Quadriceps Tendon Repair: An Intraoperative Masterclass for Acute & Chronic Ruptures
Key Takeaway
This masterclass guides fellows through the meticulous repair of quadriceps tendon ruptures, from acute avulsions to chronic, retracted tears. We cover detailed surgical anatomy, patient positioning, and step-by-step intraoperative execution for both tendon-bone interface and mid-substance repairs. Learn advanced suturing techniques, augmentation strategies, and critical pearls to avoid complications, ensuring optimal patient outcomes and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
A quadriceps tendon rupture represents a catastrophic disruption of the knee’s extensor mechanism, an injury that demands immediate and meticulous surgical intervention. This debilitating condition, if mismanaged or subjected to delayed diagnosis, inevitably leads to profound long-term disability, characterized by an intractable extensor lag, severe quadriceps atrophy, and altered joint biomechanics. The primary surgical objective is the anatomic restoration of the extensor mechanism, re-establishing the critical linkage between the quadriceps musculature and the patella to allow the patient to regain full functional ambulation and dynamic knee stability.
While these ruptures are frequently precipitated by a sudden, eccentric load applied to a flexed knee—such as a stumble on a stair or an abrupt deceleration—the orthopedic surgeon must maintain a high index of suspicion for predisposing systemic factors. Healthy, native tendons rarely rupture under normal physiologic loads; thus, underlying tendinopathy or systemic compromise is almost universally present. Conditions such as gout, pseudogout, systemic lupus erythematosus (SLE), end-stage renal disease, hyperparathyroidism, and poorly controlled diabetes mellitus induce microvascular compromise and alter collagen cross-linking, rendering the tendon structurally friable. Furthermore, iatrogenic and pharmacological factors play a significant role. Chronic corticosteroid use induces collagen necrosis, while fluoroquinolone antibiotics (e.g., ciprofloxacin) have been shown to upregulate matrix metalloproteinases (MMPs) and inhibit tenocyte proliferation, leading to acute tendon fragility.
Epidemiologically, the typical patient presenting with a quadriceps tendon rupture is a male over the age of 40, reflecting the intersection of age-related tendon degeneration and maintained physical activity levels. While unilateral ruptures constitute the vast majority of presentations, the occurrence of a simultaneous bilateral quadriceps tendon rupture is a pathognomonic red flag for a severe underlying systemic medical condition or profound metabolic derangement. Anatomically, the most common site of failure is an avulsion or transverse tear occurring through a pathologic, hypovascular zone located approximately 1 to 2 cm proximal to the superior pole of the patella. Depending on the magnitude and duration of the disruptive force, the tear frequently propagates obliquely into the medial and lateral retinacula, effectively eliminating any residual extensor capacity.
The natural history of an unrepaired or neglected quadriceps tendon rupture is universally poor. The unopposed pull of the rectus femoris and vastus musculature leads to progressive, irreversible proximal retraction and dense intramuscular fibrosis. Concurrently, the patella, deprived of its superior tether, migrates distally, resulting in a fixed patella baja. Clinically, patients present with an acute history of a distinct "pop" or tearing sensation, followed immediately by severe pain, massive hemarthrosis, and an inability to bear weight. The hallmark physical examination finding—and the sine qua non of extensor mechanism disruption—is the inability to perform an active straight leg raise (SLR) or maintain the knee in active extension against gravity. The clinician must palpate carefully for the characteristic suprapatellar gap, being mindful that intact medial and lateral retinacula can occasionally mask the defect and provide a deceptive, weak degree of active extension.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the intricate, multi-layered anatomy of the quadriceps tendon is an absolute prerequisite for successful surgical reconstruction. The quadriceps femoris is a massive, powerful muscle group composed of four distinct bellies that coalesce approximately 3 to 5 cm proximal to the superior pole of the patella to form the common quadriceps tendon. The rectus femoris, the most superficial and the only biarticular muscle of the group, originates from the anterior inferior iliac spine (AIIS) and the superior acetabular rim. Its posterior fascial envelope continues distally to form the robust superficial layer of the quadriceps tendon.
Deep to the rectus femoris lie the vastus medialis and vastus lateralis. The vastus medialis originates from the intertrochanteric line and the medial lip of the linea aspera, while the vastus lateralis arises from the greater trochanter and the lateral lip of the linea aspera. The fascial extensions of these two muscles merge to form the middle layer of the quadriceps tendon. The deepest muscle, the vastus intermedius, originates from the anterior and lateral surfaces of the femoral shaft; its anterior aponeurosis constitutes the deep layer of the tendon. Consequently, the quadriceps tendon is a trilaminar structure, averaging 8 mm in anteroposterior thickness and 35 mm in mediolateral width at its insertion point on the superior patellar pole. The patella functions as an embedded sesamoid bone, acting as a critical mechanical fulcrum that displaces the tendon anteriorly away from the center of rotation of the knee, thereby significantly increasing the moment arm and mechanical advantage of the quadriceps mechanism.
Neurovascular considerations during surgical dissection are paramount to prevent iatrogenic morbidity. The primary motor innervation to the quadriceps musculature is derived from the femoral nerve, which branches extensively in the proximal thigh. However, the terminal sensory branches, specifically the saphenous nerve and its infrapatellar branch, are highly vulnerable during surgical exposure. The saphenous nerve exits the adductor canal and courses superficially along the medial aspect of the knee; extensive medial dissection or aberrant incision placement can result in painful neuromas or medial sensory loss.
