Repairing Chronic Quadriceps Tendon Ruptures: A Definitive Guide

Key Takeaway
Discover the latest medical recommendations for Repairing Chronic Quadriceps Tendon Ruptures: A Definitive Guide. Chronic quadriceps tendon ruptures signify a prolonged disruption of the quadriceps tendon fibers, severely impairing the knee's extensor mechanism. These injuries commonly occur in patients over 40, often at a degenerated site approximately 2 cm above the patella, resulting from eccentric contraction against sudden load. Unrepaired ruptures invariably lead to persistent extensor lag and weakness.
Introduction and Epidemiology
Quadriceps tendon ruptures represent a catastrophic disruption of the knee extensor mechanism, characterized by the mechanical discontinuity of the quadriceps muscle complex from its insertion at the superior pole of the patella. While acute ruptures are well-described entities managed with prompt surgical repair, chronic quadriceps tendon ruptures—typically defined as injuries presenting more than four to six weeks post-injury—pose a substantially more complex surgical challenge. The delay in diagnosis or treatment allows for progressive tendon retraction, profound muscular atrophy, quadriceps fibrosis, and the development of patella baja, necessitating advanced reconstructive techniques rather than simple primary repair.

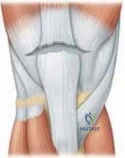
Epidemiologically, quadriceps tendon ruptures predominantly affect patients in their fifth to seventh decades of life, with a marked male predilection (male-to-female ratio approaching 8 to 1). Ruptures typically occur transversely through the tendon at a pathologic, degenerative watershed area located approximately 1 to 2 cm proximal to the superior pole of the patella. Depending on the magnitude and duration of the applied force, the tear may progress obliquely into the medial and lateral retinacula. In older patient populations, ruptures frequently occur directly at the bone-tendon interface, whereas younger patients may sustain mid-substance or musculotendinous junction failures.
Unilateral ruptures are the most common presentation. However, bilateral simultaneous ruptures are well-documented and should immediately raise clinical suspicion for underlying systemic metabolic or endocrinologic conditions. Systemic diseases predisposing patients to tendinopathy and subsequent rupture include end-stage renal disease, hyperparathyroidism, gout, pseudogout, systemic lupus erythematosus, and diabetes mellitus. Furthermore, iatrogenic factors, notably the prolonged use of systemic or local corticosteroids and the administration of fluoroquinolone antibiotics, significantly compromise tendon tensile strength and are frequently implicated in the pathogenesis of both acute and chronic ruptures.
Surgical Anatomy and Biomechanics
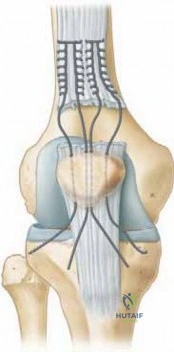
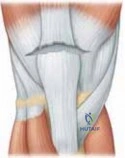
A profound understanding of the extensor mechanism anatomy is mandatory for the successful reconstruction of chronic quadriceps tendon ruptures. The quadriceps tendon is a complex, multilaminar structure formed by the coalescence of the four constituent muscles of the quadriceps femoris: the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius. This coalescence occurs approximately 3 to 5 cm proximal to the superior pole of the patella.

