

Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are tackling a common yet often technically demanding injury: traumatic disruption of the extensor mechanism. These injuries, due to the superficial and exposed location of the dorsal tendons, frequently present with concomitant damage to bone, skin, and joint structures. The dorsal integument of the hand is remarkably thin and lacks the protective subcutaneous fat padding found on the volar surface, rendering the extensor tendons highly vulnerable to lacerations, crush injuries, and abrasions from industrial accidents, domestic mishaps, and altercations. Our ultimate goal is to achieve a meticulous, biomechanically sound repair, restoring fluid function and preventing long-term disability.
Remember, early and appropriate treatment of acute injuries is paramount. The reconstruction of subacute and chronic cases is significantly more challenging and less effective due to tendon retraction, muscle contracture, and the rapid formation of dense, unyielding adhesions. The extensor mechanism is not merely a set of ropes pulling on levers; it is an intricate, finely balanced aponeurotic sheet that relies on precisely coordinated tension between extrinsic and intrinsic forces. A failure to respect this delicate balance during repair will inevitably result in a functionally compromised digit, manifesting as either an extensor lag or a severe loss of flexion.
Epidemiologically, extensor tendon injuries outnumber flexor tendon injuries, yet they have historically received less academic focus, often resulting in suboptimal outcomes when managed by inexperienced practitioners. The belief that extensor repairs are "easier" than flexor repairs is a dangerous fallacy. While the surgical access may be more straightforward, the thin, flat morphology of the extensor tendons—particularly distal to the metacarpophalangeal (MCP) joint—makes them notoriously difficult to suture securely. Furthermore, their intimate association with the underlying periosteum and joint capsules predisposes them to severe stiffness if rehabilitation is not perfectly executed.
As orthopedic surgeons, we must approach these injuries with the same reverence and technical precision as we do a Zone II flexor tendon repair. This masterclass will provide you with an exhaustive, step-by-step guide to navigating the dorsal landscape, executing robust repairs, and managing the complex postoperative rehabilitation required to achieve excellent clinical outcomes. We will cover the spectrum of injuries from the distal interphalangeal joint to the proximal forearm, equipping you with the knowledge to handle any extensor trauma that presents in the emergency department or trauma bay.
Detailed Surgical Anatomy and Biomechanics
Before we make any incision, a profound, three-dimensional understanding of the extensor anatomy is non-negotiable. The extensor mechanism is a complex, finely tuned system, and even minor disruptions or slight alterations in tendon length can have profound functional consequences. The anatomy dictates our surgical approach, our suture selection, and our rehabilitation protocols.
Extensor Tendon Zones of Injury
Let us first orient ourselves with the Verdan zones, our universal roadmap for classifying these injuries. The hand and forearm are divided into distinct zones based on the anatomical and biomechanical properties of the extensor mechanism in those regions.
For the fingers, the zones are divided into eight regions, numbered from distal to proximal. Zone I overlies the distal interphalangeal (DIP) joint. Injury here typically involves the terminal extensor tendon, leading to the classic mallet finger deformity. The terminal tendon is remarkably thin in the fingers, measuring scarcely a millimeter in thickness, making primary suture repair technically demanding and often necessitating dermatotenodesis techniques. Zone II overlies the middle phalanx, where lacerations can sometimes mimic Zone I injuries clinically. Here, we must be exquisitely mindful of the converging lateral bands and their critical contribution to distal extension. Injury to the periosteum of the middle phalanx in this zone can lead to severe tendon adherence and loss of DIP flexion.