The vascular supply to the quadriceps tendon is complex and highly relevant to its rupture pathophysiology. The tendon receives arterial contributions from the descending branch of the lateral circumflex femoral artery, the descending geniculate artery, and the medial and lateral superior geniculate arteries. Crucially, the vascular distribution is asymmetric. While the superficial and middle layers maintain a relatively robust blood supply from the musculotendinous junction down to the patellar insertion, the deep layer (derived from the vastus intermedius) contains a well-documented oval avascular zone located 1 to 2 cm proximal to the patella. This watershed area is highly susceptible to degenerative tendinosis, mucoid degeneration, and subsequent mechanical failure, explaining why the majority of ruptures initiate in this specific anatomic location.
Exhaustive Indications and Contraindications
The decision to proceed with operative management of a quadriceps tendon rupture is generally straightforward, as the functional consequences of non-operative management are severe. However, patient selection, timing of surgery, and recognition of absolute and relative contraindications are critical for optimizing outcomes and minimizing perioperative morbidity.
Surgical repair is the definitive gold standard for all complete, acute quadriceps tendon ruptures in ambulatory patients. Immediate or early repair (within 2 to 3 weeks of injury) is highly recommended to avoid tendon retraction, muscle atrophy, and the development of dense scar tissue, which significantly complicate delayed reconstructions. Partial ruptures present a more nuanced clinical scenario. If a partial rupture is associated with an intact active straight leg raise and minimal extensor lag (less than 5 to 10 degrees), a trial of conservative management utilizing a locked knee immobilizer or hinged brace in extension for 4 to 6 weeks may be appropriate. However, if a partial rupture fails conservative management, or if the patient presents with a significant, functionally limiting extensor lag, surgical repair is indicated.
Contraindications to surgical intervention are primarily dictated by the patient's overall physiological status and baseline functional capacity. Absolute contraindications include the presence of an active, untreated local or systemic infection, or a patient who is medically unstable and cannot safely tolerate general or regional anesthesia. Relative contraindications require careful, individualized risk-benefit analysis. Patients with profound, pre-existing cognitive impairment (e.g., advanced dementia) who cannot comply with strict postoperative weight-bearing and immobilization protocols are at an exceptionally high risk for early failure and re-rupture. Similarly, patients who were strictly non-ambulatory prior to the injury may not benefit from the physiological stress of a major reconstructive procedure.
| Clinical Parameter | Indications for Surgical Repair | Contraindications for Surgical Repair |
|---|---|---|
| Complete Rupture | Acute or chronic setting in any ambulatory patient. | Non-ambulatory baseline status (Relative). |
| Partial Rupture | Extensor lag > 10-15 degrees; Failure of conservative management. | Intact SLR; Extensor lag < 5 degrees; Asymptomatic. |
| Patient Physiology | Medically optimized; Compliant with rehabilitation. | Medically unstable for anesthesia (Absolute). |
| Local Tissue Status | Intact or manageable soft tissue envelope. | Active local soft tissue infection or cellulitis (Absolute). |
| Cognitive Status | Ability to follow strict post-op protocols. | Severe dementia; Inability to comply with rehab (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a successful quadriceps tendon repair. The clinical diagnosis must be corroborated and precisely defined by advanced imaging modalities. Magnetic Resonance Imaging (MRI) remains the gold standard, providing exquisite, multi-planar detail regarding the tear morphology. The surgeon must meticulously analyze the MRI to determine the exact location of the rupture (e.g., avulsion at the bone-tendon interface, mid-substance tear, or musculotendinous junction disruption), the degree of proximal tendon retraction, and the quality of the residual tendon tissue. MRI is also invaluable for identifying pre-existing pathology, such as severe tendinosis or mucoid degeneration, which may necessitate more extensive debridement and augmentation techniques.
While MRI is definitive, plain radiography is a mandatory initial step. Standard anteroposterior (AP) and lateral views of the knee should be scrutinized. The lateral radiograph may reveal a bony avulsion fracture from the superior pole of the patella, chronic calcific tendinopathy, or an altered Insall-Salvati ratio indicative of patella baja (in chronic cases) or patella alta (if the patellar tendon is concurrently injured). A Merchant's or sunrise view may demonstrate the "tooth sign"—vertical ridging of osteophytes at the anterior patellar attachment—which is highly suggestive of chronic, degenerative enthesopathy. In cases of chronic, neglected ruptures, the surgeon must anticipate significant tendon retraction and quadriceps fibrosis; thus, preoperative consent and planning must include the potential need for complex lengthening procedures (e.g., Codivilla V-Y advancement) or fascial/allograft augmentation (e.g., Scuderi flap).
Patient positioning in the operating room must be executed with precision to facilitate optimal surgical exposure and allow for dynamic intraoperative assessment of the repair. The patient is positioned supine on a standard radiolucent operating table. All bony prominences, particularly the heels, sacrum, and contralateral common peroneal nerve at the fibular head, must be meticulously padded to prevent pressure-induced neurapraxia or decubitus ulcers. A non-sterile tourniquet is applied high on the proximal thigh of the operative leg.
A critical positioning maneuver is the placement of a bump or sandbag under the ipsilateral gluteal region. This serves to internally rotate the leg slightly, neutralizing the natural tendency of the lower extremity to externally rotate when relaxed, thereby ensuring the patella faces directly anteriorly. The operative leg is then systematically prepped and draped free, allowing for unrestricted, full range of motion of the knee joint throughout the procedure. This mobility is absolutely vital; the surgeon must be able to flex the knee intraoperatively to assess the tension of the repair, confirm the security of the fixation, and determine the safe postoperative range of motion limits.
Step-by-Step Surgical Approach and Fixation Technique
Approach and Initial Dissection
The surgical procedure commences with the inflation of the proximal thigh tourniquet, following exsanguination of the limb, to provide a bloodless surgical field. A straight, 10-cm midline longitudinal incision is planned, perfectly centered over the palpable defect at the superior pole of the patella.

