Nail Matrix Repair, Reconstruction, and Ablation

Comprehensive Introduction and Patho-Epidemiology
The perionychium represents a highly specialized, biomechanically complex appendage at the distal terminus of the digits, serving indispensable roles in tactile sensory feedback, thermoregulation, fine motor prehension, and protection of the distal phalanx. Because of its highly exposed location, the perionychium is the most frequently injured structure in the hand, predominantly occurring in the setting of acute crush trauma. Industrial accidents, domestic crush injuries (such as door closures), and sports-related trauma constitute the vast majority of these presentations. The middle finger, given its relative length and exposure, is the most commonly injured digit.
Understanding the temporal dynamics of nail plate growth is paramount for both surgical planning and managing patient expectations. The normal nail plate grows at an average rate of 0.1 mm per day, translating to approximately 2 to 3 mm per month. When the nail plate is avulsed or surgically removed to facilitate acute nail bed repair, the physiological shock to the matrix delays the initiation of new nail growth for approximately 3 to 4 weeks. Following an acute repair where the native nail plate is replaced as a biological splint, the old nail will remain adherent for 1 to 3 months before being mechanically displaced by the advancing new nail plate.
Restoration of normal nail architecture and appearance is almost exclusively predicated on the meticulous, acute treatment of the nail matrix. Delayed or inadequate initial management invariably leads to chronic nail deformities that are notoriously difficult to reconstruct. Surgeons must counsel patients that the final aesthetic and functional outcome of a nail repair cannot be accurately assessed until approximately 12 months post-injury. Furthermore, a transient thickening of the nail plate proximal to the level of injury is a well-documented physiological response, typically persisting for about 50 days post-trauma, before the matrix resumes the production of a normal, uniform plate.
Beyond acute trauma, the perionychium is subject to various neoplastic processes. Benign tumors, such as glomus tumors and mucous cysts (distal interphalangeal joint ganglions), as well as malignant neoplasms, including squamous cell carcinoma and subungual melanoma, frequently necessitate surgical excision. The extirpation of these lesions often creates critical matrix defects, requiring the exact reconstructive techniques utilized in severe traumatic avulsions to restore form and function.
Detailed Surgical Anatomy and Biomechanics
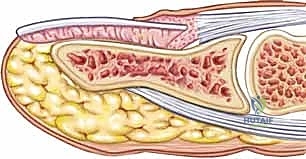
Optimal surgical management of fingertip trauma demands an exhaustive understanding of the perionychial components—the skin, sterile matrix, germinal matrix, eponychial fold, and the osseous distal phalanx—and their intricate spatial relationships. The perionychium functions as an integrated unit. It is composed of the nail plate, the underlying nail bed, the hyponychium, the eponychium and its associated fold, and the paronychium.