Zone III overlies the proximal interphalangeal (PIP) joint. This is the exclusive territory of the central slip. Disruption here leads to a boutonnière deformity, particularly if untreated, as the lateral bands migrate palmarly past the axis of rotation and paradoxically become PIP flexors. Zone IV spans the proximal phalanx. Injuries here often involve only a portion of the extensor mechanism, as the extensor hood covers a significant circumference of the digit. Zone V encompasses the metacarpophalangeal (MCP) joint. Injuries here can be open lacerations (often from human bites or "fight bites") or closed sagittal band ruptures, leading to extensor tendon subluxation. Always assume an open joint injury with any tendon laceration around the MCP joint until proven otherwise.
Zone VI covers the dorsum of the hand. Here, the juncturae tendinum provide interconnections between the Extensor Digitorum Communis (EDC) tendons. These bands can effectively mask complete lacerations if the injury is proximal to them, making clinical identification challenging. Zone VII involves the wrist and the extensor retinaculum, housing the six distinct extensor compartments. Finally, Zone VIII is located in the forearm, at the musculotendinous junction or muscle belly. Detecting concurrent posterior interosseous nerve (PIN) injury is critical and notoriously difficult in this zone. The thumb is divided into five zones, also distal to proximal, with the terminal extensor tendon of the thumb being notably thicker than in other digits.
Extrinsic Extensor Tendons and Compartments
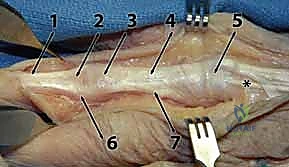
The extrinsic extensors originate from the lateral epicondyle and the dorsal aspects of the radius and ulna. Their musculotendinous junctions are typically located 3 to 4 centimeters proximal to the wrist joint. The fascia over these tendons thickens dramatically at the radiocarpal joint to form the extensor retinaculum, which prevents bowstringing during wrist extension and creates six distinct fibro-osseous compartments.

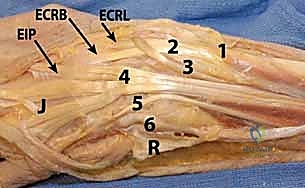
Compartment 1 houses the Abductor Pollicis Longus (APL) and Extensor Pollicis Brevis (EPB), often separated by a distinct septum which is clinically relevant in De Quervain's tenosynovitis. Compartment 2 contains the Extensor Carpi Radialis Longus (ECRL) and Extensor Carpi Radialis Brevis (ECRB), the primary wrist extensors. Compartment 3 contains the Extensor Pollicis Longus (EPL), which uniquely hooks around Lister's tubercle, utilizing it as a fulcrum to change its line of pull. Lacerations of the EPL proximal to the MCP joint are associated with massive proximal retraction, often pulling entirely into the forearm.
Compartment 4 is the most voluminous, containing the four Extensor Digitorum Communis (EDC) tendons and the Extensor Indicis Proprius (EIP). The EIP lies deep and slightly ulnar to the EDC of the index finger. Compartment 5 contains the Extensor Digiti Minimi (EDM), the independent extensor for the small finger, which often consists of two distinct tendon slips. Compartment 6 houses the Extensor Carpi Ulnaris (ECU), which runs in a distinct subsheath and is critical for wrist extension and ulnar deviation, as well as providing dynamic stability to the distal radioulnar joint.
Intrinsic Extensor Tendons and Neurovascular Structures
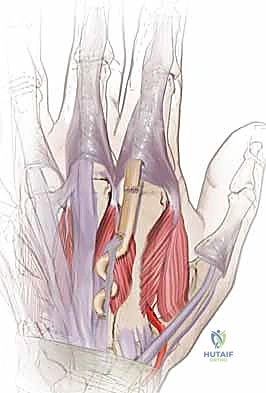
The intrinsic extensor system originates entirely within the hand and includes the four dorsal interossei, three palmar interossei, and four lumbricals. These muscles are essential for the complex, fine motor movements of the digits. The intrinsic tendons join to form the conjoined lateral bands volar to the axis of the MCP joint, acting as primary MCP flexors.
As these bands travel distally, they migrate dorsal to the axis of rotation of the PIP and DIP joints. This unique, highly specialized anatomical arrangement allows them to simultaneously flex the MCP joint and extend the interphalangeal joints. The intrinsic system interweaves with the extrinsic system via the extensor hood, a complex aponeurotic expansion that coordinates the pull of both systems. Disruption of this balance, such as in intrinsic tightness or intrinsic minus (claw) deformities, highlights the critical nature of this interplay.
Neurovascularly, the dorsal cutaneous nerves are superficial and highly vulnerable during surgical dissection. The radial sensory nerve branches supply the radial dorsum of the hand, while the dorsal branch of the ulnar nerve supplies the ulnar aspect. These nerves are frequently encountered immediately subdermally. Meticulous, sharp dissection and careful, atraumatic retraction are absolutely essential to prevent iatrogenic neuromas, which can be far more debilitating than the original tendon injury. The dorsal venous system is also extensive; while sacrificing a single vein is generally well-tolerated, mass ligation can lead to significant postoperative dorsal edema, complicating rehabilitation and wound healing.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for an extensor tendon injury relies on a careful assessment of the injury zone, the degree of tendon disruption, the presence of concomitant injuries, and the chronicity of the lesion. While many flexor tendon injuries mandate immediate surgical repair, the extensor system offers slightly more nuance, with certain injuries being highly amenable to conservative, non-operative management.
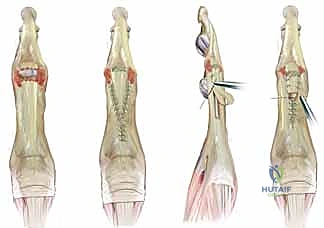
For Zone I injuries (mallet fingers), closed, purely tendinous disruptions are almost universally treated with continuous, rigid splinting of the DIP joint in slight hyperextension for 6 to 8 weeks. Surgical intervention in Zone I is generally reserved for open lacerations, massive bony avulsions involving greater than 30-50% of the articular surface, or cases complicated by volar subluxation of the distal phalanx. In contrast, open lacerations in Zones II through VIII almost universally require formal surgical exploration and primary repair to restore continuity and prevent retraction.

