Operative Management of Tendinitis and Bursitis: A Comprehensive Surgical Guide
Key Takeaway
Tendinitis and bursitis frequently result from repetitive mechanical overload, anatomic malalignment, or inflammatory arthropathies. While conservative modalities like targeted physical therapy, orthotics, and corticosteroid injections resolve most cases, refractory or septic presentations necessitate surgical intervention. Operative management ranges from minimally invasive aspiration to formal open excision and drainage. This guide details the biomechanical principles, diagnostic criteria, and step-by-step surgical techniques required for optimal outcomes in complex bursal and tendinous pathologies.
Comprehensive Introduction and Patho-Epidemiology
In the comprehensive evaluation of patients presenting with tendinitis and bursitis of the lower extremity, a meticulous history detailing occupational demands, biomechanical stressors, and exercise routines is paramount. The etiology of these ubiquitous orthopedic conditions is frequently rooted in mechanical overload, which can be further subdivided into overuse (repetitive, submaximal activity) or acute overload (sudden, unaccustomed increases in activity intensity). These pathological forces induce microtearing within the tendinous architecture, leading to a cascade of mucoid degeneration, neovascularization, and chronic tendinopathy. Unlike acute inflammatory tendinitis, chronic tendinopathy is characterized histologically by angiofibroblastic hyperplasia, an absence of acute inflammatory cells, and a disorganized collagen matrix dominated by inferior Type III collagen rather than the robust Type I collagen found in healthy tendons.
Mechanical abnormalities play a critical and often underappreciated role in the pathogenesis of both tendinous and bursal conditions. Leg-length discrepancies, coronal or sagittal plane malalignment (such as genu varum or genu valgum), and foot pathomechanics (e.g., excessive subtalar pronation, rigid supination, or pes cavus) inextricably alter the kinetic chain. This biomechanical disruption places asymmetrical stress on tendinous insertions and the adjacent bursae designed to protect them. Over time, the physiological capacity of these structures to attenuate friction is overwhelmed, leading to cellular hypertrophy, increased exudative fluid production, and clinical symptomatology.
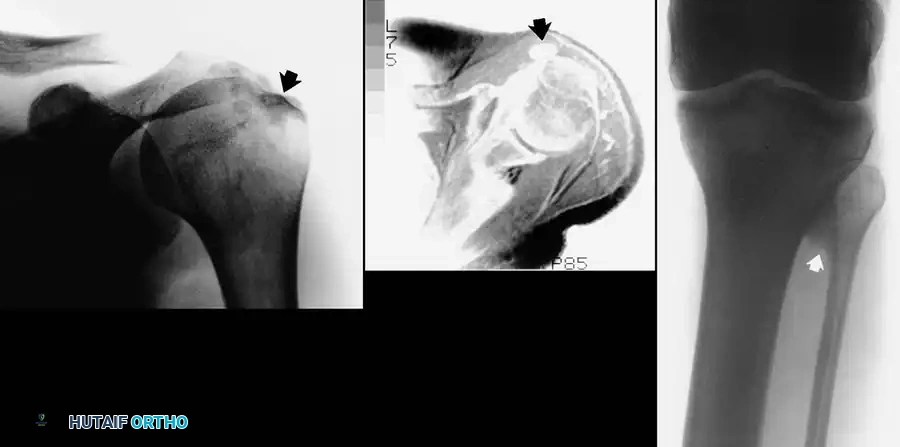
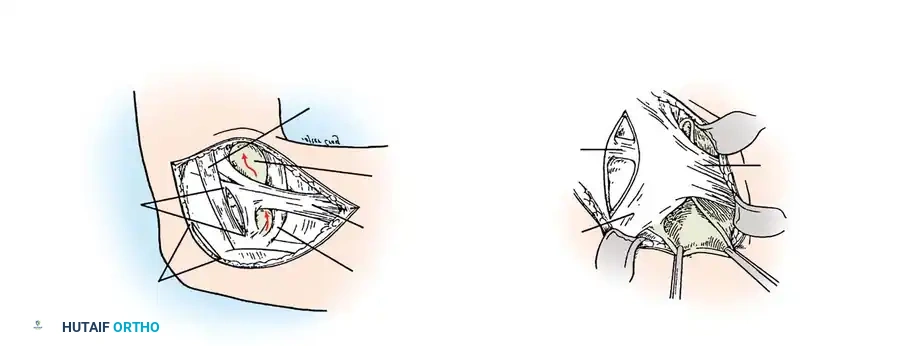
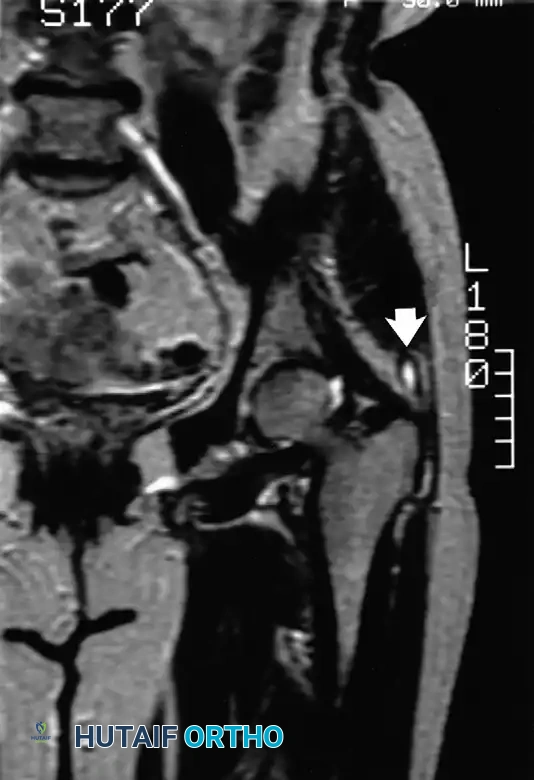
Fig. 24-7: (A) Painful calcification of the anterior deltoid. (B) MRI demonstrating localization of the calcium deposit in the deltoid muscle. (C) Calcification of the proximal tibiofibular articulation resulting in peroneal nerve entrapment in a professional athlete.
