Surgical Masterclass: Advanced Repair of Athletic Pubalgia with Dual-Layer Mesh Technique
Key Takeaway
This masterclass provides an exhaustive guide to athletic pubalgia repair, focusing on dual-layer mesh techniques. Fellows will gain real-time insights into comprehensive surgical anatomy, meticulous intraoperative execution, and critical pearls for managing complex groin injuries. We cover precise incision, deep dissection, hardware application, and strategies to prevent recurrence, ensuring optimal recovery and return to sport for athletes.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are addressing a notoriously challenging and frequently misunderstood clinical entity: Athletic Pubalgia, colloquially referred to as a "sports hernia." It is imperative to understand from the outset that this condition is not a true hernia in the traditional general surgical sense. Rather, it represents a complex spectrum of chronic groin injuries predominantly seen in high-performance athletes, characterized by a tear, attenuation, or micro-avulsion of the posterior inguinal wall and the rectus abdominis insertion, notably without a clinically obvious visceral bulge. The complexity of the groin's myoaponeurotic anatomy dictates that accurate diagnosis is paramount, as multiple pathologies frequently coexist and confound the clinical picture. We must rigorously differentiate athletic pubalgia from osteitis pubis, primary adductor strains, stress fractures, and a host of other conditions ranging from intra-articular hip joint disorders (such as femoroacetabular impingement) to referred lumbosacral radiculopathy.
The epidemiological profile of athletic pubalgia is highly specific, predominantly affecting athletes engaged in sports that demand repetitive, explosive twisting, cutting, and kicking motions. Consequently, we see the highest incidence in soccer, ice hockey, rugby, and American football players. The pathophysiology is fundamentally rooted in a biomechanical imbalance across the anterior pelvis. The pubic symphysis acts as a central fulcrum. Superiorly, the robust rectus abdominis exerts an upward and posterior force, while inferiorly, the powerful adductor longus exerts a downward and anterior force. These muscular insertions blend intimately over the anterior pubis to form a contiguous prepubic aponeurotic complex. When the kinetic chain is disrupted—often due to adductor tightness or hip joint restricted range of motion—the shearing forces across this aponeurotic plate become insurmountable, leading to microtrauma, attenuation of the transversalis fascia, and eventual tearing of the conjoint tendon insertion.
To navigate this diagnostic landscape effectively, one must recognize that "groin pain" in the athlete is an umbrella term. Osteitis pubis, for instance, presents with localized symphyseal pain and radiographic joint disruption, often secondary to the very same biomechanical imbalances that cause pubalgia, making them frequent comorbidities. Adductor strains, particularly at the myotendinous junction, are the most frequent isolated cause of acute groin pain, typically occurring during eccentric loading. However, chronic adductor tendinopathy at its bony insertion is intimately linked to the rectus-adductor aponeurotic plate dysfunction seen in athletic pubalgia.
Stress fractures of the pubic rami or femoral neck, though statistically rarer, represent a "cannot-miss" diagnosis resulting from repetitive cyclic loading. Therefore, our diagnostic paradigm must be exhaustive. It is an absolute clinical necessity to exclude intra-abdominal pathology, genitourinary abnormalities, and occult hip disorders before committing an athlete to a surgical intervention targeting the posterior inguinal wall. Failure to recognize a concomitant cam lesion or labral tear will invariably result in a failed pubalgia repair, as the underlying mechanical restriction driving the pelvic overload remains unaddressed.
Detailed Surgical Anatomy and Biomechanics
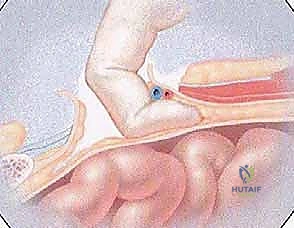
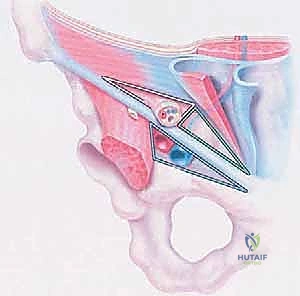
Turning our attention to the surgical anatomy, we must acknowledge that the inguinal region is an incredibly intricate, multi-layered labyrinth. A superficial understanding is insufficient; profound anatomical mastery is absolutely critical for precise diagnosis, successful surgical execution, and the mitigation of iatrogenic neurovascular injuries. The inguinal canal, our primary surgical field, is a complex oblique intermuscular passage. Its anterior boundary is formed primarily by the aponeurosis of the external oblique muscle, which splits medially to form the superficial inguinal ring. The posterior wall, the epicenter of athletic pubalgia pathology, is formed by the transversalis fascia, reinforced medially by the conjoint tendon (falx inguinalis).