Closed injuries in Zone III (central slip ruptures) can often be managed conservatively if identified acutely, utilizing static PIP extension splinting while allowing active DIP flexion to pull the lateral bands dorsally. However, if a closed central slip injury presents late with an established, stiff boutonnière deformity, surgical reconstruction or tenolysis becomes necessary. Partial lacerations of the extrinsic extensors (less than 50% of the tendon cross-sectional area) in Zones VI and VII can occasionally be managed non-operatively with splinting, provided there is no extensor lag and strength is maintained, though many surgeons prefer to explore and repair to prevent delayed rupture or triggering.
| Clinical Scenario | Indications for Surgical Repair | Contraindications for Primary Repair |
|---|---|---|
| Zone I (Mallet) | Open lacerations; Bony mallet >30% articular surface; Volar subluxation of distal phalanx. | Closed tendinous mallet (splint 6-8 weeks); Small, non-displaced bony mallet. |
| Zone III (Central Slip) | Open lacerations; Displaced bony avulsions; Failed conservative management of closed rupture. | Acute, closed central slip ruptures (amenable to cylinder splinting). |
| Zone V (Sagittal Band) | Open lacerations; Chronic symptomatic subluxation failing splinting; Professional athletes requiring immediate stability. | Acute closed radial sagittal band ruptures (often managed with extension block splinting). |
| Zone VI-VIII (Extrinsic) | Complete lacerations; Partial lacerations >50%; Concomitant open fractures or neurovascular injury. | Partial lacerations <50% with full active extension against resistance; Severe, life-threatening polytrauma (delay repair). |
| Chronic/Neglected | Functional deficit impacting ADLs; Painful deformities. | Severe joint contracture (requires release first); Poor soft tissue coverage (requires flap first); Non-compliant patient. |
Contraindications to immediate primary repair include heavily contaminated or infected wounds, severe crush injuries with questionable tissue viability, and a lack of adequate soft tissue coverage. In such instances, the priority shifts to radical surgical debridement, skeletal stabilization, and wound management. The tendon ends may be tagged for future identification, and a delayed primary repair or secondary reconstruction (utilizing tendon grafts or transfers) is planned once the soft tissue envelope is pristine and stable.
Pre-Operative Planning, Templating, and Patient Positioning
Every successful surgical outcome is predicated upon meticulous preoperative planning. A cursory examination in the emergency department is insufficient; a rigorous, systematic evaluation is required to identify all injured structures and formulate a comprehensive surgical strategy.
Patient Assessment and Diagnostic Studies
The history must elucidate the exact mechanism of injury. A clean slice from a kitchen knife carries a vastly different prognosis and surgical plan than a crush-avulsion injury from industrial machinery or a heavily contaminated agricultural wound. Hand dominance, occupation, and the patient's capacity for compliance with rigorous postoperative therapy must be assessed, as these factors heavily influence the choice of repair technique and rehabilitation protocol.