Morphologically, the normal quadriceps tendon averages 8 mm in thickness and 35 mm in width at its insertion. It is anatomically stratified into three distinct laminae:
1. The superficial layer, composed exclusively of the tendinous fibers originating from the rectus femoris.
2. The middle layer, formed by the decussating aponeurotic fibers of the vastus medialis and vastus lateralis.
3. The deep layer, which originates from the anterior fascia of the vastus intermedius.
The vascular supply to the quadriceps tendon is derived from a rich anastomotic network comprising branches of the lateral circumflex femoral artery, the descending geniculate artery, and the medial and lateral superior geniculate arteries. However, the intra-tendinous microvascular distribution is markedly asymmetric. While the superficial lamina maintains a robust and complete vascular supply from the musculotendinous junction down to the patellar insertion, the deep portion of the tendon contains a well-defined oval avascular zone. This hypovascular region, located approximately 1 to 2 cm proximal to the patellar insertion, correlates precisely with the most frequent site of spontaneous rupture, underscoring the role of ischemic degeneration in the pathogenesis of this injury.
Biomechanically, the quadriceps tendon is subjected to immense functional loads. Rupture typically ensues secondary to a violent eccentric contraction of the quadriceps muscle against a suddenly applied physiological load—most classically described as a rapid deceleration event with the foot firmly planted and the knee in a flexed position. The structural integrity of the extensor mechanism is highly dependent on the medial and lateral retinacula. If the retinacula remain intact despite a central tendon rupture, the patient may retain a weak ability to actively extend the knee, which frequently confounds the initial clinical assessment and contributes to the delayed diagnosis of chronic ruptures.
Indications and Contraindications
The management of quadriceps tendon ruptures is largely dictated by the degree of extensor mechanism disruption and the chronicity of the injury. Surgical intervention is the gold standard for complete ruptures to restore the continuity of the extensor mechanism and normal knee kinematics. Chronic ruptures invariably require surgical reconstruction, as non-operative management uniformly results in persistent extensor lag, profound functional disability, and progressive joint contracture.
Operative vs Non Operative Management Parameters
| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Complete Rupture (Acute or Chronic) | Operative Reconstruction | Mandatory to restore active knee extension. Chronic cases require tissue mobilization, V-Y advancement, or allograft augmentation due to tendon retraction and fibrosis. |
| Partial Rupture (Intact Retinacula, No Extensor Lag) | Non-Operative | Immobilization in full extension for 4-6 weeks. Serial clinical exams required to ensure no progression to complete rupture. |
| Severe Medical Comorbidities | Non-Operative | Patients deemed unfit for anesthesia or with limited baseline ambulatory status may be managed with permanent bracing (e.g., drop-lock knee brace). |
| Active Joint Infection | Contraindicated (Temporary) | Eradication of infection via serial debridement and targeted antimicrobial therapy is required prior to definitive extensor mechanism reconstruction. |
| Severe Soft Tissue Compromise | Staged Intervention | Overlying soft tissue defects or active cellulitis must be addressed (potentially requiring plastic surgery consultation for flap coverage) before tendon repair. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical, particularly in chronic settings where tendon retraction and poor tissue quality are anticipated. Diagnostic imaging begins with orthogonal plain radiographs. The lateral view is particularly high-yield, often demonstrating a loss of the normal quadriceps tendon shadow, bony avulsion fragments proximal to the patella, and patella baja secondary to the unopposed distal pull of the patellar tendon over time.

Magnetic Resonance Imaging (MRI) is the gold standard for evaluating chronic ruptures. MRI accurately quantifies the gap distance between the retracted tendon stump and the superior pole of the patella, assesses the degree of fatty infiltration and atrophy within the quadriceps muscle belly, and evaluates the integrity of the medial and lateral retinacula. This imaging modality allows the surgeon to preoperatively determine the necessity for local tissue flaps (e.g., Scuderi turndown, Codivilla V-Y advancement) or the requirement for allograft tissue (e.g., Achilles tendon allograft, extensor mechanism allograft).
Patient Positioning and Operating Room Setup
The patient is positioned supine on a radiolucent operating table to facilitate intraoperative fluoroscopy if necessary. A proximal thigh tourniquet is applied to ensure a bloodless surgical field, which is essential for identifying anatomic planes in the setting of chronic scar tissue.
The sterile prep and drape must be extensile, allowing access from the proximal thigh to the mid-tibia. If autograft harvest (e.g., semitendinosus) is planned for augmentation, the ipsilateral leg must be prepped accordingly. The contralateral leg should be padded and secured. A sterile bump or a triangular positioning foam is often utilized to maintain the knee in approximately 30 to 45 degrees of flexion during the initial exposure and debridement phases.
Detailed Surgical Approach and Technique
The surgical reconstruction of a chronic quadriceps tendon rupture is a demanding procedure that requires meticulous dissection, extensive soft tissue mobilization, and robust fixation constructs to withstand the formidable forces generated by the extensor mechanism.
Incision and Extensile Exposure
A longitudinal midline incision is utilized, typically extending from 10 cm proximal to the superior pole of the patella down to the tibial tubercle. In chronic cases, the incision may need to be extended further proximally to facilitate V-Y advancement or extensive mobilization of the quadriceps muscle belly.
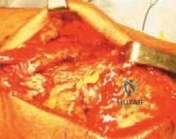
Full-thickness fasciocutaneous flaps are elevated medially and laterally to expose the extensor mechanism. It is imperative to maintain thick flaps to preserve the subdermal vascular plexus and prevent postoperative wound necrosis, a catastrophic complication in this setting. Upon exposure, the surgeon will typically encounter a dense envelope of fibrotic scar tissue bridging the gap between the retracted quadriceps tendon and the patella.

