned in the subchondral bone, the outer cortex is over-drilled. In dense, young bone, tapping may be necessary to prevent the screw from binding and inadvertently distracting the fracture. The appropriate length screws are selected (subtracting 5mm from the measured length to prevent joint penetration). Washers are strongly recommended in osteopenic bone to prevent the screw heads from burying into the lateral cortex. The screws are advanced sequentially. Crucially, before final tightening, the traction on the fracture table must be released. This allows the screws to actively compress the fracture site rather than simply holding it in distraction. Final fluoroscopic images are obtained in multiple planes to confirm fracture compression, hardware position, and the absolute absence of intra-articular screw penetration.

Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, femoral neck fractures are plagued by a high complication rate, primarily driven by the precarious local biology and challenging biomechanics. The most feared complication is avascular necrosis (AVN) of the femoral head. The incidence of AVN is directly correlated with the degree of initial fracture displacement and, to a lesser extent, the time to surgical reduction. Rates range from 5-10% in nondisplaced fractures to upwards of 30-40% in severely displaced fractures. AVN typically presents insidiously with progressive groin pain months to years after the index surgery. Diagnosis is confirmed via MRI, which will show characteristic serpiginous changes in the femoral head. Management of post-traumatic AVN depends on the extent of head collapse; pre-collapse stages may be managed with core decompression or vascularized fibular grafting in young patients, while post-collapse inevitably requires conversion to a Total Hip Arthroplasty (THA).

Nonunion is another frequent and devastating complication, occurring in up to 30% of displaced fractures treated with internal fixation. Nonunion is mechanically driven by excessive shear forces (
Clinical & Radiographic Imaging Archive