The physical examination must be exhaustive. Assess the skin for viability and contamination. Perform a complete neurologic examination before the instillation of any local anesthetic. Tendon examination requires specific maneuvers to isolate individual muscle units. To test the extrinsic extensors, maintain the patient's wrist in neutral and resist MCP extension. To isolate the EIP, ask the patient to extend the index finger while keeping the other digits tightly flexed in a fist. Perform the same maneuver for the small finger to test the EDM.

For Zone III injuries, Elson's test is the gold standard for diagnosing a central slip rupture before a boutonnière deformity develops. Flex the PIP joint to 90 degrees over the edge of a table and ask the patient to extend against resistance. If the central slip is intact, the examiner will feel tension at the PIP, and the DIP will remain flail. If the central slip is ruptured, the effort of extension is transmitted entirely to the lateral bands, resulting in weak PIP extension but rigid, paradoxical extension of the DIP joint. Plain radiographs are mandatory for all extensor injuries to rule out avulsion fractures, underlying articular damage, or retained radiopaque foreign bodies.
Anesthesia Considerations and Patient Positioning
The choice of anesthesia depends heavily on the zone of injury and the anticipated extent of dissection. For distal injuries (Zones I-IV), local anesthesia utilizing a digital block and a sterile finger tourniquet is often entirely sufficient. However, for injuries in Zones V-VIII, particularly those involving retracted tendons that require proximal exploration, an upper arm pneumatic tourniquet is mandatory to ensure a bloodless surgical field.

For these proximal injuries, regional anesthesia (such as an axillary or supraclavicular brachial plexus block) is highly advantageous. It provides excellent intraoperative muscle relaxation, which is critical when attempting to mobilize and retrieve proximally retracted muscle bellies, and offers prolonged postoperative analgesia. Alternatively, the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique, utilizing lidocaine with epinephrine, is gaining immense popularity. WALANT allows the surgeon to assess the tension, glide, and integrity of the tendon repair intraoperatively by asking the patient to actively move the digit, drastically reducing the risk of postoperative gapping or rupture.

The patient is positioned supine with the affected arm extended onto a radiolucent hand table. A well-padded upper arm tourniquet is applied. The limb is prepped and draped widely, from proximal to the elbow down to the fingertips, allowing for full intraoperative assessment of the tenodesis effect and range of motion. Ensure that fine hand instruments, specialized retractors (such as Ragnell or Senn retractors), appropriate micro-sutures (typically 3-0 or 4-0 non-absorbable core sutures and 5-0 or 6-0 epitendinous sutures), and loupe magnification (minimum 2.5x, preferably 3.5x) are immediately available on the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
Alright, fellows, let us scrub in. The tourniquet is inflated to 250 mmHg, the field is meticulously prepped, and our loupe magnification is optimally adjusted. We will proceed with a systematic, tissue-respecting approach.
Incision, Exposure, and Tendon Retrieval
"Scalpel, please, a #15 blade."
We begin by incorporating the traumatic wound into our surgical incision. On the dorsum of the hand and fingers, we can safely cross over joints with longitudinal or lazy-S incisions, unlike the volar surface where such incisions would induce severe flexion contractures. We must avoid creating long, narrow skin flaps with narrow pedicles, as the dorsal skin is prone to ischemia and necrosis. A gentle curvilinear, zig-zag, or Brunner-type incision provides excellent, extensile exposure while minimizing skin tension during retraction.

