Extensor Tendon Centralization: A Masterclass in Sagittal Band Repair & Reconstruction

Key Takeaway
Join us in the OR for an in-depth masterclass on extensor tendon centralization. We'll meticulously cover the anatomy of the MCP joint, crucial preoperative planning, and detailed surgical execution for both direct sagittal band repair and advanced reconstruction techniques. Learn to identify and manage traumatic "boxer's knuckle" injuries, ensuring optimal patient outcomes and avoiding common pitfalls.
Comprehensive Introduction and Patho-Epidemiology
Traumatic extensor tendon subluxation at the metacarpophalangeal (MCP) joint, colloquially recognized in orthopedic circles as "boxer’s knuckle," represents a fascinating, intricate, and often debilitating disruption of the digital extensor mechanism. Unlike the atraumatic, progressive subluxation frequently observed in the rheumatoid hand—which stems from chronic synovial distension, capsular attenuation, and progressive ulnar drift—traumatic sagittal band rupture is an acute biomechanical failure. This pathology demands a precise understanding of the delicate balance between dynamic tendon excursion and static ligamentous restraint. When the sagittal band fails, the extensor digitorum communis (EDC) tendon loses its centralized fulcrum, leading to altered kinematics, profound weakness in active extension, and a painful, mechanical snapping over the metacarpal condyle.
To properly categorize and manage these injuries, we rely on the foundational classification system proposed by Rayan and Murray. Type I injuries encompass a contusion or sprain of the sagittal band without frank macroscopic tearing or tendon instability; these are often managed symptomatically. Type II injuries denote a structural failure resulting in tendon subluxation, wherein the extensor tendon laterally displaces beyond the midline of the metacarpal head but critically maintains contact with the condyle during full MCP joint flexion. Type III injuries represent the most severe end of the spectrum: a complete dislocation where the EDC tendon is entirely displaced into the intermetacarpal groove, losing all articular contact with the condyle. Distinguishing between a Type II subluxation and a Type III dislocation is not merely an academic exercise; it dictates the aggressiveness of our nonoperative protocols and the threshold for surgical intervention.
Epidemiologically, traumatic sagittal band ruptures exhibit a strong predilection for the long finger, followed by the ring finger. The radial sagittal band is overwhelmingly the most frequently injured structure, leading to ulnar subluxation of the extensor tendon. This asymmetry is not coincidental; anatomical studies have demonstrated that the radial sagittal band is inherently thinner and longer than its stout ulnar counterpart, rendering it biomechanically susceptible to shear forces. Furthermore, the natural ulnar deviation of the digits during power grip places disproportionate tensile stress on the radial restraints. While ulnar-sided sagittal band injuries leading to radial subluxation are documented, they are exceedingly rare and typically associated with atypical trauma or forced hyper-radial deviation.
The pathogenesis of this injury is intimately tied to the position of the hand at the moment of impact. The classic mechanism involves a direct, blunt force applied to a clenched fist—hence the "boxer's knuckle" moniker. When the MCP joint is in maximum flexion, the sagittal bands are under their greatest physiologic tension, tightly tethering the EDC tendon to the metacarpal neck. A direct blow to the dorsal MCP joint in this position forces the tendon against the taut sagittal band, leading to a sheer failure. Alternatively, indirect mechanisms involving forceful, resisted flexion combined with sudden ulnar deviation can generate sufficient tensile overload to rupture the radial sagittal band. In cases of penetrating trauma, such as human bite wounds or lacerations, the sagittal band is directly violated, often concomitantly with the joint capsule, necessitating a vastly different, infection-conscious treatment paradigm.
Detailed Surgical Anatomy and Biomechanics
Mastery of the extensor mechanism at the MCP joint is the absolute prerequisite for successful surgical reconstruction. This region is not a simple tendon-to-bone insertion; it is a highly sophisticated, dynamic fibro-osseous and retinacular complex designed to synchronize motion across multiple joints. The primary longitudinal actor is the Extensor Digitorum Communis (EDC) tendon, which, along with the Extensor Indicis Proprius (EIP) and Extensor Digiti Minimi (EDM), provides the primary extensor moment to the digits. However, without the intricate retinacular system to constrain and guide them, these tendons would inevitably bowstring during wrist extension or slip into the intermetacarpal valleys during digital flexion.
The crucial stabilizing elements at the MCP level are the sagittal bands. Often referred to as the "shroud ligaments," these structures form a circumferential sling around the extensor tendon. Originating from the volar plate and the deep transverse metacarpal ligament, the sagittal bands course dorsally to envelop the EDC tendon. They are composed of two distinct layers: a superficial layer that passes over the dorsal aspect of the tendon, and a deep layer that passes volarly, effectively creating a tunnel. The primary biomechanical function of the sagittal bands is twofold: they prevent bowstringing of the extensor tendon during MCP hyperextension, and they strictly centralize the tendon over the metacarpal head during the full arc of flexion.