The Germinal and Sterile Matrices
The nail bed is anatomically and functionally divided into two distinct regions. The proximal portion, residing largely beneath the eponychial fold, is the germinal matrix. The germinal matrix is the primary engine of nail generation, responsible for producing approximately 90% of the total volume of the nail plate. The macroscopic manifestation of the distal extent of the germinal matrix is the lunula, the white, crescent-shaped opacity at the base of the nail.
Distal to the lunula lies the sterile matrix, which extends to the hyponychium. While the sterile matrix contributes only the remaining 10% of the nail plate's volume, its primary biomechanical function is the production of specialized cells on the undersurface of the nail plate. These cells act as a biological adhesive, ensuring the firm adherence of the nail plate to the underlying bed. Injury to the sterile matrix predictably results in non-adherence and subsequent deformity.
Peripheral Soft Tissue Structures
The peripheral soft tissues provide structural boundaries and protection for the growing nail. The hyponychium is the specialized, keratinized skin immediately distal to the sterile matrix, marking the transition from the nail bed to the volar fingertip skin. The paronychium comprises the lateral cutaneous folds bordering the nail plate on each side. The eponychium (cuticle) is the distal extension of the proximal nail fold, providing a critical waterproof seal that protects the underlying germinal matrix from environmental pathogens.
Osteocutaneous Relationship
A critical anatomical feature of the nail bed is its direct, unyielding adherence to the periosteum of the distal phalanx. There is virtually no subcutaneous fat interposed between the sterile matrix and the bone. Consequently, the nail bed relies entirely on the structural integrity of the distal phalanx for its flat contour. This intimate relationship explains why approximately 50% of all nail bed injuries are associated with an underlying distal phalanx fracture. Loss of this bony support inevitably leads to a contour deformity of the nail, most notably the hook nail deformity.
Exhaustive Indications and Contraindications
Surgical intervention on the nail matrix is dictated by the mechanism of injury, the presence of underlying fractures, and the chronicity of the presentation. In the acute setting, aggressive and precise repair yields the highest probability of a cosmetically and functionally normal nail.
| Category | Indications for Surgery | Contraindications |
|---|---|---|
| Acute Trauma | Subungual hematoma >50% of nail surface; Displaced nail plate; Stellate or crush lacerations; Avulsion injuries; Open distal phalanx fractures. | Active, uncontrolled local infection (relative); Severe vascular compromise requiring proximal amputation; Medical instability precluding safe anesthesia. |
| Chronic Deformity | Symptomatic split nail deformity; Painful hook nail; Pincer nail deformity causing soft tissue impingement; Chronic non-adherence. | Asymptomatic, purely cosmetic deformities in medically non-compliant patients; Lack of adequate donor sites for massive reconstruction. |
| Neoplastic | Excision of glomus tumors (pain, cold intolerance); Mucous cysts threatening nail matrix; Biopsy/excision of suspected melanoma or SCC. | Incomplete oncologic workup for suspected malignant lesions without defined surgical margins. |
Pre-Operative Planning, Templating, and Patient Positioning
In the acute trauma setting, a systematic evaluation of the entire fingertip is mandatory before focusing on the nail. The surgeon must assess the viability and quality of the surrounding skin, the presence and extent of a subungual hematoma, the integrity of the nail matrix, capillary refill, two-point discrimination for digital nerve function, and the active range of motion at the distal interphalangeal (DIP) joint.
Imaging Protocols
Standard anteroposterior (AP) and lateral radiographs of the affected digit are non-negotiable. Given that 50% of nail bed crush injuries involve a distal phalanx fracture, the surgeon must actively rule out osseous involvement.
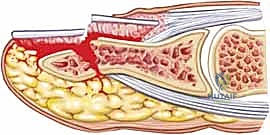
Fractures associated with nail bed lacerations represent open fractures. A break in the periosteum establishes direct communication between the distal phalanx and the external environment, carrying a significant risk of osteomyelitis if not treated with thorough irrigation, aggressive débridement, and appropriate antibiotic prophylaxis. Depending on the level of the crush, the surgeon may encounter distal tuft fractures, highly comminuted diaphyseal fractures, or transverse/oblique midshaft fractures. Intra-articular fractures extending into the DIP joint are relatively rare but must be identified.
Anesthesia and Hemostasis
A bloodless surgical field is an absolute prerequisite for nail matrix repair, as the tissue is delicate, and visualization of the matrix margins under magnification is critical.
1. Anesthesia: A digital block utilizing 1% plain lidocaine (without epinephrine, though modern literature increasingly supports epinephrine use, plain lidocaine remains the classic textbook standard) is administered. The maximum safe dose is 7 mg/kg.
2. Tourniquet: Exsanguination of the digit followed by the application of a Penrose drain tourniquet at the base of the digit, secured with a hemostat, is highly recommended.

Crucial Warning: The use of a rolled-up portion of a surgical glove as a tourniquet is strictly discouraged. It is easily forgotten beneath bulky postoperative dressings, leading to catastrophic vascular compromise, ischemia, and subsequent necrosis of the digit.
Surgical Preparation and Equipment
Sterile preparation and draping are performed meticulously to prevent the introduction of nosocomial bacteria into the subungual space. The use of surgical loupes providing at least 2.5x magnification is mandatory. The matrix is incredibly friable, and macroscopic repair inevitably leads to malalignment and subsequent scarring. A Kleinert elevator or a fine periosteal elevator is required for the atraumatic separation of the nail plate from the underlying matrix.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach is dictated by the specific pathology, ranging from simple hematoma decompression to complex micro-surgical grafting.
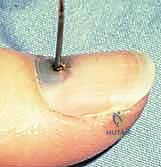
Drainage of Subungual Hematoma
A subungual hematoma generates intense, throbbing pain secondary to the accumulation of blood in the rigid, enclosed space between the nail plate and the nail bed. If the hematoma involves less than 50% of the visible nail and the nail plate is firmly adherent and intact, simple decompression is indicated.
Trephination of the nail plate can be swiftly accomplished using a heated paper clip, a large-bore needle, or a handheld, battery-powered electrocautery device. The goal is to melt a small hole through the inert nail plate without penetrating and thermally injuring the underlying sterile matrix.

