Mastering Fibular Resections: An Intraoperative Guide to Oncologic Limb Salvage
Key Takeaway
Join us in the operating theater for a masterclass on fibular resections. We'll meticulously cover patient positioning, detailed surgical anatomy, and step-by-step intraoperative execution for benign-aggressive and malignant tumors. Learn precise techniques for curettage, Type I, and Type II resections, emphasizing neurovascular preservation and reconstruction. Gain insights into critical pearls, potential pitfalls, and comprehensive postoperative management to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we delve into the intricate world of fibular resections, a procedure that, while seemingly straightforward in its osseous execution, demands profound anatomical knowledge and meticulous surgical technique regarding the surrounding soft tissue envelope. The fibula, historically dismissed as a mere non-weight-bearing strut, plays indispensable roles in both ankle and knee biomechanics. Its unique anatomical relationships, particularly its intimate proximity to the common peroneal nerve and the popliteal vascular trifurcation, make oncologic tumor resection a challenging yet profoundly rewarding endeavor in the realm of limb salvage surgery.
Historically, primary and metastatic bone tumors involving the fibula were managed with radical ablative procedures, most commonly above-knee amputations. This draconian approach was driven by the complex compartmental anatomy of the leg and the high risk of local recurrence associated with marginal excisions. However, the paradigm has shifted dramatically. Advancements in neoadjuvant chemotherapy, sophisticated high-resolution cross-sectional imaging, and a deeper understanding of regional microvascular anatomy have spurred the development of complex limb-sparing procedures. Today, en bloc resection of the fibula with wide oncologic margins is the standard of care for most localized fibular malignancies.
Epidemiologically, primary bone tumors of the fibula are relatively rare, accounting for approximately 2% to 3% of all primary bone neoplasms. When they do manifest, they exhibit a distinct predilection for the proximal third of the bone, followed by the diaphysis, and least commonly, the distal third. Osteosarcoma and Ewing sarcoma are the most frequent primary malignant entities encountered in the pediatric and adolescent populations, whereas chondrosarcoma and undifferentiated pleomorphic sarcoma dominate the adult demographic. Benign-aggressive lesions, such as giant cell tumors of bone (GCTB) and aneurysmal bone cysts (ABC), also frequently target the proximal fibula and often require aggressive en bloc resection rather than simple intralesional curettage to minimize recurrence.
The overarching goal of this chapter is to equip the orthopedic oncologist, fellow, and resident with the advanced anatomical knowledge and surgical acumen required to perform these resections safely and effectively. We will meticulously navigate the preoperative planning phases, dissect the complex neurovascular relationships, detail the step-by-step surgical execution of proximal, diaphyseal, and distal resections, and finally, outline the reconstructive techniques necessary to restore joint stability and maximize postoperative functional outcomes.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate and unforgiving anatomy surrounding the fibula is paramount to achieving clear oncologic margins while preventing catastrophic iatrogenic complications. The fibula is essentially a muscular aponeurotic strut, completely enveloped by the origins and insertions of the leg's musculature, which simultaneously acts as a barrier to tumor spread and a complex web to navigate during resection.
Proximal Fibula
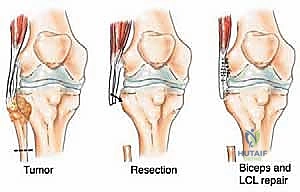
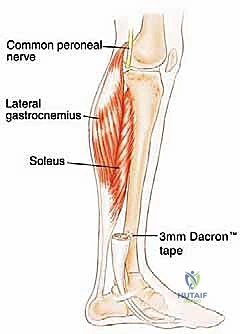
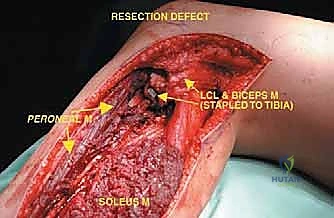
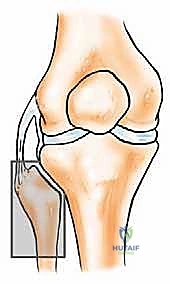
The proximal fibula is an anatomically dense and perilous region. Osteologically, the fibular head articulates with the posterolateral aspect of the lateral tibial condyle, forming the proximal tibiofibular joint—a synovial joint that dissipates torsional stresses applied to the ankle. Biomechanically, the fibular head is the critical anchor point for the lateral collateral ligament (LCL) and the biceps femoris tendon. Together, these structures form the primary restraint to varus stress and posterolateral rotatory instability of the knee. Resection of the proximal fibula inherently destroys this stabilizing complex, mandating meticulous soft tissue reconstruction to the lateral tibia to prevent chronic knee instability.
