Mastering PIP Joint Collateral Ligament Reconstruction via Tendon Graft

Key Takeaway
Chronic instability of the proximal interphalangeal (PIP) joint following a neglected or severe collateral ligament rupture often necessitates surgical reconstruction. Utilizing a free tendon graft, such as the palmaris longus, restores coronal plane stability and joint kinematics. This advanced surgical guide details the biomechanical principles, precise anatomical approaches, graft routing techniques, and postoperative rehabilitation protocols required to achieve optimal functional outcomes in complex PIP joint ligamentous reconstructions.
Comprehensive Introduction and Patho-Epidemiology
The proximal interphalangeal (PIP) joint is the functional epicenter of the digital ray, contributing to over eighty percent of the total arc of digital flexion required for a functional power grip and precision pinch. As a highly constrained ginglymus (hinge) joint, it relies profoundly on its intricate ligamentous architecture for stability throughout its extensive and demanding arc of motion. The primary static stabilizers are the proper collateral ligaments (PCL), the accessory collateral ligaments (ACL), and the robust fibrocartilaginous volar plate. Rupture of the collateral ligament complex typically results from high-energy forced lateral deviation coupled with rotational torque. If left untreated, or if primary repair fails due to biological or mechanical inadequacy, this injury invariably leads to debilitating chronic instability, persistent pain, and a profound diminution of grip and pinch strength.
The epidemiology of PIP joint collateral ligament injuries reveals a high prevalence among athletes engaged in ball sports, as well as manual laborers subjected to sudden, unexpected loading of the digits. While acute, low-grade sprains may be managed conservatively with buddy taping and early mobilization, complete ruptures—particularly those involving the radial collateral ligament of the index finger, which must withstand the immense forces of key pinch—often demand surgical intervention. The patho-epidemiology of chronic instability is characterized by the gradual attenuation of secondary stabilizers. As the primary collateral ligament remains incompetent, the repetitive application of varus or valgus stress leads to the progressive stretching of the volar plate and the extensor mechanism, culminating in multiplanar instability and, ultimately, post-traumatic arthrosis.
When direct anatomical repair is precluded by tissue retraction, poor tissue quality, or the chronicity of the injury (typically defined as presenting more than six weeks post-trauma), reconstruction utilizing a free tendon graft becomes the gold standard of care. Chronic attenuation results in a biological environment where native ligament remnants are replaced by disorganized, non-functional scar tissue that cannot hold suture under physiological loads. This comprehensive, advanced textbook chapter delineates the precise surgical technique for replacing a ruptured collateral ligament of the PIP joint using a tendon autograft. It provides an exhaustive guide to restoring coronal stability, re-establishing functional kinematics, and preventing the devastating sequelae of chronic digital instability.
Undiagnosed Interphalangeal Dislocations
Failure to diagnose interphalangeal dislocations in the acute setting is a rare but catastrophic clinical error that severely complicates subsequent management. Rapid onset of profound soft tissue edema often obscures the bony landmarks that typically make early diagnosis straightforward. In the emergency department or primary care setting, the absence of immediate radiographic evaluation can lead to the misclassification of a frank dislocation or subluxation as a simple "jammed finger." This diagnostic failure sets the stage for rapid, irreversible joint destruction.
🚨 SURGICAL WARNING: If a PIP joint dislocation is not diagnosed and reduced within the first week, the articular cartilage may undergo rapid, mechanical erosion due to abnormal, concentrated pressure from the sharp articular edge of the dislocated phalanx against the opposing condyle. In such delayed presentations, closed reduction is frequently impossible due to soft tissue contracture and early fibrosis, mandating open reduction, extensive debridement, and potential ligamentous reconstruction to salvage joint function.
Irreducible and Complex Dislocations
Certain high-energy injury patterns result in irreducible dislocations due to the complex interposition of surrounding soft tissues. A classic and notoriously challenging example is the complete rupture of the collateral ligament accompanied by the trapping of the lateral band of the extensor hood within the joint space. When the proximal phalanx condyle buttonholes through the extensor mechanism, the lateral band slips volarly and becomes incarcerated between the articular surfaces, acting as a mechanical block to concentric reduction.