This extensile midline approach is preferred over transverse incisions as it preserves the vascular supply to the skin flaps, allows for proximal or distal extension if necessary, and provides unparalleled access to both the medial and lateral retinacular expansions. The skin and subcutaneous tissues are sharply incised down to the level of the deep fascia. Meticulous hemostasis is maintained using electrocautery. As the dissection deepens, the surgeon must remain vigilant to identify and protect any superficial sensory nerve branches, particularly the infrapatellar branch of the saphenous nerve, which may cross the operative field distally and medially.
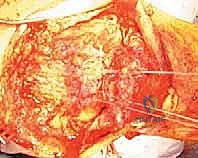
Upon incising the deep fascial layer longitudinally, the catastrophic nature of the injury becomes immediately apparent. In the acute setting, the surgeon will encounter a massive, organized fracture hematoma filling the suprapatellar pouch and the defect between the retracted tendon and the patella.

This hematoma must be aggressively evacuated using a combination of blunt dissection, suction, and copious pulsed lavage. Clearing this debris is essential to accurately visualize the torn tendon ends, assess the degree of retraction, and evaluate the articular surface of the patellofemoral joint for any concomitant chondral injury.
Once the field is cleared, the superficial layers are carefully retracted to expose the deeper tissue planes. The surgeon must systematically evaluate the integrity of the medial and lateral retinacula. These robust fascial expansions are critical secondary stabilizers of the patella, and their disruption significantly compromises the extensor mechanism.