Once the skin is incised, we perform careful, sharp dissection through the subcutaneous tissues. "Pickups and tenotomy scissors." We must immediately identify and protect the dorsal sensory nerve branches and major longitudinal venous channels. Retract these structures gently with vessel loops. As we expose the extensor mechanism, we assess the extent of the damage. In Zone VI injuries, we frequently find that the proximal tendon stump has retracted significantly due to muscle resting tone.

To retrieve a retracted proximal stump, we first attempt to milk the forearm musculature distally. If the tendon end appears in the wound, it is gently grasped with a fine non-crushing instrument, such as a smooth forceps or a wet sponge. Never crush the tendon end with a heavy hemostat, as this devitalizes the tissue we intend to repair. If the tendon has retracted into a proximal compartment (e.g., the EPL retracting into the third compartment), we may need to make a separate counter-incision proximally, pass a pediatric feeding tube or a wire loop distally through the compartment, suture the tendon to the loop, and gently pull it back into the primary wound.
Suture Techniques and Biomechanical Fixation
Once both tendon ends are cleanly identified and debrided of any frankly necrotic or severely frayed tissue, we proceed with the core repair. The goal of the core suture is to provide sufficient tensile strength to withstand the forces of early rehabilitation without gapping. For the extrinsic tendons in Zones IV through VIII, a robust, multi-strand core suture is required.

"Pass me a 3-0 Prolene on a non-cutting taper needle." We frequently utilize a modified Kessler, a Krackow, or a multi-strand figure-of-eight technique. The Krackow locking stitch is particularly advantageous for the flat, broad extensor tendons, as it securely grips the longitudinal collagen bundles and prevents suture pull-out. We place the core sutures carefully, ensuring the knots are buried within the repair site to minimize soft tissue irritation and adhesion formation.

Distal to Zone IV, the tendons become exceedingly thin and flat, making traditional core sutures technically impossible and biomechanically detrimental. In Zones I, II, and III, we rely on a combination of fine figure-of-eight sutures, horizontal mattress sutures, or dermatotenodesis techniques utilizing 4-0 or 5-0 monofilament. In these distal zones, the repair relies heavily on splinting for protection, as the suture purchase is inherently weak.
Following the core repair in the proximal zones, we must augment the construct with a continuous epitendinous suture. "Let's use a 5-0 or 6-0 nylon for the epitendinous running stitch." This peripheral stitch serves two critical functions: it significantly increases the overall tensile strength of the repair (by up to 30-50%), and it neatly tucks in any frayed tendon edges, creating a smooth, streamlined surface that dramatically reduces the risk of postoperative adhesions and improves tendon glide.
Before closing, we must rigorously test the repair. We release the tourniquet, achieve meticulous hemostasis using bipolar electrocautery, and assess the resting posture of the hand. The repaired digit should cascade naturally with the adjacent digits. We then passively flex and extend the wrist to observe the tenodesis effect; the repaired tendon should glide smoothly without catching or gapping. If the surgery is performed under WALANT, we ask the patient to perform active extension and flexion, allowing us to directly visualize the integrity and mechanics of our repair under physiological load.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, extensor tendon repairs are fraught with potential complications. The delicate balance between allowing sufficient healing time and preventing crippling adhesions makes the postoperative phase a proverbial tightrope walk. Recognizing these complications early and understanding the salvage options is a critical component of orthopedic mastery.
The most ubiquitous complication following extensor tendon repair is an extensor lag, defined as an inability to actively fully extend the joint despite full passive extension. This occurs due to tendon stretching, gapping at the repair site, or inadequate initial tensioning. Minor lags (10-15 degrees) at the DIP or PIP joints are common and often functionally well-tolerated, but larger lags require intervention. Conversely, a severe loss of flexion is frequently seen, driven by robust adhesion formation between the repaired tendon, the overlying skin, and the underlying periosteum or joint capsule.