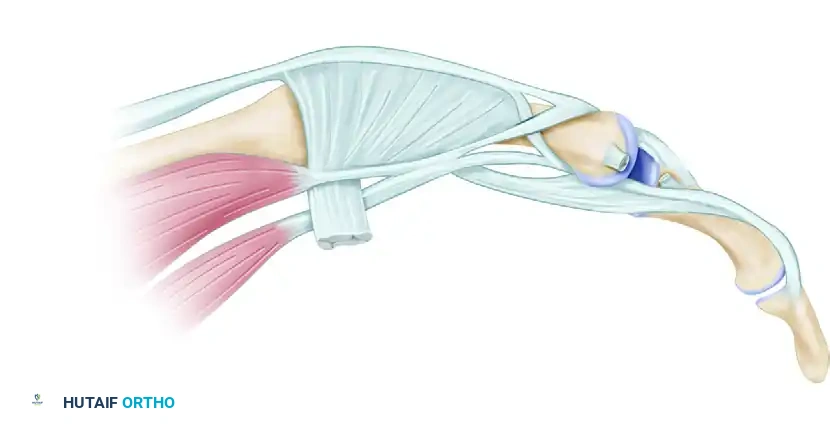
Irreducible dislocation of the proximal interphalangeal joint. The collateral ligament has been torn, and the lateral band of the extensor hood is trapped within the joint (Dorsal view).

Lateral view demonstrating the trapped lateral band preventing concentric reduction.
Similarly, volar dislocations can present with highly complex pathoanatomy, often highly suggestive of a concomitant central slip injury. In severe cases, the radial condyle of the proximal phalanx may buttonhole through the extensor mechanism, trapping the lateral band volarly and creating a profound disruption of the extensor apparatus. These injuries require meticulous open exploration to extract the interposed tissue without causing further iatrogenic damage to the delicate extensor slips.

Volar dislocation of the middle finger PIP joint, suggestive of a central slip injury.
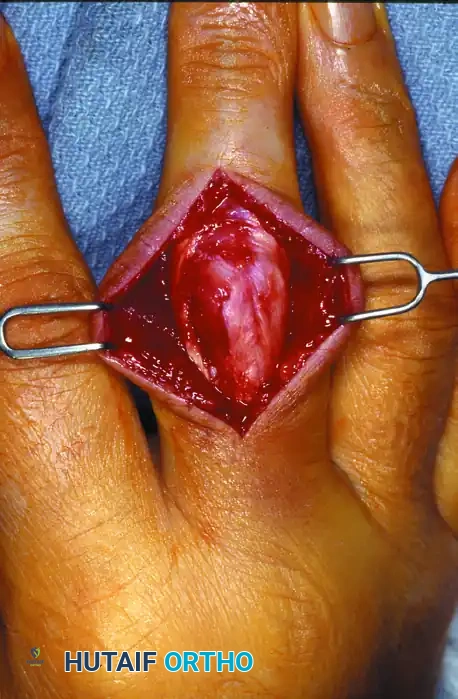
Proximal phalangeal radial condyle buttonholed through the extensor mechanism with the lateral band trapped volarly.

Intraoperative view following the reduction of the trapped lateral band.
Even with acute anatomical repair and the restoration of excellent passive flexion, patients may experience persistent, frustrating extensor lags. This phenomenon occurs due to the severe attenuation of the extensor mechanism sustained during the initial trauma, or secondary to the necessary surgical mobilization. The delicate balance of the extensor hood is easily disrupted, and the central slip may fail to transmit adequate tension to the base of the middle phalanx, highlighting the extreme complexity of managing volar dislocation injuries.

Postoperative clinical presentation demonstrating persistent extensor lag.

Despite acute repair, an extensor lag of 20 degrees persisted, highlighting the complexity of volar dislocation injuries.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate biomechanics and micro-anatomy of the PIP joint is paramount for successful reconstruction. The PIP joint is structurally defined by the bicondylar head of the proximal phalanx articulating with the biconcave base of the middle phalanx. The geometry of the proximal phalanx head is not perfectly spherical; it exhibits a "cam effect," meaning the radius of curvature increases from dorsal to volar. This anatomical nuance dictates the tensioning of the collateral ligaments throughout the arc of motion.