While conservative management remains the cornerstone of initial treatment, understanding the epidemiological distribution of these lesions is vital for the practicing orthopedic surgeon. Most cases of aseptic tendinitis and bursitis respond favorably to relative rest, cryotherapy, compressive Neoprene sleeves, nonsteroidal anti-inflammatory drugs (NSAIDs), and ergonomic modifications. Biomechanical deficits must be systematically addressed with properly fitted, custom orthotics to neutralize abnormal foot mechanics. Furthermore, muscular imbalances require targeted physical therapy focusing on eccentric strengthening and dynamic flexibility protocols. However, when the pathological threshold is crossed—resulting in fibrotic thickening, intrabursal loose bodies (rice bodies), or frank suppuration—the disease process transitions from a medically managed inconvenience to a surgically imperative pathology.
The epidemiological profile of bursitis demonstrates a bimodal distribution, heavily influenced by occupational hazards and systemic comorbidities. Traumatic or friction-induced bursitis (e.g., prepatellar bursitis or "housemaid's knee") is predominantly observed in working-age adults whose occupations require prolonged kneeling, such as carpenters, roofers, and plumbers. Conversely, septic bursitis disproportionately affects pediatric populations, immunocompromised adults, and individuals with poorly controlled diabetes mellitus or chronic renal failure. Systemic inflammatory conditions, including gout, pseudogout, and rheumatoid arthritis, further complicate the epidemiological landscape, precipitating acute bursal flares that can perfectly mimic pyogenic infections.
Detailed Surgical Anatomy and Biomechanics
Bursae are specialized, flattened, sac-like structures lined with a synovial-like membrane, strategically located throughout the musculoskeletal system. They are typically found in periarticular regions or where skin, tendon, or muscle glides over a bony prominence. Their primary biomechanical function is to act as biological bearings, attenuating friction and protecting delicate neurovascular and tendinous structures from compressive and shear forces during dynamic joint articulation. The synovial lining of a healthy bursa secretes a highly viscous fluid rich in hyaluronic acid, which provides boundary lubrication and minimizes the coefficient of friction between moving anatomical layers.
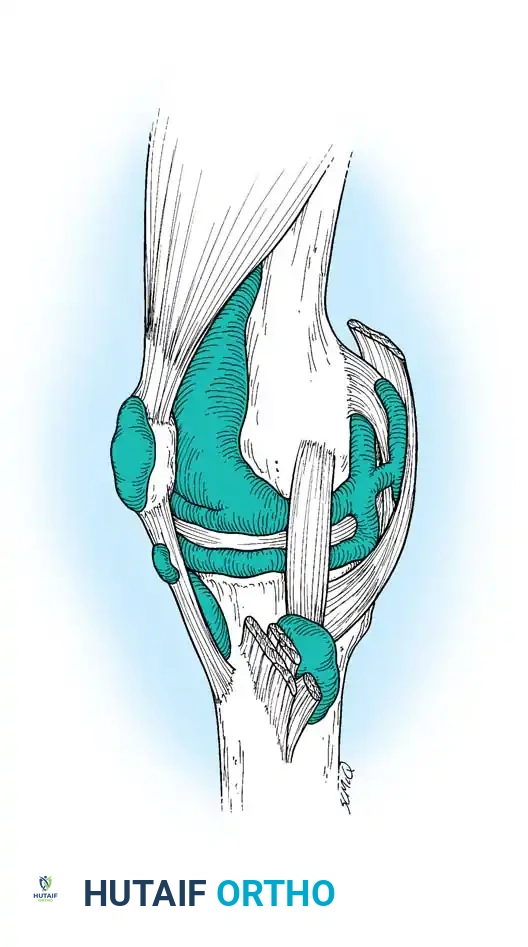
Fig. 24-8: Multiple bursae around the knee that may become acutely or chronically inflamed, including the prepatellar, superficial and deep infrapatellar, and pes anserine bursae.