The conjoint tendon itself is a critical structure, representing the fusion of the distal aponeuroses of the internal abdominal oblique and transversus abdominis muscles. It inserts onto the pubic crest and pectineal line. In the setting of athletic pubalgia, it is precisely here that we encounter the occult injury: a subtle tear, a profound thinning, or a complete avulsion of this posterior inguinal wall from its pubic insertion. Because the external oblique aponeurosis remains intact, this defect is rarely palpable as a classic reducible hernia. Deep to the canal, the spermatic cord in males (or the round ligament in females) traverses this space. The cord houses critical structures including the vas deferens, the testicular artery, the pampiniform venous plexus, and the genital branch of the genitofemoral nerve.
Neurovascular preservation is the hallmark of a master surgeon in this region. The ilioinguinal nerve typically courses within the inguinal canal, superficial to the spermatic cord, exiting through the external ring to innervate the superior medial thigh and the root of the external genitalia. It is notoriously variable in its course and highly susceptible to transection or entrapment during the incision and mobilization of the external oblique aponeurosis. The iliohypogastric nerve runs more superiorly, deep to the external oblique, supplying sensation to the suprapubic region. The genitofemoral nerve is equally critical; its genital branch courses directly with the spermatic cord, supplying the cremaster muscle. Aggressive or careless mobilization of the cord can lead to debilitating chronic orchialgia.

Furthermore, we must respect the deep vascular landmarks. The inferior epigastric vessels, originating from the external iliac system, ascend superiorly to form the lateral border of Hesselbach's triangle. These vessels must be meticulously identified and protected during the deep dissection of the posterior wall and preperitoneal space to avert catastrophic hemorrhage. The pubic tubercle and Cooper's (pectineal) ligament serve as our primary bony and ligamentous anchors. Understanding the dynamic interplay between these static stabilizers and the dynamic muscular forces of the rectus abdominis, the internal oblique, and the adductor complex is what allows us to reconstruct the anatomy not just statically, but biomechanically, restoring the athlete's explosive core stability.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for athletic pubalgia must be made with rigorous clinical judgment, as conservative management remains the first-line approach. Surgery is strictly indicated for high-demand athletes who have failed a comprehensive, physical therapy-guided conservative rehabilitation program lasting a minimum of 6 to 12 weeks. These patients present with persistent, disabling groin pain that profoundly limits their ability to accelerate, cut, or kick, fundamentally preventing their return to competitive play. The pain must be specifically localized to the inguinal canal, the pubic tubercle, or the conjoint tendon insertion, and must be reliably reproduced by provocative maneuvers such as a resisted sit-up or a dynamic Valsalva maneuver.
Conversely, the contraindications to this procedure are equally important to delineate. Absolute contraindications include active local or systemic infection, severe uncorrected coagulopathy, and the presence of a true, large, strangulated or incarcerated inguinal hernia that requires emergent general surgical intervention rather than an elective sports repair. However, the most critical relative contraindication—and the most common cause of surgical failure—is the presence of untreated, symptomatic intra-articular hip pathology. If an athlete possesses symptomatic femoroacetabular impingement (FAI) with restricted internal rotation, the mechanical stress will simply bypass the repaired inguinal floor and continue to overload the pelvis. In such cases, the hip pathology must be addressed either prior to or concurrently with the pubalgia repair.
Furthermore, patients with isolated, acute adductor avulsions or severe osteitis pubis without concomitant posterior wall attenuation may not be appropriate candidates for an isolated mesh repair of the inguinal floor. These pathologies require their own specific targeted interventions, such as adductor tenotomy or, in rare, recalcitrant cases of osteitis pubis, symphyseal arthrodesis. We must also carefully evaluate patients with a history of chronic pain syndromes or multiple prior failed groin surgeries, as the altered anatomical planes and established neuropathic pain pathways significantly reduce the probability of a successful outcome from a standard dual-layer mesh repair.