The proper collateral ligament (PCL) is a robust, cord-like structure that originates from a distinct depression on the dorsal-lateral aspect of the proximal phalanx head. It courses obliquely and distally to insert into the volar-lateral base of the middle phalanx. Because of the cam effect of the proximal condyle, the PCL is relatively lax in full extension but becomes maximally taut at approximately 70 to 90 degrees of flexion, providing maximal stability against varus and valgus stress during power grip.
The Accessory Collateral Ligament and Volar Plate Complex
The accessory collateral ligament (ACL) originates volar and slightly proximal to the PCL origin on the proximal phalanx. Unlike the PCL, which inserts into bone, the ACL fans out to insert broadly into the lateral margins of the volar plate. This anatomical arrangement ensures that the ACL remains taut in full extension, stabilizing the volar plate and preventing hyperextension of the PIP joint. The volar plate itself is a thick, fibrocartilaginous structure that forms the floor of the PIP joint, acting as a vital checkrein against dorsal dislocation.
During surgical reconstruction, recreating the isolated function of the PCL is often insufficient if the ACL and volar plate complex are profoundly attenuated. The surgeon must understand that the native collateral ligament complex functions as a singular, continuous sheet of tissue with varying vectors of tension. The true isometric point of the PIP joint—the point where a reconstructed ligament will experience minimal length change during flexion and extension—is located slightly dorsal and proximal to the central axis of rotation of the proximal phalanx condyle. Identifying and utilizing this exact isometric footprint is the most critical biomechanical step in tendon graft reconstruction to prevent postoperative stiffness or recurrent laxity.
Exhaustive Indications and Contraindications
Reconstruction of the PIP joint collateral ligament via tendon graft is not a first-line treatment for acute injuries, save for exceptional circumstances involving massive tissue loss. The procedure is technically demanding and carries a significant risk of postoperative stiffness. Therefore, patient selection must be rigorous, and the indications must be clearly established based on clinical examination, chronicity, and functional deficit.
The primary indication is chronic, symptomatic instability that severely impairs the patient's activities of daily living or occupational duties. This is most frequently seen in the radial collateral ligament (RCL) of the index finger. The index RCL must resist the powerful, repetitive adduction forces generated by the thumb during key pinch. A deficient index RCL leads to profound pinch weakness and disabling pain. Similarly, ulnar collateral ligament (UCL) injuries of the small finger can lead to a severely compromised power grip, as the digit diverges radially during grasp.

Chronically unstable proximal interphalangeal joint permitting abnormal tilting and producing severe pain during pinch maneuvers.

Restoration of coronal alignment achieved by a segmental graft from the palmaris longus tendon attached through transosseous tunnels.
Table of Indications and Contraindications
| Category | Specific Clinical Scenarios | Rationale for Inclusion/Exclusion |
|---|---|---|
| Absolute Indications | Chronic symptomatic instability (>6 weeks) with failed conservative management. | Native ligament is entirely replaced by non-functional scar tissue; direct repair is impossible. |
| Failed primary anatomical repair. | Tissue quality is compromised; biological augmentation via autograft is required. | |
| Acute injuries with massive soft tissue avulsion or crushing. | Insufficient local tissue remains to achieve a stable, functional repair. | |
| Relative Indications | Subacute injuries (3-6 weeks) with highly retracted ligament ends. | Attempted primary repair may over-tension the joint; grafting provides necessary length. |
| High-demand athletes requiring immediate, rigid biological constructs. | Autograft reconstruction may offer a more robust construct than primary repair in select elite athletes. | |
| Absolute Contraindications | Active local or systemic infection. | High risk of deep joint infection and catastrophic failure of the free tendon graft. |
| Severe, symptomatic post-traumatic osteoarthritis of the PIP joint. | Reconstructing ligaments around a destroyed arthritic joint will not relieve pain; arthrodesis or arthroplasty is indicated. | |
| Relative Contraindications | Poor patient compliance or inability to participate in rigorous rehabilitation. | The procedure requires meticulous postoperative therapy; non-compliance guarantees severe stiffness or rupture. |
| Severe concomitant extensor mechanism destruction. | Lack of active extension will render the stabilized joint functionally useless. |
Alternative Interventions: Dynamic External Fixation
In cases of acute fracture-subluxations where ligamentous reconstruction is not immediately feasible—often due to the presence of highly comminuted intra-articular fractures that cannot support bone tunnels—dynamic external fixation may be employed. This technique maintains joint congruity and capsular distraction while allowing early, protected active motion.