With the patella gently retracted inferiorly using a bone hook or towel clip, the full transverse extent of the quadriceps tendon tear is clearly demonstrated.

To assess the mobility and quality of the proximal stump, the superficial and deep layers of the retracted quadriceps tendon are grasped securely with multiple Allis or Kocher clamps. Gentle, sustained distal traction is applied to overcome the initial muscle spasm and evaluate whether the tendon can be reapproximated to the superior pole of the patella without excessive, unphysiologic tension.

Tendon Preparation and Debridement
The foundation of a robust, biologically sound repair is the meticulous preparation of both the tendon stump and the bony insertion site. The proximal tendon stump is often frayed, disorganized, and infiltrated with necrotic, mucoid-degenerated tissue. Using a fresh #10 scalpel blade or heavy Mayo scissors, the surgeon must sharply debride the tendon edge, excising all non-viable, degenerative tissue until healthy, organized, glistening white collagen fibers are encountered.

Failure to adequately debride the tendon will result in sutures pulling through friable tissue, leading to catastrophic early failure of the repair. Once debrided, the tendon edge is squared off to maximize the surface area for bone-to-tendon healing.
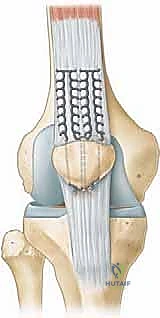
With the tendon prepared, heavy, non-absorbable, braided sutures (e.g., #2 or #5 FiberWire or Ethibond) are systematically woven through the proximal stump. The Krackow locking stitch technique is universally recognized as the biomechanically superior method for securing the tendon. The surgeon places two or three parallel rows of Krackow stitches, starting 2 to 3 cm proximal to the rupture edge and working distally, ensuring that each locking loop securely grasps a substantial bite of healthy tendon.

The free ends of the sutures are carefully managed, clamped with hemostats, and organized to prevent tangling during the subsequent passage through the patella.

Patellar Preparation and Suture Management
Attention is then directed to the superior pole of the patella. To stimulate a robust healing response and provide a vascularized bed for the tendon to incorporate, the superior pole is decorticated. Using a rongeur or a high-speed burr, a transverse bony trough, approximately 5 mm deep and extending the width of the patella, is created at the exact anatomic footprint of the quadriceps tendon.
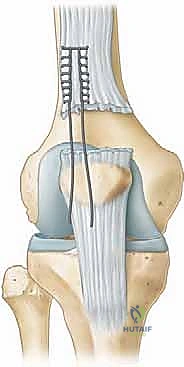
The traditional, time-tested method of fixation utilizes transosseous tunnels. Using a 2.0 mm or 2.5 mm drill bit, three parallel longitudinal tunnels are drilled from the depths of the prepared superior trough, exiting distally at the inferior pole of the patella, taking care to remain extra-articular (anterior to the articular cartilage).

Alternatively, modern techniques utilize double-loaded suture anchors placed directly into the superior pole, which provide equivalent biomechanical strength and eliminate the need for transosseous drilling, potentially reducing the risk of iatrogenic patellar fracture. If transosseous tunnels are utilized, a suture passer or a Hewson slider is used to shuttle the heavy free ends of the Krackow sutures through the bony tunnels. The central sutures share the middle tunnel, while the medial and lateral sutures pass through their respective peripheral tunnels.

Tensioning, Fixation, and Retinacular Repair
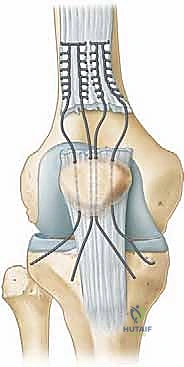
Tensioning the repair is a critical step that requires precise coordination. The knee is positioned in full extension (0 degrees). The surgeon applies firm, distal traction on the sutures exiting the inferior pole of the patella, drawing the prepared tendon stump deeply into the bleeding bony trough.
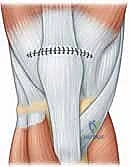
While maintaining this tension, the sutures are tied securely over the bony bridge at the inferior pole. It is imperative that the knots are buried deep within the soft tissue to prevent painful hardware prominence postoperatively.