Indications and Contraindications Summary
| Category | Specific Clinical Scenarios | Rationale / Impact |
|---|---|---|
| Primary Indications | Failure of 6-12 weeks of targeted physical therapy. | Confirms chronicity and failure of intrinsic tissue healing. |
| Disabling pain preventing return to sport (RTS). | Quality of life and functional deficit justify surgical risk. | |
| MRI evidence of rectus/adductor aponeurotic plate injury. | Confirms structural anatomical defect requiring mechanical repair. | |
| Positive resisted sit-up and Valsalva with localized pain. | Clinically localizes the pathology to the posterior inguinal wall. | |
| Absolute Contraindications | Active local dermatological or systemic infection. | High risk of catastrophic mesh infection and systemic sepsis. |
| Uncorrected bleeding diathesis / coagulopathy. | Risk of massive retroperitoneal or preperitoneal hematoma. | |
| Relative Contraindications | Untreated, symptomatic Femoroacetabular Impingement (FAI). | Ongoing mechanical restriction will cause the mesh repair to fail. |
| Isolated acute adductor longus rupture. | Requires primary tendon repair or tenotomy, not inguinal mesh. | |
| Severe, isolated lumbosacral radiculopathy. | Pain generator is spinal; inguinal surgery will provide no relief. |
Pre-Operative Planning, Templating, and Patient Positioning
Our journey begins long before the scalpel touches the skin; meticulous preoperative planning is the bedrock of surgical success. The most critical step is confirming the diagnosis through a synthesis of a highly detailed history, a nuanced physical examination, and the judicious application of advanced imaging studies. Athletes typically present with deep, disabling groin pain that is insidious in onset, progressively worsening with specific athletic movements like kicking, sprinting, or sudden directional changes. They frequently report an exacerbation of pain with increased intra-abdominal pressure—such as coughing, sneezing, or a Valsalva maneuver—and note that the pain generally subsides with rest, only to recur immediately upon returning to the field.
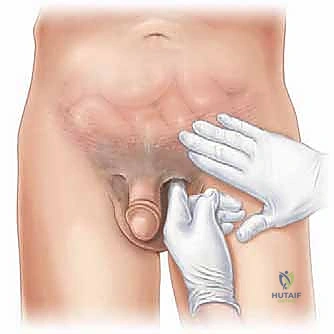
The physical examination must be systematic and exhaustive. Palpation is directed at the pubic symphysis to assess for osteitis pubis, the adductor origin to evaluate for tendinopathy, and the insertion of the conjoint tendon at the pubic tubercle to identify the classic sports hernia defect. In male patients, a direct hernia assessment is performed by invaginating the loose scrotal skin and gently advancing the index finger through the external inguinal ring. While a classic, bulging hernia is absent, asking the patient to perform a Valsalva maneuver often reveals a subtle, palpable tearing sensation, a focal weakness, or a distinct attenuation of the inguinal floor. Comprehensive hip range of motion testing, including the Thomas test for iliopsoas contracture and the FADIR test for anterior impingement, is mandatory to rule out concomitant intra-articular pathology.
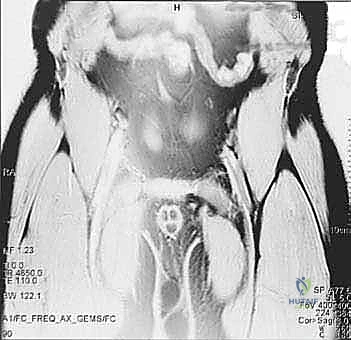
Imaging serves to confirm our clinical suspicions and map the anatomical damage. Standard radiographs (AP pelvis, flamingo views) are essential for excluding stress fractures, avulsion injuries, and identifying the characteristic sclerotic, irregular borders of the pubic symphysis seen in osteitis pubis. However, high-resolution Magnetic Resonance Imaging (MRI) utilizing dedicated athletic pubalgia protocols is the gold standard. MRI provides unparalleled visualization of bone marrow edema, rectus abdominis insertion avulsions, adductor microtears, and the integrity of the aponeurotic plate. Dynamic ultrasound, while highly operator-dependent, can also be a valuable adjunct for visualizing posterior wall ballooning in real-time under Valsalva.
In the operating theater, the patient is positioned supine on a standard radiolucent operating table. While fluoroscopy is not routinely required for the soft tissue repair, its availability is prudent should unexpected bony pathology be encountered or if concurrent adductor tenotomy requires precise localization. The entire abdomen, from the umbilicus down to the mid-thighs bilaterally, including the genitalia, is meticulously prepped and draped to allow for wide exposure and the possibility of bilateral exploration. Prior to incision, we administer a preemptive local analgesic block utilizing a mixture of 0.5% lidocaine with epinephrine, 0.25% bupivacaine, and sodium bicarbonate. This multi-modal approach provides immediate hemostasis via vasoconstriction, reduces the pain of injection through buffering, and establishes a profound preemptive analgesic field that significantly blunts the central sensitization of pain pathways, ensuring a smoother emergence from anesthesia and reduced postoperative narcotic requirements.
Step-by-Step Surgical Approach and Fixation Technique
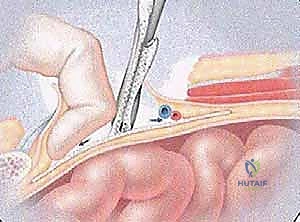
The surgical execution of the dual-layer mesh technique demands precision, anatomical respect, and a profound understanding of groin biomechanics. We initiate the procedure with a standard oblique inguinal incision, approximately 5 to 6 centimeters in length, positioned roughly 1 to 2 centimeters superior and medial to the anatomical axis of the inguinal ligament. This specific placement is strategic; it provides optimal, direct access to the external inguinal ring and the inguinal canal while minimizing undue tension on the wound margins during retraction. Using a #15 blade, the skin and subcutaneous tissues are sharply divided.