Proximal interphalangeal joint fracture-subluxation.

Application of a dynamic external fixator to maintain reduction.

Lateral radiographic view confirming concentric joint reduction with the dynamic external fixator in place.
Dynamic external fixation utilizes the principle of ligamentotaxis to mold the healing fracture fragments while preventing the stiffness associated with static immobilization. Once the fracture has healed (typically 4 to 6 weeks), the fixator is removed. If residual, symptomatic collateral ligament instability persists after bony union and a course of therapy, the surgeon may then proceed with a delayed tendon graft reconstruction in a more stable osseous environment.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential for anticipating intraoperative challenges and ensuring a smooth surgical workflow. Clinical evaluation must include a precise assessment of the axis of instability. Varus and valgus stress testing should be performed with the PIP joint in both full extension and 30 degrees of flexion to isolate the ACL and PCL, respectively. Comparison with the contralateral, uninjured digit is mandatory to establish the patient's baseline physiological laxity. Radiographic evaluation, including true AP, lateral, and oblique views, is required to rule out subluxation, avulsion fractures, or advanced arthritic changes that would contraindicate soft tissue reconstruction.
Graft selection must be discussed with the patient preoperatively. The palmaris longus (PL) tendon is the undisputed graft of choice due to its expendability, appropriate caliber, and ease of harvest. The presence of the PL must be confirmed clinically using Schaeffer's test (opposition of the thumb and small finger with wrist flexion). In the 15% of the population where the PL is congenitally absent, alternative options must be planned. These include a partial-thickness slip of the flexor carpi radialis (FCR), a slip of the abductor pollicis longus (APL), or a toe extensor tendon (typically the extensor digitorum longus to the second or third toe).
Anesthesia, Tourniquet, and Patient Positioning
- Anesthesia: A regional block (axillary or supraclavicular brachial plexus block) is highly preferred. It provides excellent intraoperative anesthesia, profound muscle relaxation, and extended postoperative analgesia, facilitating early rehabilitation. General anesthesia is rarely required unless patient anxiety dictates otherwise.
- Positioning: The patient is positioned supine with the operative arm extended on a radiolucent hand table. The hand should be secured, but the digits must remain completely free to allow for intraoperative manipulation and assessment of kinematics.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is applied. Following strict exsanguination with an Esmarch bandage, the tourniquet is inflated to 250 mm Hg (or 100 mm Hg above systolic pressure) to ensure a bloodless, pristine surgical field, which is critical for identifying the delicate micro-anatomy of the digit.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a PIP joint collateral ligament reconstruction demands meticulous soft tissue handling, precise identification of isometric points, and rigid initial fixation. The procedure is unforgiving; minor deviations in tunnel placement can result in severe kinematic derangement.
1. Surgical Approach and Exposure
- Incision: A midlateral (or midaxial) incision is made over the proximal interphalangeal joint on the side of the collateral ligament insufficiency. The incision should be centered over the joint line, extending from the mid-diaphysis of the proximal phalanx to the mid-diaphysis of the middle phalanx. The midlateral approach minimizes the risk of postoperative scar contracture limiting flexion.
- Dissection: Careful sharp and blunt dissection is carried through the subcutaneous tissues. It is imperative to identify, mobilize, and protect the dorsal sensory branches of the digital nerve and the accompanying digital artery. Retraction of these neurovascular structures must be gentle to prevent neurapraxia.
- Extensor Mechanism Reflection: Identify the transverse retinacular ligament (TRL), which runs from the volar capsule to the lateral band of the extensor mechanism. Incise the TRL longitudinally to create a window, allowing the lateral band to be mobilized. Reflect the extensor mechanism dorsally to expose the underlying joint capsule and the fibrotic remnants of the collateral ligament.