Tendon Mobilization and Debridement
The chronic scar tissue must be systematically excised to identify the true, healthy margins of the native quadriceps tendon proximally and the superior pole of the patella distally. The tendon edges are sharply debrided back to healthy, bleeding tissue. Because chronic ruptures result in significant tendon retraction, extensive mobilization of the quadriceps muscle is mandatory.
Mobilization is achieved by bluntly and sharply elevating the quadriceps muscle off the anterior femur. The suprapatellar pouch is often obliterated in chronic cases and must be meticulously recreated. Adhesions in the medial and lateral gutters must be released. The surgeon should apply distal traction to the tendon stump using a heavy grasping clamp (e.g., a Kocher clamp) to assess the remaining gap with the knee in full extension. If the tendon can be opposed to the patella without excessive tension, primary repair with or without local augmentation may proceed. If a gap persists, advanced lengthening techniques are required.
Primary Repair and Fixation Strategies
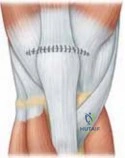
When adequate length is achieved, the tendon is prepared for reattachment to the patella. Two primary fixation techniques are utilized: transosseous tunnels and suture anchors. Biomechanical studies have demonstrated comparable ultimate failure loads between the two techniques, though suture anchors may experience less cyclic displacement.

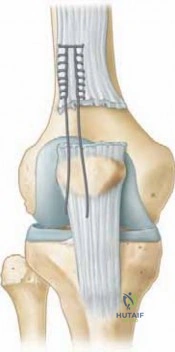
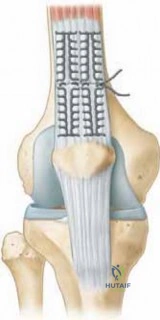
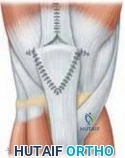
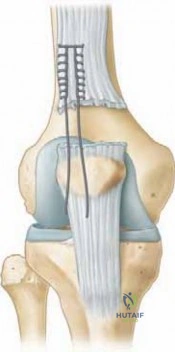
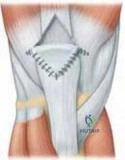
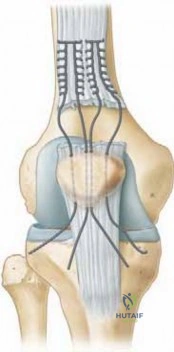
For the transosseous technique, the superior pole of the patella is decorticated with a rongeur or burr to expose a bleeding cancellous bone bed, promoting biologic healing. Three parallel longitudinal tunnels (typically 2.0 to 2.5 mm in diameter) are drilled from the superior pole to the inferior pole of the patella.

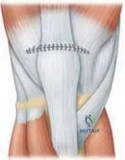
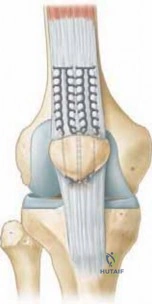
Heavy, non-absorbable sutures (e.g., #2 or #5 FiberWire or Ethibond) are woven through the proximal tendon stump using a locked Krackow or Bunnell configuration. Typically, two to three separate suture strands are utilized. The free ends of the sutures are then passed through the transosseous tunnels using a suture passer or Beath pin.
Alternatively, in the suture anchor technique, two to three biocomposite or titanium anchors are placed into the decorticated superior pole of the patella. The attached sutures are similarly woven through the tendon using locking stitches.
Augmentation Strategies for Chronic Retracted Ruptures
In chronic cases where a gap persists despite extensive mobilization, augmentation or lengthening procedures are required.
Codivilla V Y Advancement
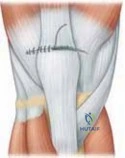
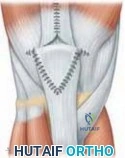
The Codivilla V-Y quadricepsplasty is a classic technique for gaining length. An inverted "V" incision is made through the full thickness of the rectus femoris tendon and fascia, with the apex located 10 to 15 cm proximal to the rupture site. The limbs of the "V" extend distally to the medial and lateral borders of the tendon stump. The tendon is then advanced distally, converting the "V" into a "Y" upon closure. This technique can reliably provide 2 to 4 cm of additional length.