Beyond the sagittal bands, the broader extensor retinacular system plays a synergistic role. The juncturae tendinum are oblique intertendinous connections located proximal to the MCP joints. They serve to distribute extensor forces across the digits and can occasionally mask a proximal EDC laceration by transmitting force from an adjacent intact tendon. Distally, the intrinsic mechanism integrates with the extrinsic system. The lumbrical muscles, originating from the flexor digitorum profundus tendons, course along the radial aspect of the digits volar to the deep transverse metacarpal ligament. They insert into the radial lateral band of the extensor expansion, facilitating simultaneous MCP flexion and interphalangeal (IP) extension. During dissection, the lumbrical tendon must be carefully identified and protected, as iatrogenic injury will severely compromise intrinsic digital balance.
From a neurovascular perspective, the dorsal approach to the MCP joint is fraught with potential hazards. The dorsal sensory branches of the radial nerve and the dorsal branch of the ulnar nerve arborize extensively in the subcutaneous tissues overlying the metacarpals. These delicate nerves are highly susceptible to traction injury or inadvertent transection during the initial skin incision and superficial dissection. Iatrogenic neuroma formation in this region is a catastrophic complication that can render a technically perfect tendon reconstruction clinically disastrous due to intractable pain. Therefore, meticulous, blunt subcutaneous dissection and the use of gentle, broad-based retraction are mandatory to preserve these vital sensory conduits.
Exhaustive Indications and Contraindications
The decision-making algorithm for surgical intervention in sagittal band ruptures requires a nuanced synthesis of the patient's chronicity, functional demands, injury severity, and soft tissue integrity. While conservative management remains the gold standard for many acute, closed injuries, specific clinical scenarios unequivocally demand operative centralization and repair to restore hand kinematics.
Indications for Surgical Intervention
Acute surgical intervention (within 3 weeks of injury) is primarily indicated for open injuries, particularly those involving human or animal bites, where formal joint exploration, meticulous debridement, and copious irrigation are paramount to prevent devastating septic arthritis. Furthermore, professional athletes or high-demand manual laborers who cannot tolerate the prolonged immobilization required for conservative management may be candidates for acute primary repair to expedite their return to play or work. Type III dislocations—where the tendon is irreducibly trapped in the intermetacarpal groove—frequently fail closed management and require surgical relocation and repair.
Chronic injuries (presenting >3-4 weeks post-injury) represent the most common indication for surgery. In these cases, the torn sagittal band has retracted, scarred, and attenuated, rendering nonoperative splinting futile. Patients presenting with chronic, painful snapping, persistent extensor lag, and ulnar deviation deformity require formal surgical reconstruction. Additionally, any patient who has undergone a compliant trial of conservative splinting but continues to experience symptomatic subluxation or functional deficit is an absolute candidate for operative centralization.
Contraindications to Surgery
Contraindications must be strictly respected to avoid compounding the patient's morbidity. Active localized or systemic infection (excluding the immediate management of an open bite wound) is an absolute contraindication to elective tendon reconstruction. A severely compromised dorsal soft tissue envelope—whether from profound crush injury, severe burns, or previous multiple surgeries—precludes immediate reconstruction until soft tissue coverage (e.g., via flap transfer) is secured. Severe, end-stage osteoarthritis or inflammatory arthropathy of the involved MCP joint is a relative contraindication; in such cases, soft tissue reconstruction alone will fail to address the underlying articular pathology, and arthroplasty or arthrodesis combined with extensor centralization may be more appropriate. Finally, a non-compliant patient who is unable or unwilling to adhere to the rigorous, multi-week postoperative rehabilitation protocol will inevitably suffer from repair rupture or profound stiffness, contraindicating the procedure.
| Category | Specific Clinical Scenario | Rationale / Management Impact |
|---|---|---|
| Indications (Acute) | Open joint injury / Bite wound | Requires immediate I&D, prevents septic arthritis; repair done concurrently if clean. |
| Indications (Acute) | High-demand professional athlete | Expedites rigid stabilization; allows for early relative motion protocols. |
| Indications (Acute) | Irreducible Type III Dislocation | Tendon trapped in intermetacarpal groove; mechanical block to extension requires open reduction. |
| Indications (Chronic) | Failed conservative management | Persistent snapping/pain after 4-6 weeks of strict splinting necessitates structural repair. |
| Indications (Chronic) | Chronic painful subluxation (>4 weeks) | Attenuated tissues will not heal with immobilization; requires formal reconstruction (e.g., tendon slip). |
| Contraindications | Active overlying infection / Cellulitis | High risk of deep space infection and hardware/suture seeding; requires resolution prior to surgery. |
| Contraindications | Poor soft tissue envelope (Crush/Burn) | High risk of wound dehiscence and tendon exposure; requires plastic surgery optimization first. |
| Contraindications | End-stage MCP Osteoarthritis | Soft tissue repair alone will not relieve pain; requires concurrent arthroplasty or fusion. |
| Contraindications | Demonstrated severe non-compliance | Post-op rehab is critical; failure to comply leads to rupture or frozen joint. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative evaluation is the cornerstone of a successful surgical outcome. The clinical examination must be exhaustive. Visually, the surgeon should assess for localized edema, ecchymosis, and resting digital posture. A characteristic ulnar deviation of the affected digit at rest is highly suggestive of a radial sagittal band rupture.