2. Joint Preparation and Scar Excision
- Debridement: Perform a limited arthrotomy to inspect the joint for any osteochondral fragments, loose bodies, or interposed soft tissue. Excise the dense, disorganized scar tissue from around the anatomical origin (proximal phalanx head) and insertion (middle phalanx base) of the cord fibers of the collateral ligament.
- Preparation of the Bed: Ensure the bony surfaces where the graft will interface are lightly decorticated using a high-speed burr or a curette. This creates a bleeding bony bed that promotes rapid biological integration and healing of the tendon-to-bone interface.
3. Bone Tunnel Preparation
Precise placement of the bone tunnels is the most critical step to ensure isometric function of the reconstructed ligament. Non-isometric placement will result in either a ligament that is too tight in flexion (preventing a full fist) or too loose in extension (failing to provide stability).
* Proximal Tunnel: Identify the isometric point on the condyle of the proximal phalanx. This point is located slightly dorsal and proximal to the true center of rotation of the condylar head. Surgical Pearl: Before drilling, place a small K-wire at the suspected isometric point, loop a suture around it, and attach it to the distal insertion site. Take the joint through a full range of motion. If the suture tension changes by more than 1-2 mm, reposition the K-wire until isometry is achieved. Once confirmed, drill a hole completely through the bone from the injured side to the contralateral side using a 1.5 mm or 2.0 mm drill bit, ensuring a trajectory perpendicular to the longitudinal axis of the phalanx.
* Distal Tunnel: Identify the insertion footprint at the volar-lateral base of the middle phalanx. Drill a second hole completely through the bone on this side of the joint, maintaining a similar perpendicular trajectory.
4. Graft Harvest
- Palmaris Longus Harvest: Obtain the necessary graft material. Make a small transverse incision at the distal wrist crease over the palmaris longus tendon. Using a minimally invasive tendon stripper (e.g., Brand tendon stripper), harvest an adequate length of the tendon. Typically, 6 to 8 cm is required to allow for secure fixation and potential creation of an ACL.
- Graft Preparation: On the back table, meticulously clean the graft of any adherent muscle belly or paratenon to prevent bulky passage through the bone tunnels. Whipstitch both ends of the graft using a strong, non-absorbable 4-0 suture (e.g., braided polyester or ultra-high-molecular-weight polyethylene).
5. Graft Passage and Fixation
- Suture/Wire Loop Application: Tie a 4-0 non-absorbable suture or a 34-gauge wire loop around each whipstitched end of the prepared tendon graft to facilitate passage.
- Initial Passage: Using a suture passing instrument or a straight Keith needle, bring one end of the graft out through the proximal phalanx tunnel, passing from the injured side to the contralateral, intact side.
- Joint Crossing: Pass the other end of the graft across the joint line, carefully mimicking the anatomical, oblique trajectory of the native proper collateral ligament. Thread it through the distal hole in the middle phalanx in the appropriate direction.
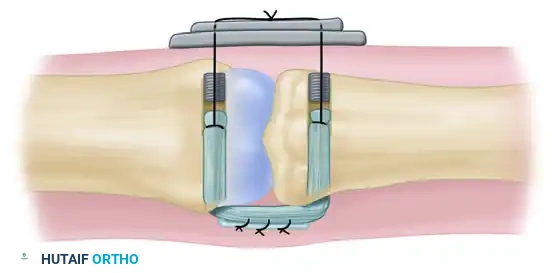
Diagrammatic representation of the reconstruction of the collateral ligament of the proximal interphalangeal joint with a tendon graft. The graft is passed through the transosseous tunnels.
- Button Fixation: Pass each wire loop (or suture ends) on the exiting ends of the graft through a piece of sterile felt (to protect the skin from necrosis) and then through separate holes in a single, sterile standard surgical button resting on the contralateral intact skin.