The human body contains over 140 bursae, which are broadly classified into two distinct pathoanatomic categories: anatomical (innate) bursae and adventitious bursae. Anatomical bursae are naturally occurring structures present from embryological development, such as the prepatellar, olecranon, and trochanteric bursae. These possess a true endothelial and synovial lining capable of massive fluid exudation in response to trauma or infection. In contrast, adventitious bursae are acquired structures that develop strictly in response to chronic, repeated trauma, constant friction, or abnormal pressure over time. Common sites for adventitious bursa formation include the medial eminence of a hallux valgus deformity (bunion), the apex of a severe spinal kyphosis, or overlying a prominent osteochondroma.
Histological studies, notably those by Kuhns, have demonstrated that while adventitious bursae initially lack a true endothelial or synovial lining, they are subject to the identical pathological changes seen in innate bursae. Through chronic mechanical irritation, the surrounding mesenchymal tissue differentiates into a pseudosyovial layer. Because adventitious bursae develop thick, fibrous walls in a relatively avascular subcutaneous bed, they are highly susceptible to chronic inflammatory changes, pyogenic infection, villous hypertrophy, fibrotic thickening, and, rarely, tumorous transformation. The shared histological profiles of bursae and tendon sheaths render them mutually vulnerable to acute or chronic microtrauma, direct inoculation of pyogenic organisms (most commonly Staphylococcus aureus), and systemic inflammatory cascades.
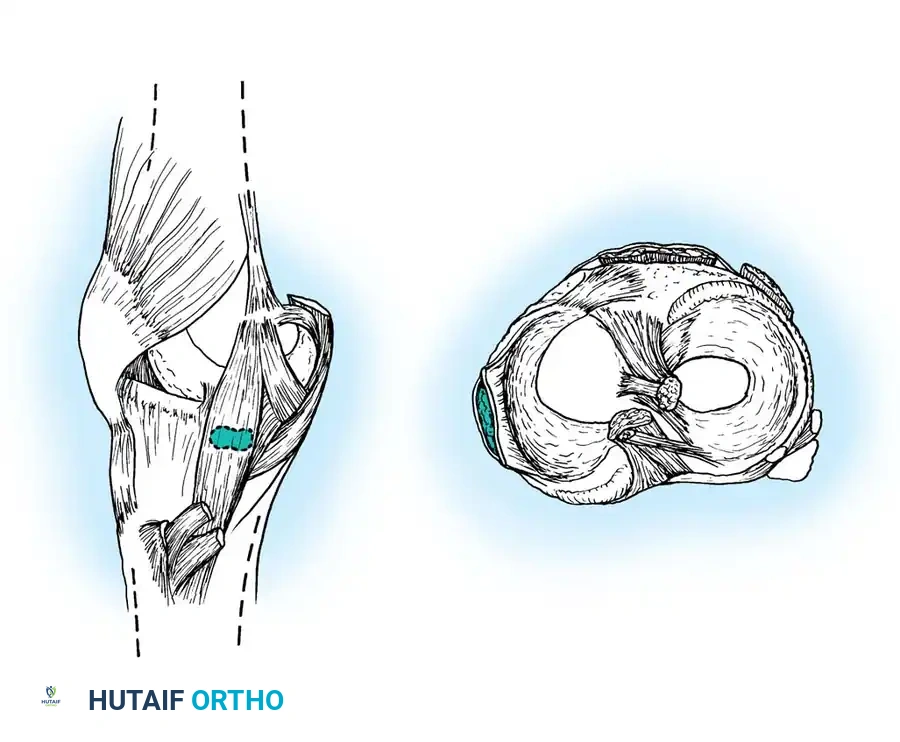
Fig. 24-9: Voshell bursa located just below the joint line, situated between the superficial tibial collateral ligament and the deep joint capsule.
Anatomy of the Knee Bursal Network
The knee joint is surrounded by a complex and highly specialized network of bursae, making it uniquely susceptible to both traumatic and inflammatory bursitis. The prepatellar bursa is a trilaminar structure located anterior to the lower half of the patella and the superior half of the patellar ligament. The superficial infrapatellar bursa lies between the skin and the tibial tubercle, while the deep infrapatellar bursa is situated between the posterior aspect of the patellar tendon and the anterior tibia, separated from the intra-articular synovium by Hoffa's fat pad.
Sagittal representation of the deep infrapatellar bursa and its relationship to the patellar tendon and Hoffa's fat pad.