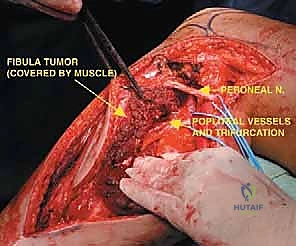
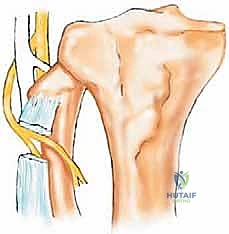
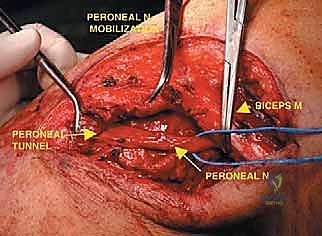
Neurovascularly, the proximal fibula is dominated by the common peroneal nerve (CPN). Originating from the sciatic nerve bifurcation in the distal thigh, the CPN courses superficially and obliquely along the medial border of the biceps femoris. It wraps around the posterior aspect of the fibular neck, directly against the periosteum, before diving anteriorly into the fibro-osseous peroneus longus tunnel. Within this tunnel, it bifurcates into the superficial and deep peroneal nerves. This intimate bone-nerve relationship means any proximal fibular tumor expansion places the CPN at immediate risk. Iatrogenic injury results in a devastating foot drop (loss of ankle dorsiflexion and eversion) and sensory deficits over the anterolateral leg and dorsum of the foot.
Posteromedial to the proximal fibula lies the popliteal vascular trifurcation. The popliteal artery descends beneath the tendinous arch of the soleus and divides into the anterior tibial artery and the tibioperoneal trunk. The anterior tibial artery is of critical surgical significance during fibular resection; it passes directly anteriorly through the proximal hiatus of the interosseous membrane, intimately tethering the vascular bundle to the fibula and restricting mobilization. The peroneal artery, a branch of the tibioperoneal trunk, descends along the medial crest of the fibula, supplying the bone via nutrient branches and providing the vascular basis for free vascularized fibular grafts.
Fibular Diaphysis
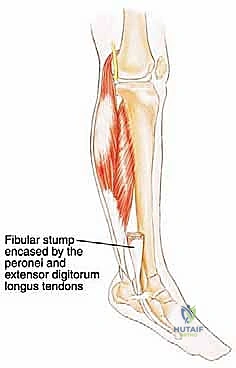
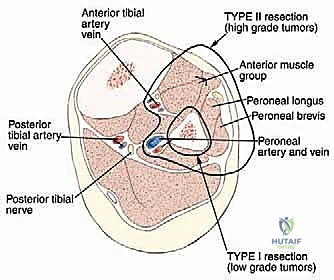
The fibular diaphysis is circumferentially cloaked by the origins of the leg musculature, dividing the leg into its functional compartments. Anteriorly, it provides origin to the extensor digitorum longus, extensor hallucis longus, and peroneus tertius. Laterally, it anchors the peroneus longus and brevis. Posteriorly, it supports the soleus, flexor hallucis longus, and tibialis posterior. The interosseous membrane, a robust fibrous sheet, spans the gap between the interosseous crests of the tibia and fibula, serving as a critical compartmental barrier to tumor extension.
During diaphyseal (intercalary) resections, this muscular envelope provides a natural oncologic barrier. However, achieving a wide margin requires resecting a cuff of normal muscle contiguous with the bone. The deep peroneal nerve and anterior tibial vessels course along the anterior aspect of the interosseous membrane, while the peroneal vessels descend along the posterior aspect, deeply embedded within the flexor hallucis longus. Meticulous subperiosteal dissection is contraindicated in oncologic resections; therefore, the surgeon must navigate these vascular planes extra-periosteally, safely ligating muscular branches while preserving the main axial vessels.