Conversely, if the hematoma elevates more than 50% of the nail, or if the nail edges are disrupted, the nail plate must be completely removed to explore and repair the underlying laceration.
Repair of Acute Nail Bed Lacerations
Nail bed lacerations present in four primary morphologies: simple, stellate, severe crush, and avulsion.
1. Exposure: The Kleinert elevator is gently introduced beneath the free edge of the nail plate. By sweeping proximally and laterally, the plate is separated from the sterile and germinal matrices.
2. Nail Plate Preservation: Once removed, the nail plate is thoroughly cleaned, scrubbed, soaked in a povidone-iodine (Betadine) solution, and rinsed with normal saline. It will be utilized later as a biological splint.
3. Matrix Repair: The lacerated edges of the matrix are identified under loupe magnification. Aggressive débridement must be strictly avoided; only clearly necrotic, non-viable tissue should be excised to preserve every millimeter of matrix. The matrix is meticulously reapproximated using fine, absorbable sutures—typically 7-0 chromic gut on a spatulated micro-needle.


- Fracture Management: If an underlying distal phalanx fracture is displaced or unstable, it must be reduced and stabilized with longitudinal or crossed Kirschner wires (K-wires) prior to matrix repair to provide a rigid foundation.
- Splinting: The sterilized native nail plate is reinserted into the proximal eponychial fold. This step is vital to prevent the eponychial fold from scarring down to the germinal matrix (synechiae formation), which would permanently arrest nail growth. The plate also serves as an excellent splint for underlying tuft fractures. It is secured with a figure-of-8 suture of 5-0 nylon or a simple stitch securing the distal nail to the hyponychium. If the native nail is lost or destroyed, a custom-cut piece of sterile silicone sheet or non-adherent gauze must be utilized as a substitute.
Exposure of the Germinal Matrix
In cases of proximal avulsions, the germinal matrix may be torn and retracted deep beneath the eponychium. Blind repair is impossible and dangerous. To gain adequate exposure, bilateral incisions are made perpendicular to the curved portions of the eponychial fold. The eponychial flap is elevated dorsally, exposing the entire germinal matrix for precise anatomical repair.


Treatment of Nail Bed Defects and Reconstruction
When trauma or tumor extirpation results in a tissue void, the defect must be addressed to prevent severe deformity. Small defects (less than 5 mm) may occasionally be left to heal by secondary intention, but this carries a high risk of recurrent scarring and localized nail deformity.
Defects larger than 5 mm require grafting.
1. Sterile Matrix Defects: These are best treated with split-thickness nail bed grafts. The donor site can be the adjacent uninjured nail bed of the same digit, a non-injured adjacent finger, or the sterile matrix of the great toe. Using a No. 15 scalpel blade, a razor-thin layer of sterile matrix is harvested, ensuring the donor site retains enough basal cells to re-epithelialize. The graft is transferred to the defect and secured with 7-0 chromic sutures.







- Germinal Matrix Defects: Loss of the germinal matrix means loss of nail production. Reconstruction requires a full-thickness germinal matrix graft. Because harvesting full-thickness germinal matrix ablates nail growth at the donor site, a toe (preferably the second toe) is utilized.






Nail Matrix Ablation
In cases of severe, recalcitrant deformity, chronic fungal infections refractory to medical management, or complete loss of bony support where reconstruction is impossible, complete nail matrix ablation is indicated. This can be achieved chemically via the application of 89% phenol to the germinal matrix after nail extraction, or surgically by sharply excising the entire germinal matrix down to the periosteum, ensuring no residual matrix cells remain to form painful nail spicules.
Complications, Incidence Rates, and Salvage Management
Inadequate acute treatment, severe initial crush mechanisms, or postoperative infections frequently lead to chronic posttraumatic nail deformities. Reconstruction of these chronic injuries must be approached with highly realistic expectations, as restoring a perfectly normal nail is exceedingly difficult.
Common Nail Deformities
- Split Nail Deformity: Caused by longitudinal scarring within the sterile or germinal matrix. The scar tissue lacks the specialized cells to produce or adhere to the nail plate, resulting in a longitudinal fissure. Salvage requires complete excision of the scar and primary closure of the matrix. If the resulting defect is too wide for tension-free closure, a split-thickness graft from the great toe is required.
- Non-adherence: Usually due to extensive injury to the sterile matrix. The nail plate grows but fails to attach to the bed, catching on clothing and causing pain. Treatment involves excision of the non-adherent bed and split-thickness grafting.
- Hook Nail Deformity: Arises from a combination of excessive volar tension at the junction of the nail bed and hyponychial skin, coupled with a loss of osseous support from the distal phalanx (often following a distal tuft amputation). The nail curves sharply over the fingertip. Salvage requires reconstruction of the nail bed, release of volar tethering, and structural bone grafting to the distal tip of the phalanx to restore support.
- Nail Remnant (Spicule): Caused by the presence of residual germinal matrix cells that were incompletely ablated during an initial repair or a revision amputation. These spicules are highly painful. Treatment requires formal re-exploration and complete surgical ablation of the offending remnant.
- Pincer Nail Deformity: Characterized by excessive, progressive transverse curvature of the nail plate. It pinches the distal fingertip soft tissues, causing severe pain and aesthetic abnormality. Management ranges from partial or complete nail ablation to complex reconstruction involving the elevation of the lateral nail bed using dermal grafts or acellular dermal matrices (e.g., AlloDerm) to flatten the contour.