On the medial aspect of the knee, the pes anserine bursa separates the conjoined tendons of the sartorius, gracilis, and semitendinosus from the underlying medial collateral ligament (MCL) and medial tibial metaphysis. Deep to the MCL, Voshell and Brantigan identified a complex of bursae located between the longitudinal fibers of the superficial MCL and the deep knee capsule. Up to three distinct bursae can exist beneath this ligament, and their distension often mimics medial meniscal pathology. Laterally, the fibular collateral ligament bursa, described by Hendryson, lies beneath, anterior, or posterior to the lateral collateral ligament (LCL), presenting a diagnostic challenge against cysts of the lateral meniscus or biceps femoris tendinopathy.
Anatomical dissection highlighting the lateral ligamentous complex and the typical location of the fibular collateral ligament bursa.
Exhaustive Indications and Contraindications
Surgical intervention for bursitis and tendinitis is dictated primarily by the underlying etiology, the chronicity of the symptoms, and the morphological changes within the bursa or tendon. In the vast majority of cases, surgery is strictly avoided in the acute phase of aseptic inflammation. Systemic drivers, such as inflammatory arthropathies or crystal deposition diseases, must be medically optimized by rheumatology, and local mechanical irritants must be eliminated through orthoses or activity modification. Surgery is reserved for recalcitrant cases that have failed a dedicated, multi-modal nonoperative regimen lasting a minimum of three to six months.
When conservative measures—including prolonged rest, moist heat therapy, protective padding, therapeutic ultrasound, and immobilization—fail to provide durable relief, surgical intervention becomes necessary. Furthermore, the presence of acute suppuration (septic bursitis) drastically alters the treatment algorithm, often necessitating emergent or urgent surgical decompression to prevent contiguous osteomyelitis, skin necrosis, or systemic sepsis. The primary surgical modalities include simple aspiration and injection, formal incision and drainage (I&D), complete bursectomy, and resection of underlying bony prominences that act as mechanical triggers.
The decision to proceed with operative management must carefully weigh the significant risks of wound healing complications, particularly over extensor surfaces like the patella and olecranon, where the skin is thin, mobile, and poorly vascularized. A thorough understanding of the indications and absolute contraindications is essential to prevent catastrophic iatrogenic complications, such as converting a sterile, localized bursitis into a fulminant intra-articular septic arthritis.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Aspiration & Corticosteroid Injection | Acute sterile bursitis; diagnostic fluid analysis; painful calcific tendinitis. | Suspected or confirmed pyogenic infection; overlying cellulitis; intra-tendinous injection (risk of rupture). | Coagulopathy; poorly controlled diabetes (risk of glycemic spike); multiple prior injections. |
| Incision and Drainage (I&D) | Acute suppurative bursitis refractory to 36-48 hours of serial aspiration and IV antibiotics; frank abscess formation. | Sterile, aseptic bursitis (risk of introducing nosocomial infection). | Severe peripheral vascular disease precluding wound healing; uncorrectable coagulopathy. |
| Open Bursectomy (Excision) | Chronic, fibrotic bursitis with painful nodules (rice bodies); recurrent sterile effusions failing conservative care. | Active overlying cellulitis or acute untreated pyogenic infection (unless performing an open, packed procedure). | Inadequate soft tissue envelope for primary closure; non-compliant patient unable to tolerate post-op immobilization. |
| Baker's Cyst Excision (Adults) | Massive, multiloculated cysts causing direct compression of the tibial nerve or popliteal vein; failure of intra-articular management. | Uncorrected intra-articular pathology (e.g., untreated medial meniscus tear or severe OA). | Asymptomatic cysts; cysts in pediatric patients (which typically resolve spontaneously). |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for the surgical management of tendinitis and bursitis begins with a rigorous clinical and radiographic evaluation to definitively rule out intra-articular pathology. The diagnostic warning cannot be overstated: differentiating septic prepatellar bursitis from septic arthritis of the knee is a critical clinical skill. In isolated bursitis, gentle, short-arc joint motion (typically between 15 and 30 degrees of flexion) is relatively painless, as the intra-articular capsule is not under tension. Conversely, in true septic arthritis, any micromotion of the joint elicits severe, intractable pain and involuntary muscular guarding.
Diagnostic imaging is a fundamental component of pre-operative templating. Plain radiography (anteroposterior, lateral, and axial views) is obtained to evaluate for underlying osteophytes, calcific deposits (such as Pellegrini-Stieda lesions near the MCL), or concomitant osteoarthritis. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating refractory cases, delineating the exact anatomical boundaries of the bursa, identifying loculations, and assessing the integrity of adjacent tendons. For example, tibial collateral ligament bursitis presents on MRI with a characteristic fluid signal deep to the MCL, forming an inverted "U" shape that must be differentiated from a parameniscal cyst. Ultrasonography is increasingly utilized as a dynamic, cost-effective adjunct for both diagnosis and ultrasound-guided therapeutic aspiration.