Distal Fibula
The distal fibula expands to form the lateral malleolus, a subcutaneous structure with minimal soft tissue coverage, making it highly susceptible to direct tumor extension into the superficial dermis. Biomechanically, the lateral malleolus is the cornerstone of the ankle mortise, providing the lateral buttress that prevents lateral talar shift. It is secured to the tibia via the robust syndesmotic ligament complex (anterior inferior tibiofibular ligament, posterior inferior tibiofibular ligament, and interosseous ligament).
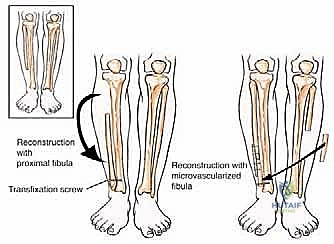
Distally, the fibula also provides the origin for the lateral collateral ligaments of the ankle—the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). Resection of the distal fibula for malignancy necessitates complex reconstructive strategies, ranging from primary ankle arthrodesis using structural allografts or endoprostheses to complex ligamentous reconstructions, depending on the extent of the resection and the functional demands of the patient.
Exhaustive Indications and Contraindications
The decision-making algorithm for fibular resection is highly nuanced, dictated by the tumor's histologic diagnosis, anatomical stage, biological aggressiveness, and the patient's overall functional status. The primary objective is absolute oncologic clearance (R0 resection) with maximal preservation of limb function. A multidisciplinary tumor board consensus is mandatory before proceeding with surgical intervention.
Indications
Primary bone sarcomas (e.g., osteosarcoma, Ewing sarcoma, chondrosarcoma, fibrosarcoma) localized to the fibula represent the absolute indication for en bloc resection. For these high-grade malignancies, the surgical plan must include a wide margin, resecting the bone along with a continuous cuff of normal surrounding muscle and the adjacent interosseous membrane. Neoadjuvant chemotherapy is typically administered for osteosarcoma and Ewing sarcoma, and the surgical resection is timed post-induction to capitalize on tumor necrosis and pseudocapsule formation.
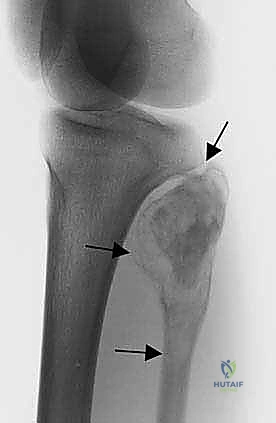
Benign-aggressive tumors, such as Campanacci Grade III giant cell tumors or recurrent aneurysmal bone cysts, frequently destroy the fibular cortex and expand into the surrounding soft tissues. While these are technically benign, their locally destructive nature and high recurrence rates following intralesional curettage make en bloc marginal or wide resection the preferred, definitive treatment. Resection virtually eliminates the risk of local recurrence and avoids the complications associated with massive bone grafting or cementation in a mechanically compromised strut.
Metastatic lesions to the fibula are relatively uncommon and are generally managed non-operatively with systemic therapy and external beam radiation, given the bone's non-weight-bearing nature in its diaphyseal region. However, surgical resection is indicated in select scenarios: intractable pain refractory to radiation, impending or actual pathologic fracture causing severe mechanical instability (particularly in the proximal or distal thirds), or as a curative-intent metastasectomy in patients with isolated oligometastatic disease (e.g., renal cell carcinoma or thyroid carcinoma).
Contraindications
Limb salvage via fibular resection is strictly contraindicated when a wide oncologic margin cannot be achieved without compromising the viability or essential function of the limb. The most critical contraindication is gross, circumferential encasement of the major neurovascular bundles—specifically the popliteal artery, tibioperoneal trunk, or the tibial nerve. While isolated resection and grafting of the anterior tibial or peroneal vessels are feasible, involvement of the main posterior tibial bundle or sciatic/tibial nerve typically mandates an above-knee amputation to achieve local control.