Tendon rupture is a catastrophic complication, occurring in roughly 3-5% of repairs, usually secondary to patient non-compliance, overly aggressive early therapy, or failure to recognize a concomitant joint contracture. Infection, while less common in clean lacerations, can rapidly destroy a tendon repair and necessitate emergent debridement, intravenous antibiotics, and likely a delayed secondary reconstruction once the infection is eradicated.

Salvage management requires patience and precise surgical timing. Tenolysis (the surgical release of adhesions) should never be performed before 3 to 6 months post-repair. The tendon must be biologically mature and the soft tissue envelope completely soft and pliable; premature tenolysis will inevitably fail. If the tendon has ruptured or is deemed non-reconstructable due to massive substance loss, tendon transfers become the workhorse of salvage surgery. Common transfers include utilizing the EIP to restore EPL function, or transferring the Flexor Digitorum Superficialis (FDS) of the ring finger to restore common digit extension.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Extensor Lag | 20 - 40% (Zone dependent) | Tendon stretching, gapping, inadequate tensioning, poor compliance. | Prolonged extension splinting; Late shortening or plication (rarely successful). |
| Loss of Flexion (Adhesions) | 15 - 30% | Prolonged immobilization, severe initial trauma, periosteal injury. | Aggressive hand therapy; Surgical tenolysis (wait minimum 3-6 months). |
| Tendon Rupture | 3 - 5% | Non-compliance, aggressive therapy, weak core suture, infection. | Primary re-repair (if acute); Tendon graft or transfer (if delayed/retracted). |
| Boutonnière Deformity | High in missed Zone III | Failure to diagnose central slip injury; premature PIP flexion. | Serial casting/splinting; Surgical reconstruction (e.g., Fowler tenotomy, lateral band relocation). |
| Infection | 1 - 3% | Contaminated wounds, human/animal bites, poor soft tissue coverage. | Emergent I&D, targeted IV antibiotics, delayed reconstruction. |
When joint destruction is severe, or when tendon transfers are not feasible due to a lack of available donors, joint arthrodesis (fusion) remains a reliable, definitive salvage option. Fusing the DIP or PIP joint in a functional position provides a stable, pain-free digit, albeit at the permanent sacrifice of motion at that specific articulation.
Phased Post-Operative Rehabilitation Protocols
The surgical repair is merely the first step; the ultimate success of an extensor tendon repair is heavily dictated by the postoperative rehabilitation protocol. The historical standard of 4 to 6 weeks of static immobilization has largely been abandoned in favor of dynamic and early active motion protocols, which have been definitively shown to reduce adhesion formation, improve tendon excursion, and yield superior functional outcomes.

For complex repairs in Zones IV through VII, the Early Active Motion (EAM) or Relative Motion Extension (RME) protocols are currently favored. The Immediate Controlled Active Motion (ICAM) protocol utilizes a specialized splinting system. In the first phase (Weeks 0-3), the wrist is splinted in 20-30 degrees of extension. A relative motion splint (often a yoke splint) is applied to the digits, holding the injured digit in 15-20 degrees more extension relative to the adjacent uninjured digits. This capitalizes on the quadriga effect of the common muscle belly, significantly reducing the tension on the repaired tendon while allowing for immediate, controlled active flexion and extension.
During Phase II (Weeks 3-6), the wrist splint is generally discontinued, but the relative motion yoke splint is maintained. The patient is encouraged to use the hand for light, non-resistive activities of daily living. The controlled stress applied to the
Clinical & Radiographic Imaging Archive




Detailed Chapters & Topics
Dive deeper into specialized chapters regarding repair-following-traumatic-extensor-tendon-disruption-in-the-hand-wrist-and-forearm