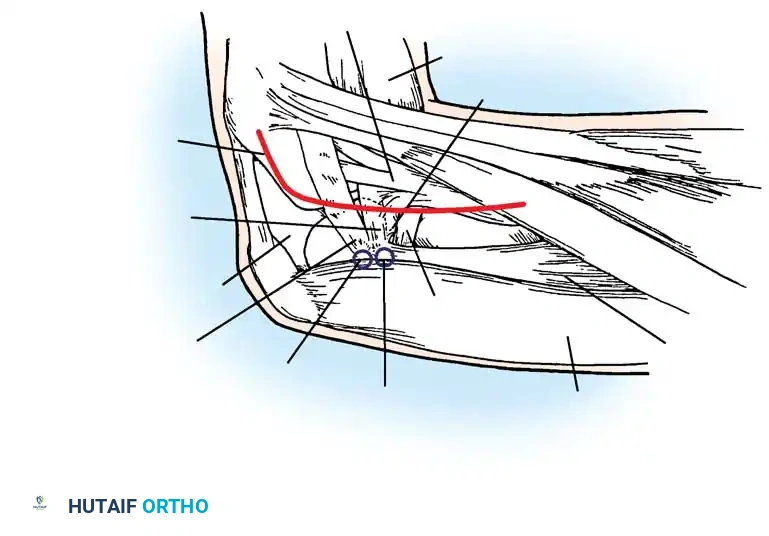
Surgical exposure demonstrating the critical neurovascular boundaries during deep bursal excision.
Laboratory analysis of aspirated bursal fluid is mandatory whenever infection is suspected. Fluid should be sent for cell count with differential, Gram stain, aerobic and anaerobic cultures, acid-fast bacilli (AFB), and crystal analysis under polarized light microscopy. While a synovial white blood cell (WBC) count exceeding 50,000 cells/mm³ is classic for septic arthritis, septic bursitis may present with significantly lower WBC counts; therefore, clinical correlation and Gram stain results are paramount.
Patient positioning is dictated by the specific anatomical location of the pathology. For anterior knee procedures (prepatellar, infrapatellar, pes anserine bursae), the patient is positioned supine on a standard radiolucent operating table. A proximal thigh tourniquet is applied but should only be inflated if visualization is compromised, as tourniquet-induced ischemia can complicate hemostasis during closure. For posterior pathology, such as a complex popliteal (Baker's) cyst excision, the patient is positioned prone. Careful padding of all bony prominences, particularly the contralateral peroneal nerve at the fibular head, is essential. The surgical limb is prepped and draped freely to allow for dynamic manipulation of the joint during the procedure, which aids in identifying capsular communications and assessing the tension on surgical repairs.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention demands meticulous soft tissue handling, precise anatomical dissection, and rigorous dead space management to prevent the high incidence of postoperative hematoma and seroma formation. The surgical approach must be tailored to the specific bursa, respecting the delicate cutaneous vascular supply and the underlying extensor mechanisms.
Surgical Technique: Drainage of Prepatellar Bursa
For acute suppurative prepatellar bursitis failing nonoperative management, formal incision and drainage (I&D) is indicated. The patient is positioned supine, and while a tourniquet may be applied, it is often unnecessary for simple drainage. The approach utilizes either two longitudinal incisions (one medial and one lateral to the fluctuant bursa) or a single transverse incision centered over the mass. Transverse incisions are generally preferred as they parallel the Langer lines of the anterior knee, resulting in superior cosmesis and less tension during knee flexion.
The bursal sac is incised sharply with a #15 blade. All purulent material is immediately evacuated, and representative swabs or fluid aliquots are sent for aerobic, anaerobic, and AFB cultures. The surgeon must systematically break up any loculations within the bursa using a blunt hemostat or a gloved finger, ensuring that no isolated pockets of infection remain. The cavity is then copiously irrigated with several liters of sterile normal saline, occasionally augmented with dilute Betadine or antibiotic solutions, depending on surgeon preference.
Crucially, the wound is never closed primarily in the setting of acute infection. The cavity is packed loosely with petrolatum gauze, iodoform gauze, or a passive drain (e.g., a Penrose drain) is placed to allow for continuous egress of infected fluid. The extremity is immobilized in a posterior splint in full extension to prevent skin tension and the mechanical pumping action that can disseminate the infection. Intravenous antibiotics are continued based on specific culture sensitivities, and the packing is changed at least twice weekly until the sinus tract heals completely by secondary intention.