Extensive multicompartmental soft tissue involvement, particularly deep extension into the posterior compartment infiltrating the deep flexors and the posterior tibial neurovascular bundle, precludes a safe limb-sparing resection. Additionally, massive tumor extension directly invading the adjacent tibia necessitates a complex en bloc resection of both bones, which carries an exceptionally high morbidity rate and often results in a functionally inferior limb compared to a well-fitted modern prosthesis following amputation.
| Category | Indications for Fibular Resection | Contraindications for Limb Salvage |
|---|---|---|
| Tumor Type | Primary Bone Sarcomas (Osteosarcoma, Ewing, Chondrosarcoma) | Gross encasement of Tibial Nerve or Popliteal Trifurcation |
| Benign/Aggressive | Giant Cell Tumor (Grade 3), aggressive ABCs | Massive invasion of the adjacent Tibia requiring total leg resection |
| Metastatic | Intractable pain, impending fracture, isolated oligometastasis | Extensive multicompartmental soft tissue infiltration |
| Patient Factors | Good baseline function, favorable response to neoadjuvant therapy | Medically unfit for prolonged surgery, severe peripheral vascular disease |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough, exhaustive preoperative planning is the bedrock of a successful oncologic resection. The surgeon must transition from a conceptual understanding of the tumor to a precise, three-dimensional intraoperative roadmap. This requires a meticulous review of all imaging modalities and a strategic approach to patient positioning and operating room setup.
Imaging and Staging Studies
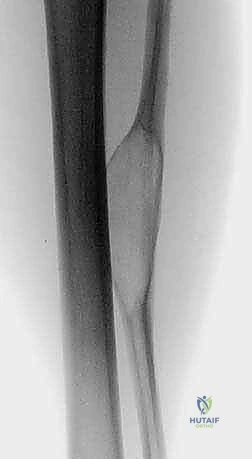
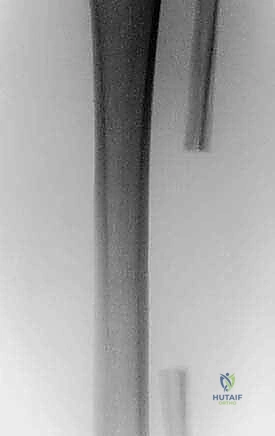
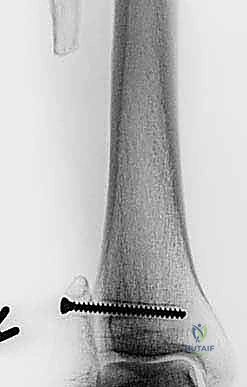
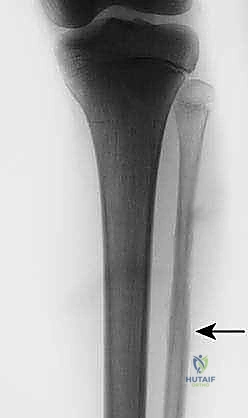
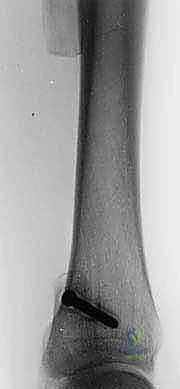
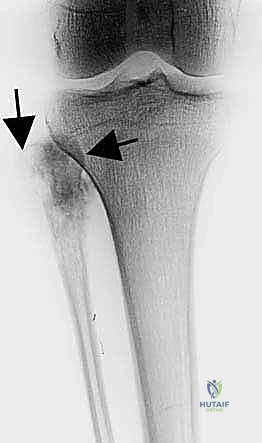
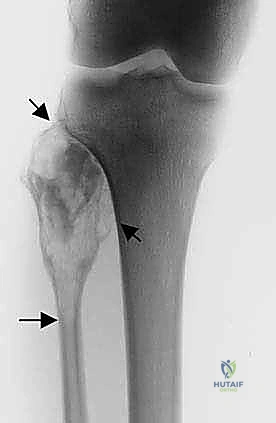
The initial evaluation begins with high-quality orthogonal plain radiographs of the entire tibia and fibula. These provide a macroscopic overview of bone destruction, periosteal reaction patterns (e.g., Codman's triangle, sunburst appearance), and the presence of pathologic fractures. However, plain films drastically underestimate the true extent of intramedullary and extraosseous tumor spread.