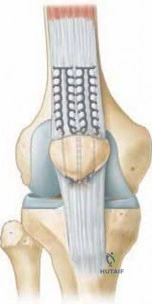
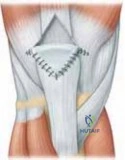
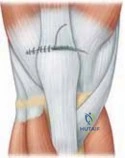
Scuderi Turndown Flap
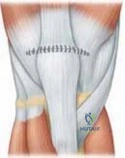
For smaller gaps or to reinforce a tenuous primary repair, a Scuderi turndown flap may be employed. A partial-thickness, distally based triangular flap is elevated from the anterior aspect of the proximal quadriceps tendon. The flap is folded distally over the repair site and sutured to the patella and surrounding retinaculum, providing a biologic overlay that reinforces the repair site.
Allograft Reconstruction
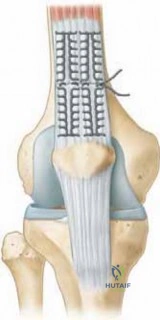
In cases of massive retraction or catastrophic tissue loss, structural allograft reconstruction is indicated. An Achilles tendon allograft with an attached calcaneal bone block is frequently utilized.

The calcaneal bone block is contoured to fit into a precisely created trough in the anterior aspect of the patella and secured with compression screws. The tendinous portion of the Achilles allograft is then woven through and sutured over the remaining native quadriceps muscle and tendon proximally. Synthetic meshes (e.g., Marlex) have also been described as augmentation devices, acting as a scaffold for fibrous tissue ingrowth.