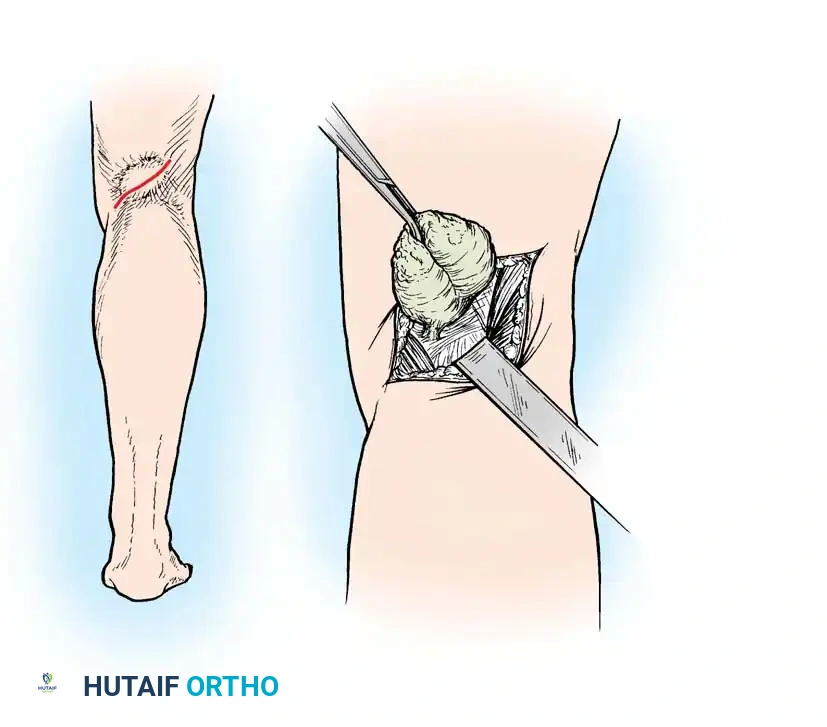
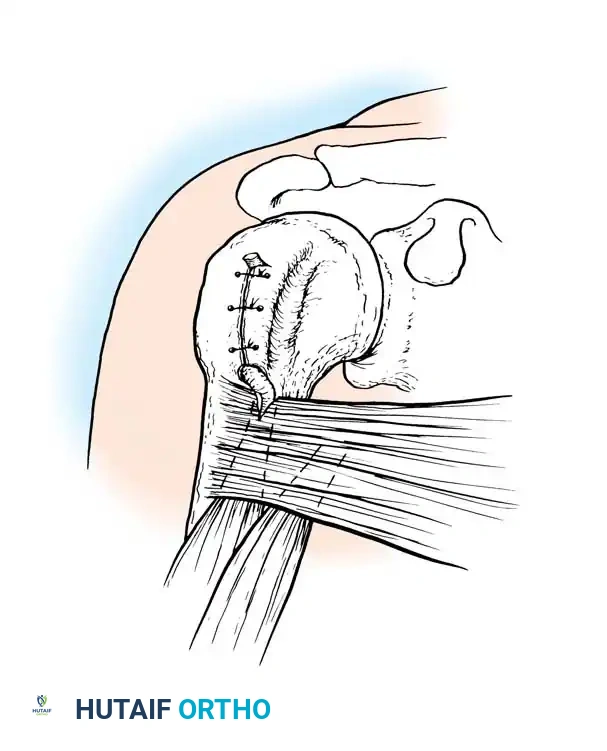
Intraoperative view of prepatellar bursa excision, demonstrating the thick, fibrotic walls characteristic of chronic inflammation.
Surgical Technique: Excision of Prepatellar Bursa (Bursectomy)
For chronic, fibrotic prepatellar bursitis characterized by painful nodules or recurrent sterile effusions, a formal bursectomy is performed. The patient is positioned supine with a proximal thigh tourniquet inflated to provide a bloodless field. A transverse incision of appropriate length is made directly over the center of the bursa. The dissection must carefully separate the bursal sac from the overlying skin and subcutaneous tissue. Maintaining a meticulous, superficial dissection plane is critical to avoid devascularizing the thin anterior skin flaps, which is a primary cause of postoperative wound necrosis.
Once the superficial aspect is freed, the deep surface of the bursa is dissected off the underlying patellar aponeurosis. The surgeon should attempt to excise the bursa en bloc without rupturing it, although this may be impossible in the presence of acute serous effusions. After complete excision, the tourniquet must be deflated prior to closure to obtain absolute hemostasis using electrocautery. The most common complication of superficial bursectomy is postoperative hematoma formation, which can act as a nidus for infection or cause wound dehiscence.
Redundant, devitalized skin edges are sharply trimmed. The dead space is obliterated using closed-suction drainage (e.g., a Hemovac drain) or by placing deep mattress sutures through the skin and underlying aponeurosis, tied over large buttons or bolsters, as classically described by Breck and Higinbotham. A bulky, compressive Jones dressing is applied, and the knee is strictly immobilized in full extension for two weeks to allow skin flap adherence.