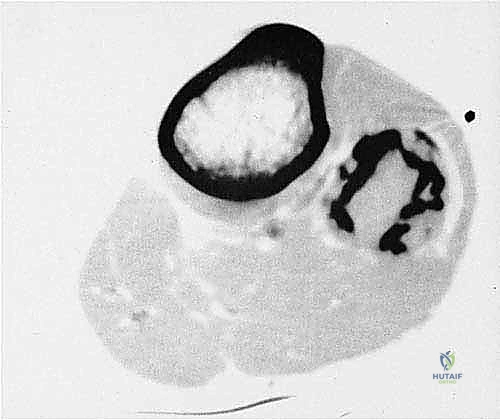
Computed Tomography (CT) of the affected extremity is essential for defining the precise limits of cortical osteolysis and identifying subtle matrix mineralization. More importantly, CT provides exquisite detail regarding the anatomical relationship between the fibular tumor and the adjacent tibial cortex, helping to determine if the tibia is at risk or frankly invaded.
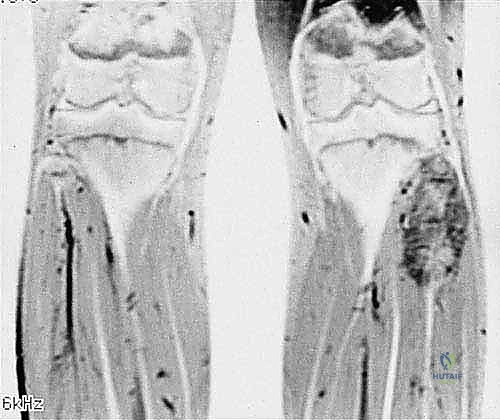
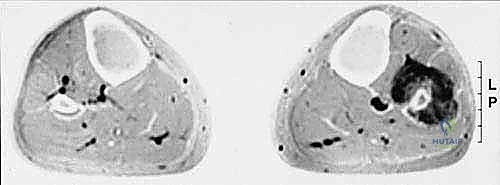
Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the gold standard for local staging. T1-weighted longitudinal images are critical for defining the intramedullary extent of the tumor and identifying skip metastases within the same bone. T2-weighted and STIR sequences perfectly delineate the extraosseous soft tissue mass, its relationship to the compartmental fascial boundaries, and, crucially, its proximity to the common peroneal nerve and the popliteal trifurcation. The MRI dictates the exact level of the planned bone osteotomies to ensure a minimum of 3 to 5 centimeters of normal marrow margin.
Biopsy Principles
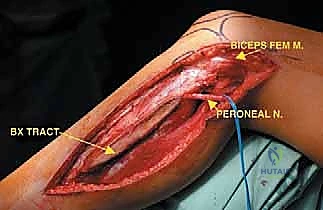
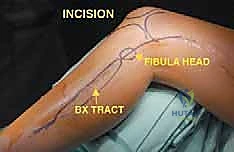
Prior to definitive resection, a core needle or incisional biopsy is mandatory to establish the histologic diagnosis. The placement of the biopsy tract is a critical oncologic principle: the tract must be considered contaminated with tumor cells and must be excised en bloc with the definitive specimen. Therefore, the biopsy incision must be meticulously planned to lie perfectly in line with the planned utilitarian surgical incision for the fibular resection. Poorly placed transverse biopsies can irrevocably compromise the soft tissue flaps, forcing an otherwise avoidable amputation.
Patient Positioning and Setup
The patient is positioned in a semisupine (bumpy supine) position on a radiolucent operating table. A large gel bump or sandbag is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the fibula directly towards the ceiling. The operative extremity is prepped and draped entirely free, from the inguinal ligament down to the toes.
This extensive free draping is non-negotiable. It allows the surgeon to freely manipulate the knee and ankle joints throughout the procedure, facilitating access to different anatomical compartments. It permits continuous intraoperative monitoring of distal pedal pulses, which is vital when dissecting near the trifurcation. Furthermore, it ensures that the sterile field is already prepared should intraoperative findings (such as unexpected vascular encasement) necessitate an immediate conversion to an above-knee amputation. A sterile tourniquet is applied high on the thigh but is generally left uninflated; operating without a tourniquet allows for better identification of small bleeding vessels and prevents ischemic injury to nerves that are already undergoing surgical manipulation.

Step-by-Step Surgical Approach and Fixation Technique
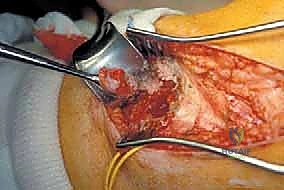
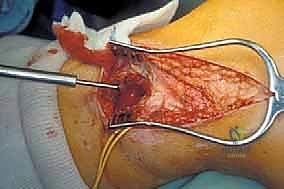
The surgical execution of a fibular resection demands a seamless blend of blunt compartmental dissection and sharp, precise neurovascular skeletonization. We will detail the approach using the classic utilitarian incision, adaptable for proximal, intercalary, and distal resections.