Retinacular Repair and Closure
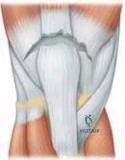
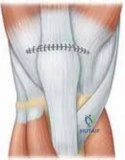
Regardless of the central fixation technique, meticulous repair of the medial and lateral retinacula is absolutely critical. The retinacula contribute significantly to the overall strength of the extensor mechanism and are vital for proper patellar tracking. The retinacular tears are repaired using heavy absorbable or non-absorbable sutures.
The central repair sutures (transosseous or anchors) are tied with the knee in full extension to minimize tension on the repair. The surgeon must then carefully assess the repair construct by ranging the knee. In chronic reconstructions, it is common to limit intraoperative flexion to 30 to 45 degrees to avoid excessive tension and catastrophic failure of the repair. The wound is closed in layers over a closed suction drain to prevent hematoma formation.
Complications and Management
The surgical management of chronic quadriceps tendon ruptures carries a higher complication profile compared to acute repairs, primarily due to the requisite extensive soft tissue dissection, poor baseline tissue quality, and the necessity for prolonged postoperative immobilization.
Arthrofibrosis and profound knee stiffness are the most common complications following chronic reconstruction. The delicate balance between protecting the tenuous repair and initiating early range of motion is difficult to achieve.
Infection and wound healing complications are particularly devastating given the subcutaneous nature of the extensor mechanism. Deep infections may necessitate serial debridements, removal of non-absorbable sutures or allograft material, and prolonged intravenous antibiotics, often resulting in a permanently compromised functional outcome.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Management and Salvage Strategy |
|---|---|---|
| Arthrofibrosis / Stiffness | 15% - 25% | Aggressive physical therapy. Manipulation under anesthesia (MUA) is generally contraindicated due to rupture risk. Arthroscopic or open lysis of adhesions may be considered >6 months post-op. |
| Re-Rupture | 2% - 5% | Requires revision open reconstruction. Typically necessitates structural allograft (Achilles tendon) or synthetic mesh augmentation due to depleted host tissue. |
| Superficial Wound Infection | 3% - 8% | Oral or IV antibiotics based on cultures. Local wound care. Close monitoring to ensure no deep space involvement. |
| Deep Joint Space Infection | < 2% | Emergent operative irrigation and debridement. Retention of hardware/sutures if acutely infected, but late infections may require complete removal of foreign material. |
| Persistent Extensor Lag | 10% - 20% | Often secondary to irreversible muscle atrophy or elongation of the repair. Managed with intensive quadriceps strengthening. Rarely requires revision shortening. |
| Symptomatic Hardware | 5% - 10% | Prominent transosseous knots or anchor pullout. Managed with localized hardware removal after complete biologic healing is confirmed (>6-12 months). |
Post Operative Rehabilitation Protocols
Rehabilitation following the reconstruction of a chronic quadriceps tendon rupture must be highly individualized, conservative, and strictly supervised. The protocol is inherently slower than that of an acute repair due to the extensive tissue mobilization and reliance on augmentation techniques.
Phase One Immediate Post Operative Period
For the first 2 to 4 weeks, the knee is locked in full extension in a hinged knee brace or cylinder cast. Weight-bearing status is typically restricted to touch-down or partial weight-bearing with crutches to minimize reflexive quadriceps contraction. Isometric quadriceps sets, straight leg raises (if cleared by the surgeon), and ankle pumps are initiated immediately to prevent profound atrophy and deep vein thrombosis.
Phase Two Early Protected Range of Motion
Between weeks 4 and 8, progressive, protected range of motion is initiated. The brace is unlocked to allow passive and active-assisted flexion, typically starting from 0 to 30 degrees and advancing by 10 to 15 degrees weekly. Active knee extension is strictly prohibited during this phase to protect the healing tendon-to-bone interface. Weight-bearing is progressively advanced to full as tolerated with the brace locked in extension.
Phase Three Strengthening and Weaning
From weeks 8 to 12, the goal is to achieve 90 to 120 degrees of flexion. Active knee extension exercises are gradually introduced, initially in a closed-kinetic-chain fashion (e.g., leg presses with light resistance) to minimize shear forces across the repair. The hinged knee brace is progressively weaned as the patient demonstrates adequate quadriceps control and no extensor lag during straight leg raises.
Phase Four Advanced Rehabilitation and Return to Function
Beyond 3 to 4 months, therapy focuses on functional strengthening, proprioception, and endurance. Open-kinetic-chain extension exercises may be cautiously introduced. Return to strenuous manual labor or low-impact sports is typically delayed until 6 to 9 months postoperatively, contingent upon the recovery of at least 85% of the contralateral extremity's quadriceps strength as measured by isokinetic testing.
Summary of Key Literature and Guidelines
The academic literature regarding chronic quadriceps tendon ruptures emphasizes the necessity of robust fixation and the frequent need for tissue augmentation.
Classic biomechanical studies by Sherman et al. and more recent investigations evaluating suture anchors versus transosseous tunnels have established that while both constructs provide adequate initial fixation strength (failing at approximately 300-400 Newtons), suture anchors may offer superior cyclic loading characteristics and a reduced risk of suture cutout at the bony interface. However, transosseous tunnels remain the historical gold standard and provide an excellent surface area for biologic integration.
Clinical outcome studies, such as those detailing the Scuderi turndown and Codivilla V-Y advancement, demonstrate that while functional range of motion and active extension can be reliably restored, patients universally experience some degree of permanent quadriceps weakness and atrophy compared to the uninjured limb.
For massive chronic defects, the utilization of Achilles tendon allografts, as described by DeOrio and others, has shown favorable mid-to-long-term survivorship. The literature strongly cautions against over-tensioning the extensor mechanism during chronic reconstruction, as the resultant patellofemoral compressive forces can lead to severe anterior knee pain, accelerated chondrolysis, and profound arthrofibrosis. Consequently, modern surgical guidelines advocate for accepting a mild, functional extensor lag in favor of preserving joint kinematics and achieving a stable, healed construct.
Clinical & Radiographic Imaging