Surgical Technique: Excision of Popliteal (Baker's) Cyst
Surgical excision of a popliteal cyst in an adult is a formidable procedure reserved for massive, multiloculated cysts causing neurovascular compression, and only after intra-articular pathology has been addressed. Originally described by Adams in 1840 and popularized by Baker in 1877, a popliteal cyst is typically a distension of the gastrocnemio-semimembranosus bursa. The patient is positioned prone, and a classic "lazy-S" incision is utilized across the popliteal crease to avoid postoperative flexion contractures.
Posterior approach to the popliteal fossa for excision of a complex, multiloculated Baker's cyst.
The deep fascia is incised, and the cyst is identified between the medial head of the gastrocnemius and the semimembranosus tendon. The tibial nerve and popliteal vessels, located laterally and deep to the cyst, must be unequivocally identified and protected throughout the dissection. The cyst is meticulously mobilized from surrounding soft tissues, tracing it proximally to its stalk, which invariably communicates with the posterior joint capsule.
The stalk is clamped, ligated with heavy non-absorbable suture (e.g., #1 Ethibond), and sharply divided. The remaining capsular defect must be securely closed, often requiring a local capsular shift or reinforcement with a portion of the medial gastrocnemius tendon to prevent synovial fluid extrusion and inevitable recurrence. The wound is closed in layers over a closed-suction drain, and the leg is immobilized in 10 to 15 degrees of flexion to minimize tension on the posterior capsular repair.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for bursitis, particularly superficial bursectomies over the patella and olecranon, is fraught with a surprisingly high complication rate. The subcutaneous nature of these bursae, combined with the extreme mobility and poor vascularity of the overlying skin, creates a hostile environment for wound healing. Orthopedic surgeons must maintain a high index of suspicion for postoperative complications and be prepared to execute rapid salvage protocols to prevent devastating outcomes, such as exposed patellar bone or secondary septic arthritis.
The most frequent complication following bursectomy is hematoma or seroma formation, occurring in up to 15-20% of cases despite meticulous intraoperative hemostasis and the use of drains. Hematomas create tension on the fragile surgical incision, leading to marginal skin necrosis and subsequent wound dehiscence. If a postoperative hematoma is identified, it should be aggressively managed with early aspiration under sterile conditions or formal operative evacuation if it becomes organized or threatens the viability of the skin flaps.
Infection, either superficial cellulitis or deep space infection, is another significant risk, particularly in patients with a history of prior septic bursitis or those with systemic comorbidities like diabetes. Deep infections that penetrate the patellar aponeurosis can rapidly evolve into septic arthritis of the knee, a limb-threatening complication. Salvage management for deep infections requires immediate return to the operating room for radical debridement, copious irrigation, and the initiation of broad-spectrum intravenous antibiotics. In cases of massive skin loss over the patella, consultation with plastic surgery for local rotational flaps (e.g., medial gastrocnemius flap) or split-thickness skin grafting may be required.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Protocol |
|---|---|---|---|
| Hematoma / Seroma | 15% - 20% | Inadequate hemostasis; failure to obliterate dead space; early premature mobilization. | Sterile aspiration; compressive wrapping; operative evacuation if skin necrosis is imminent. |
| Wound Dehiscence / Necrosis | 5% - 10% | Dissection too superficial (devascularizing flaps); excessive tension on closure; longitudinal incisions. | Local wound care; negative pressure wound therapy (VAC); rotational muscle flaps for exposed bone. |
| Recurrent Bursitis | 5% - 15% | Incomplete excision of the bursal sac; failure to address the underlying mechanical or intra-articular trigger. | Repeat conservative management; revision open bursectomy ensuring complete marginal resection. |
| Iatrogenic Nerve Injury | < 2% | Aggressive retraction; poor anatomical knowledge (e.g., tibial nerve in Baker's cyst excision). | Immediate intraoperative repair if transected; neurolysis and observation for traction neuropraxias. |
| Secondary Septic Arthritis | < 1% | Inadvertent capsular penetration during aspiration or bursectomy; contiguous spread of untreated deep infection. | Emergent arthroscopic or open joint lavage; prolonged IV antibiotics; infectious disease consultation. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following surgical management of tendinitis and bursitis is as critical to the ultimate clinical outcome as the surgical procedure itself. The rehabilitation protocol must strike a delicate balance between protecting the fragile surgical wound and preventing deleterious joint stiffness and muscle atrophy. The protocol is generally divided into four distinct phases, tailored to the specific anatomical site and the nature of the surgical intervention.
Phase I: Protection and Immobilization (Weeks 0 - 2)
The primary goal of the initial postoperative phase is wound healing and the prevention of hematoma formation. For superficial bursectomies (e.g., prepatellar), the extremity is immobilized in a bulky, compressive Jones dressing and a posterior splint or hinged knee brace locked in full extension. Flexion is strictly prohibited during this phase, as it places immense tension on the anterior skin flaps, risking dehiscence. Weight-bearing is typically allowed as tolerated with crutches, provided the knee remains locked in extension. Isometric exercises, such as quadriceps sets and ankle pumps, are initiated immediately on postoperative day one to maintain muscle tone and promote venous return.