Palpation is critical; exquisite tenderness localized directly over the dorsal-radial aspect of the metacarpal head points to the sagittal band, whereas deeper pain in the intermetacarpal space might suggest a collateral ligament injury. The hallmark of the physical exam is the dynamic assessment of tendon instability. Ask the patient to actively flex the MCP joint while making a fist. In a positive test, the extensor tendon will visibly and palpably snap off the metacarpal condyle into the ulnar gutter. Upon active extension, the tendon may snap back into a centralized position, or, in severe cases, the patient may exhibit an extension lag, requiring passive assistance to bring the tendon back over the apex of the joint.
Imaging modalities serve to confirm the clinical diagnosis and rule out concomitant pathology. Standard posteroanterior, lateral, and oblique radiographs of the hand are mandatory. While the sagittal bands are radiolucent, X-rays are crucial for excluding metacarpal head fractures, collateral ligament avulsion fractures, or underlying degenerative joint disease that could compromise the surgical outcome. If the clinical picture is obscured by massive swelling or patient guarding, dynamic ultrasonography is an excellent, cost-effective tool. It allows for real-time visualization of the tendon subluxating during passive and active flexion. For more complex or chronic cases, Magnetic Resonance Imaging (MRI) without contrast is the gold standard. High-resolution axial T1 and T2-weighted sequences will definitively demonstrate focal discontinuity, thickening, or complete absence of the sagittal band, alongside the eccentrically positioned extensor tendon.
Preoperative preparation and positioning must be standardized. The procedure is typically performed on an outpatient basis under regional anesthesia (e.g., axillary or supraclavicular brachial plexus block) or local anesthesia with intravenous sedation (WALANT - Wide Awake Local Anesthesia No Tourniquet is increasingly popular as it allows for intraoperative active motion testing). If a block is used, the patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm, typically inflated to 250 mmHg after exsanguination with an Esmarch bandage, to ensure a bloodless surgical field. Loupe magnification (minimum 2.5x to 3.5x) is absolutely essential for the meticulous identification of the attenuated retinacular structures and the protection of the delicate dorsal sensory nerves.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution for extensor tendon centralization demands precision, respect for the soft tissue envelope, and a deep understanding of dynamic tendon tracking. The choice between direct primary repair and complex reconstruction hinges entirely on the chronicity of the injury and the intraoperative assessment of tissue viability.
The Surgical Approach and Dissection
The procedure begins with a dorsal longitudinal or slightly curvilinear incision centered over the affected MCP joint, extending approximately 2 cm proximal and 2 cm distal to the joint line. A curvilinear incision is often preferred to prevent a linear scar contracture directly over the joint apex.

Upon incising the dermis, meticulous blunt dissection is utilized to spread the subcutaneous fat. The immediate priority is the identification and mobilization of the dorsal sensory nerve branches. These must be gently retracted with vessel loops; rigorous retraction can lead to neuropraxia.
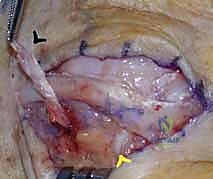
Once the extensor mechanism is exposed, the paratenon is carefully incised longitudinally. The surgeon must now dynamically assess the joint. By passively flexing and extending the MCP joint, the exact pathology becomes evident. In a classic radial sagittal band rupture, the EDC tendon will forcefully subluxate ulnarly into the intermetacarpal groove as the joint moves into flexion. The radial sagittal band will appear either acutely avulsed from the volar plate/extensor hood or chronically attenuated and scarred.


Acute Primary Repair Technique
If the injury is acute (typically less than 3 weeks old), the edges of the ruptured sagittal band are usually identifiable and possess sufficient integrity for direct repair. The subluxated extensor tendon is manually centralized over the metacarpal head.
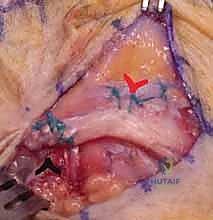
The torn edges of the radial sagittal band are approximated. Using a non-absorbable braided suture (such as 4-0 or 5-0 Ethibond or FiberWire), a horizontal mattress or figure-of-eight suture configuration is employed to reapproximate the tissue.