The Utilitarian Incision and Flap Creation
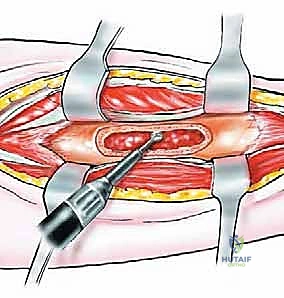
The universal approach to the fibula utilizes a curvilinear lateral incision. For a total or proximal resection, the incision begins 5 centimeters proximal to the knee joint line, following the posterior border of the biceps femoris tendon. It crosses the joint line, curves gently anteriorly over the lateral compartment of the leg, and descends towards the lateral malleolus.
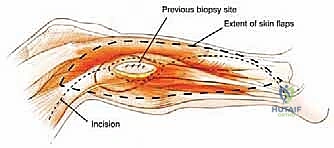
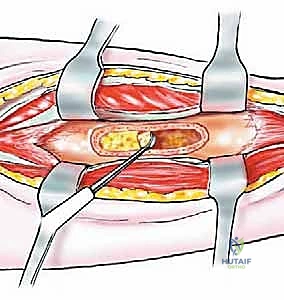
Thick, full-thickness fasciocutaneous flaps are raised anteriorly and posteriorly. It is imperative to maintain the deep fascia attached to the subcutaneous tissue to preserve the subdermal vascular plexus, preventing flap necrosis. The anterior flap is elevated to expose the anterior intermuscular septum, while the posterior flap is retracted to reveal the lateral gastrocnemius and soleus. The previous biopsy tract, marked by an ellipse of skin, is left attached to the underlying tumor mass.
Proximal Fibular Resection (Malawer Type I/II)
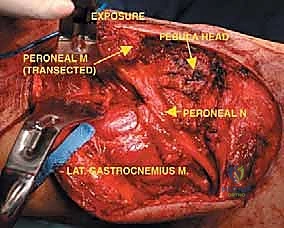
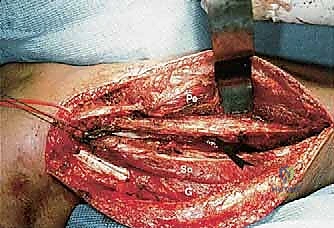
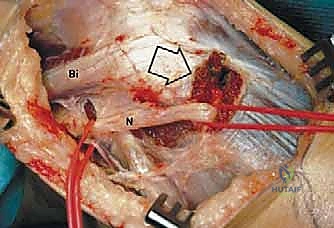
The most critical step in proximal resections is the early identification and protection of the common peroneal nerve. The nerve is located proximally, deep to the medial border of the biceps femoris. It is carefully neurolysed and traced distally as it winds around the fibular neck. Vessel loops are utilized for gentle retraction. If the tumor intimately involves the nerve sheath, the nerve must be sacrificed to achieve oncologic margins, accepting the resulting foot drop.


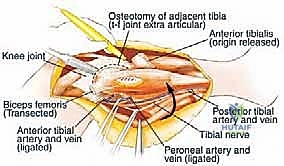
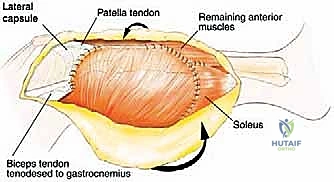
Once the nerve is secured, the biceps femoris tendon and the LCL are sharply detached from the fibular head, tagging them with heavy non-absorbable sutures for later reconstruction. The anterior compartment musculature is then transected at a safe distance from the tumor pseudocapsule. As dissection proceeds medially, the anterior tibial recurrent artery and the main anterior tibial artery are identified as they pass through the interosseous membrane. These vessels are carefully ligated and divided to free the proximal fibula from the vascular axis.
The proximal tibiofibular joint capsule is incised. A Gigli saw or an oscillating saw is passed around the fibular diaphysis at the pre-calculated MRI margin (typically 3-5 cm distal to the tumor extent).
Clinical & Radiographic Imaging Archive