Phase II: Early Range of Motion (Weeks 2 - 4)
Upon confirmation of primary wound healing and removal of sutures (typically at 14 days), the patient transitions to Phase II. The goal is to gradually restore joint range of motion (ROM) while continuing to protect the healing deep tissues. For knee procedures, passive and active-assisted ROM exercises are initiated, progressing slowly from 0 to 90 degrees. Stationary cycling with a high seat may be introduced to encourage gentle, low-resistance mobility. Aggressive passive stretching is avoided to prevent reactive effusion. Weight-bearing is progressed to full, and patients are transitioned out of the locked brace as quadriceps control normalizes.
Phase III: Strengthening and Eccentric Loading (Weeks 4 - 8)
Once full, painless ROM is achieved, the focus shifts to restoring muscular strength, endurance, and proprioception. This phase is particularly critical for patients recovering from tendinopathy procedures. Physical therapy protocols heavily emphasize eccentric strengthening exercises, which have been biomechanically proven to stimulate collagen alignment and tendon remodeling. Closed kinetic chain exercises, such as leg presses, mini-squats, and step-ups, are incorporated. Dynamic flexibility protocols for the hamstrings, quadriceps, and gastrocnemius-soleus complex are essential to correct any underlying kinetic chain deficits that contributed to the initial pathology.
Phase IV: Return to Play and Work Hardening (Weeks 8+)
The final phase involves functional, sport-specific, or occupation-specific training. Patients are cleared to return to heavy labor or competitive athletics only when they demonstrate symmetric strength (at least 90% of the contralateral limb on isokinetic testing), full dynamic stability, and an absence of effusion or localized tenderness. For patients with occupational bursitis (e.g., carpenters), ergonomic counseling and the mandatory use of heavy-duty, gel-padded knee orthoses are required to prevent recurrence upon return to work.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of tendinitis and bursitis is built upon a foundation of robust anatomical and clinical research spanning over a century. A thorough understanding of this landmark literature is essential for the academic orthopedic surgeon, as it provides the evidence-based rationale for current treatment algorithms and surgical techniques.
The histological classification of bursae was definitively established by Kuhns in the mid-20th century. His seminal work demonstrated the subtle but critical differences between innate, anatomically present bursae with true endothelial linings and adventitious bursae that develop strictly from mesenchymal tissue in response to chronic mechanical friction. This histological distinction explains the propensity of adventitious bursae to develop thick, fibrotic, and highly reactive walls that often necessitate surgical excision when conservative measures fail.
In the realm of medial knee pathology, the anatomical descriptions by Voshell and Brantigan remain the gold standard. They meticulously mapped the bursal complex located deep to the superficial medial collateral ligament, identifying up to three distinct bursal sacs. Their work highlighted how distension of these specific bursae perfectly mimics the mechanical symptoms of a medial meniscus tear, a diagnostic pitfall that continues to challenge modern clinicians. Similarly, Hendryson's anatomical studies of the lateral knee delineated the fibular collateral ligament bursa, providing the anatomical basis for differentiating lateral bursitis from parameniscal cysts and biceps femoris tendinopathy.
The pathophysiology and management of popliteal (Baker's) cysts were revolutionized by the combined works of Meyerding, Van Demark, Touloukian, and Malloch. Meyerding and Van Demark first established the one-way valve mechanism that allows synovial fluid to escape from the knee joint into the gastrocnemio-semimembranosus bursa during knee flexion, preventing its return. This discovery fundamentally shifted the surgical approach from simple posterior cyst excision to addressing the primary intra-articular pathology. Later, Touloukian and Malloch provided critical epidemiological insights, highlighting the stark differences between pediatric and adult presentations. They demonstrated that pediatric popliteal cysts rarely communicate with the joint and almost universally resolve with benign neglect, whereas adult cysts are inextricably linked to intra-articular derangement (primarily medial meniscus tears and osteoarthritis) and require arthroscopic management of the joint to prevent recurrence.
Modern clinical guidelines, supported by the American Academy of Orthopaedic Surgeons (AAOS), heavily emphasize a stepwise, conservative approach to these pathologies. Surgical intervention is strictly reserved for recalcitrant cases, acute suppuration, or compressive neuropathies. The literature consistently warns against the indiscriminate use of intra-bursal corticosteroid injections, particularly in the setting of suspected infection or directly into tendinous structures, due to the high risk of iatrogenic rupture and the masking of pyogenic symptoms. Ultimately, successful operative management relies on meticulous surgical technique, rigorous dead space management, and a deep respect for