If the sagittal band has avulsed directly off the base of the proximal phalanx or the volar plate, suture anchors (typically 1.5mm or 2.0mm) loaded with non-absorbable suture may be placed into the bone to provide a robust anatomic reattachment.
Following the repair, the MCP joint is passively cycled through a full range of motion to ensure the tendon tracks centrally without overriding tension that could restrict flexion.

Chronic Reconstruction Techniques
In chronic settings, the sagittal band tissue is often contracted, friable, or completely resorbed, rendering primary repair impossible. Here, a reconstructive sling must be fabricated. Several masterclass techniques exist, primarily utilizing local tendon slips.
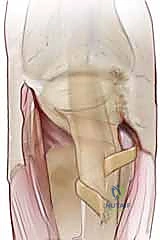
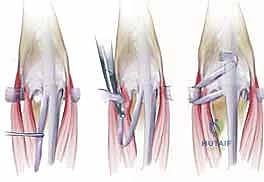
The Tendon Slip Transfer (Carroll or Wheeldon Technique): This is the workhorse for chronic reconstructions. A distally based, partial-width slip of the EDC tendon (approximately one-third of its width) is harvested from the ulnar side of the affected tendon.

This slip is left attached distally at the level of the MCP joint. The free proximal end is then passed volarly, looping around the radial collateral ligament or through the deep transverse metacarpal ligament.

It is then brought back dorsally and sutured onto itself or the main body of the EDC tendon under appropriate tension while the tendon is held in a centralized position. This effectively creates a new, robust radial checkrein.

Junctura Tendinum Transfer: If the adjacent junctura tendinum is robust, it can be detached from its adjacent tendon, mobilized, and sutured tightly to the radial aspect of the subluxating EDC tendon, pulling it radially and centralizing it.
Extensor Indicis Proprius (EIP) Transfer: For severe, recurrent cases or massive tissue loss, the EIP tendon can be harvested, routed radially around the base of the proximal phalanx, and woven into the EDC to provide a powerful, dynamic centralization force.

Regardless of the reconstructive method chosen, meticulous hemostasis is achieved after tourniquet deflation. The skin is closed with interrupted non-absorbable sutures (e.g., 5-0 nylon). A bulky, sterile compressive dressing is applied, incorporating a volar resting splint to protect the repair immediately postoperatively.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, extensor tendon centralization procedures carry a distinct profile of potential complications. The delicate balance between achieving sufficient tension to prevent recurrent subluxation and allowing sufficient excursion to permit full flexion is the central challenge of this surgery.
The most frequent complication encountered is a loss of terminal active MCP joint flexion, often coupled with an extensor lag. This stiffness arises from over-tensioning of the reconstructed sagittal band sling, postoperative adhesions between the extensor mechanism and the underlying periosteum, or prolonged immobilization. Extensor lags of 10 to 15 degrees are relatively common but are usually functionally well-tolerated by the patient. However, severe stiffness that impedes power grip requires aggressive intervention. Initial management is always nonoperative, relying on intensive hand therapy, dynamic flexion splinting, and scar massage. If stiffness persists beyond 6 months and functionally limits the patient, a surgical tenolysis and capsulotomy may be indicated as a salvage procedure.
Recurrent subluxation is a catastrophic failure of the repair or reconstruction. This typically occurs due to inadequate initial tissue tensioning, failure of the suture material, or patient non-compliance with the postoperative splinting protocol (e.g., forceful early fist-making).
When recurrent instability occurs, conservative management is futile. The patient must be counseled on the need for revision surgery. Revision cases are technically demanding due to the altered anatomy and dense scar tissue. In these salvage scenarios, local tissue transfers are often inadequate, and the surgeon must resort to more robust techniques, such as a free tendon graft (e.g., palmaris longus) routed through a drill hole in the proximal phalanx to reconstruct the sagittal band, or an EIP transfer.

Infection and wound dehiscence are rare but devastating complications, particularly given the superficial nature of the extensor tendons. Superficial infections can often be managed with oral antibiotics and local wound care. Deep space infections, however, threaten the integrity of the tendon repair and the joint cartilage, necessitating emergent operative irrigation and debridement, often resulting in the failure of the centralization. Iatrogenic nerve injury to the dorsal sensory branches results in painful neuromas, which can be far more debilitating than the original tendon instability. Prevention through careful dissection is paramount; if a neuroma forms, salvage may require neuroma excision and burying the proximal nerve stump into deep muscle or bone.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Extensor Lag / Stiffness | 15% - 25% | Over-tensioning, prolonged immobilization, dense adhesions. | Aggressive hand therapy, dynamic splinting; late surgical tenolysis if refractory. |
| Recurrent Subluxation | 5% - 10% | Under-tensioning, suture |
Clinical & Radiographic Imaging Archive