- Tensioning: This is a crucial maneuver. Pull the graft snug to eliminate laxity. Assess the joint for stability by applying varus/valgus stress. Ensure there is no impingement or excessive resistance during a trial range of motion. The joint should be tensioned at approximately 20 to 30 degrees of flexion. Once optimal tension is achieved, tie the two wires (or sutures) together securely over the button. (Note: While modern techniques occasionally utilize small bone anchors or interference screws for fixation, the transosseous pull-out button technique remains the classic, highly reliable gold standard described in definitive texts, as it allows for precise, adjustable tensioning without introducing bulky hardware into the small phalanges).
6. Creation of an Accessory Collateral Ligament (Optional but Recommended)
To comprehensively restore the volar stability provided by the accessory collateral ligament and prevent postoperative hyperextension, an advanced adjunctive technique may be employed.
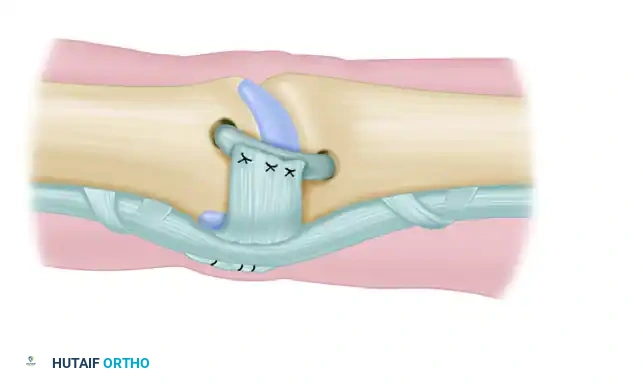
* Flexor Sheath Utilization: An accessory collateral ligament may be created utilizing local tissue. Section a portion of the flexor tendon sheath—typically the A3 pulley or the adjacent cruciform tissue (C1/C2)—on the side opposite the defect.
* Transposition: Carefully maintain its insertion into the bone on the side of the involved collateral ligament. Fold this robust, fascia-like sheath over the newly grafted tendon.
* Suturing: Suture this sheath tissue directly to the tendon graft using fine, non-absorbable sutures. This must be performed with the finger held in full extension to ensure appropriate tensioning of the volar structures, effectively recreating the checkrein function of the native ACL and volar plate complex.
Creation of an accessory collateral ligament utilizing a portion of the flexor sheath folded over and sutured to the primary tendon graft.
7. Joint Transfixion and Closure
- K-Wire Stabilization: To absolutely protect the reconstruction during the vulnerable initial phase of biological healing and to prevent inadvertent stretching of the graft, transfix the PIP joint. Drive an oblique 0.045-inch Kirschner wire (K-wire) across the joint, positioning the PIP in approximately 20 to 30 degrees of flexion.
- Closure: Meticulously repair the transverse retinacular ligament with fine absorbable sutures (e.g., 5-0 Vicryl). Failure to close the TRL can lead to dorsal subluxation of the lateral band and a subsequent swan neck deformity. Close the skin with interrupted non-absorbable sutures (e.g., 5-0 Nylon).
- Dressing: Apply a bulky, non-adherent compressive dressing. Fabricate a custom volar plaster or fiberglass splint, maintaining the PIP joint in the transfixed position and the metacarpophalangeal (MCP) joint in 70 degrees of flexion to prevent collateral ligament contracture at the MCP level.
💡 CLINICAL PEARL: Over-tensioning the tendon graft is the single most common surgical pitfall in this procedure, invariably leading to severe, intractable postoperative stiffness. The graft should be tensioned just enough to eliminate abnormal joint opening under varus/valgus stress. It must not be drawn so tight that it compresses the articular surfaces together, which will destroy the gliding mechanics of the joint.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following PIP joint collateral ligament reconstruction are not uncommon. The delicate balance between achieving stability and maintaining motion makes this one of the most challenging procedures in hand surgery.
Table of Complications and Management Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Management and Salvage Strategy |
|---|---|---|---|
| Joint Stiffness | 30% - 50% | Over-tensioning the graft; non-isometric tunnel placement; prolonged immobilization (>4 weeks); excessive scar formation. | Aggressive hand therapy, dynamic splinting. If refractory after 6 months, surgical tenolysis and capsulotomy may be required. |
| **Recurrent |