| Complication | Pathophysiology | Surgical Salvage Strategy |
|---|---|---|
| Split Nail | Matrix scarring preventing continuous plate formation. | Scar excision; primary micro-repair or split-thickness toe graft. |
| Hook Nail | Loss of distal phalanx bony support; volar scar tethering. | Volar release; structural bone grafting; revision amputation if severe. |
| Pincer Nail | Excessive transverse curvature pinching soft tissue. | Lateral nail bed elevation with dermal matrix; partial/total ablation. |
| Osteomyelitis | Untreated open distal phalanx fracture. | Hardware removal; aggressive bone débridement; IV antibiotics. |
Phased Post-Operative Rehabilitation Protocols
Postoperative management is heavily focused on protecting the delicate surgical repair while preventing joint stiffness.
Phase I: Acute Protection (Weeks 0-3)
Immediately postoperatively, the digit is dressed with non-adherent gauze (e.g., Adaptic or Xeroform) followed by a bulky, protective soft dressing. If a fracture was pinned, a protective splint is applied to immobilize the DIP joint. The patient is instructed to keep the hand elevated above heart level for the first 48 to 72 hours to minimize throbbing pain and edema. The first dressing change is typically performed at 5 to 7 days in the clinic. The replaced nail plate (or silicone sheet) must not be disturbed.
Phase II: Matrix Healing and Splint Retention (Weeks 3-12)
By week 3, the initial acute healing of the matrix is complete. If K-wires were utilized for fracture fixation, they are generally removed between 4 and 6 weeks once clinical and radiographic union is achieved. The replaced native nail or silicone splint is left in place. Patients are advised that the old nail will slowly detach and fall off spontaneously between 1 to 3 months as the new nail plate begins to push outward from the germinal matrix.
Phase III: Maturation and Remodeling (Months 3-12)
During this phase, the new nail plate becomes visible. The patient must be aggressively counseled regarding the expected visual changes. Thickening, ridging, and irregularity of the nail proximal to the level of injury are entirely normal and are typically observed for the first 50 days of new growth. Gentle massage of the eponychial fold can help desensitize the digit. The surgeon should defer any consideration of revision surgery for at least 12 months, as the nail bed undergoes continuous remodeling, and the final aesthetic outcome cannot be judged until a complete cycle of nail growth has occurred.
Summary of Landmark Literature and Clinical Guidelines
The foundational principles of nail bed repair were largely established by Dr. Elvin G. Zook and colleagues, who pioneered the meticulous, microsurgical approach to perionychial trauma. Landmark studies have consistently demonstrated that the use of magnification (loupes or operating microscope) and fine absorbable suture (7-0 or 8-0 chromic) significantly reduces the incidence of secondary nail deformities compared to macroscopic repair.
Furthermore, clinical guidelines strongly advocate for the preservation and replacement of the native nail plate whenever possible. Literature indicates that the native plate provides superior splinting of the eponychial fold and maintains the physiological contour of the sterile matrix better than synthetic alternatives. However, in cases of severe avulsion where the plate is lost, the use of medical-grade silicone sheeting has been validated as a safe and effective alternative to prevent synechiae formation.
For neoplastic conditions, particularly subungual melanoma, guidelines dictate that management requires an acute understanding of safe amputation levels—usually requiring disarticulation at the DIP joint or more proximally—and the integration of sentinel lymph node biopsy protocols as determined by the depth of invasion. Reconstruction of the nail matrix after tumor excision remains a secondary priority to achieving definitive oncologic clearance.