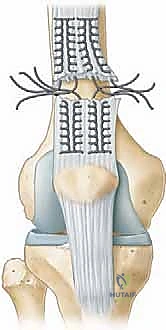
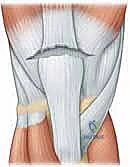
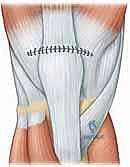
Once the primary tendon-to-bone fixation is secure, the surgeon must meticulously repair the medial and lateral retinacular tears. Using #1 or #0 absorbable sutures (e.g., Vicryl), the retinacula are repaired in an interrupted fashion, ensuring a watertight closure of the joint capsule and restoring the dynamic mediolateral stability of the patella.


With the repair complete, the most crucial intraoperative test is performed. The surgeon carefully and slowly flexes the knee while directly visualizing the repair site. The knee should comfortably reach 90 degrees of flexion without excessive gapping at the bone-tendon interface. This determines the safe zone for postoperative rehabilitation.

The wound is then thoroughly irrigated. The subcutaneous tissue is closed in layers to eliminate dead space, and the skin is approximated using staples or a subcuticular closure.
The limb is immediately placed in a well-padded, sterile dressing and secured in a locked hinged knee brace or a rigid cylinder cast in full extension.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following quadriceps tendon repair can be devastating and profoundly alter the patient's functional trajectory. The most catastrophic complication is re-rupture, which typically occurs within the first 6 to 12 weeks postoperatively, often due to patient non-compliance with weight-bearing restrictions or an aggressive, premature return to deep flexion activities. Re-rupture necessitates a highly complex revision surgery, frequently requiring allograft augmentation (e.g., Achilles tendon allograft with a bone block) due to severe tissue compromise and retraction.
Arthrofibrosis and profound knee stiffness represent the most common complications, arising from prolonged immobilization and dense intra-articular scar formation. Patients may struggle to regain flexion past 90 degrees. If aggressive physical therapy fails to restore motion by 3 to 4 months postoperatively, a manipulation under anesthesia (MUA) or arthroscopic lysis of adhesions may be indicated, though these procedures carry a secondary risk of iatrogenic tendon rupture. Deep surgical site infections are rare but limb-threatening, requiring emergent surgical debridement, copious irrigation, and prolonged culture-directed intravenous antibiotic therapy.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Re-Rupture | 2% - 5% | Non-compliance; Poor tissue quality; Premature flexion. | Revision repair with allograft augmentation; V-Y lengthening. |
| Arthrofibrosis (Stiffness) | 10% - 15% | Prolonged immobilization; Inadequate physical therapy. | Aggressive PT; Manipulation Under Anesthesia (MUA); Arthroscopic lysis. |
| Deep Infection | 1% - 2% | Diabetes; Obesity; Immunocompromise; Prolonged OR time. | Emergent I&D; IV Antibiotics; Retention of hardware if stable. |
| Symptomatic Hardware | 5% - 10% | Prominent transosseous knots at inferior patellar pole. | Minor outpatient procedure for knot excision/hardware removal after healing. |
| Patella Baja | 5% - 8% | Over-tensioning of repair; Chronic, delayed reconstruction. | Often tolerated; Severe cases may require tibial tubercle osteotomy (TTO). |
Phased Post-Operative Rehabilitation Protocols
The success of a quadriceps tendon repair is inextricably linked to a rigid, highly structured, phased postoperative rehabilitation protocol. The delicate balance between protecting the healing tendon from excessive tensile loads and preventing debilitating arthrofibrosis requires constant communication between the surgeon and the physical therapist.
Phase I: Maximum Protection (Weeks 0 to 2)
Immediately postoperatively, the knee is locked in full extension (0 degrees) in a hinged knee brace. Weight-bearing status is typically restricted to toe-touch or partial weight-bearing with crutches, primarily