Hemostasis is immediately secured using precise electrocautery as we deepen the dissection through Scarpa's fascia. It is critical to maintain a dry field here, ligating any branches of the superficial epigastric or superficial circumflex iliac vessels, as postoperative hematomas in this space are a significant source of morbidity. We proceed with blunt and sharp dissection until the glistening, pearlescent fibers of the external oblique aponeurosis are widely exposed. At this juncture, the surgeon must exercise extreme vigilance regarding the ilioinguinal nerve, which frequently courses just deep to, or even within the fibers of, the external oblique aponeurosis near the external ring.
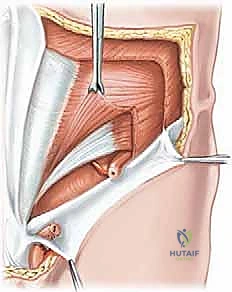
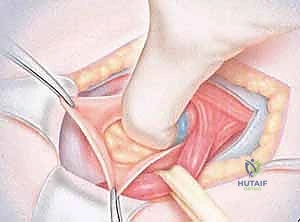
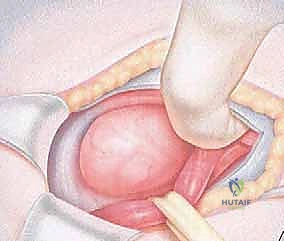
The external oblique aponeurosis is incised parallel to its fibers, extending down through the external inguinal ring. The superior and inferior aponeurotic flaps are elevated. The ilioinguinal nerve is meticulously identified, dissected free from its fascial attachments, and safely retracted using a vessel loop. Next, we mobilize the spermatic cord. Using blunt dissection, the cord is encircled at the level of the pubic tubercle and elevated with a Penrose drain. This maneuver exposes the posterior wall of the inguinal canal—the transversalis fascia and the conjoint tendon. In the athlete with pubalgia, we typically observe a thinned, translucent, or overtly torn posterior wall, lacking the robust, taut character of normal anatomy.
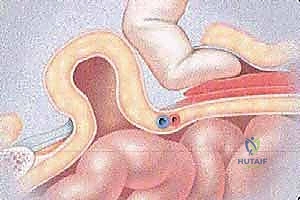
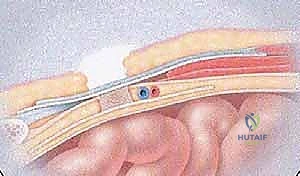
We now commence the dual-layer mesh reconstruction. The first layer involves reinforcing the preperitoneal space. A small incision is made in the attenuated transversalis fascia to enter the space of Bogros. A tailored piece of lightweight, macroporous polypropylene mesh is introduced into this preperitoneal space, positioning it deep to the transversalis fascia to provide a broad, foundational reinforcement against intra-abdominal pressure. This mesh is carefully smoothed out to prevent folding and is typically secured with a few interrupted absorbable sutures to the posterior aspect of the rectus muscle superiorly and Cooper's ligament inferiorly, taking great care to avoid the deep epigastric vessels laterally.
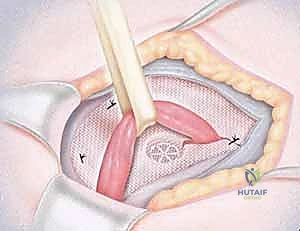
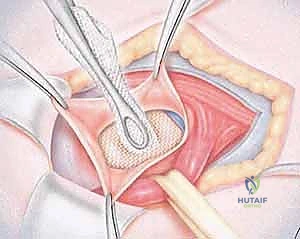
The second, anterior layer of the dual-mesh technique addresses the structural deficit of the conjoint tendon. A second piece of mesh, often a self-gripping or partially absorbable composite mesh, is fashioned to fit the floor of the inguinal canal. It is placed anterior to the newly reconstructed transversalis fascia but deep to the spermatic cord and the external oblique aponeurosis. The inferior border of this mesh is sutured continuously to the shelving edge of the inguinal ligament, from the pubic tubercle extending laterally to the internal ring. The superior border is sutured to the conjoint tendon and the internal oblique aponeurosis.
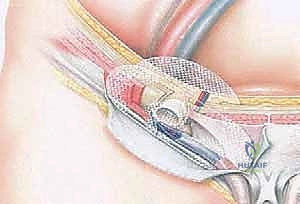
Crucially, the mesh must be tailored to create a snug, but not constricting, new internal ring for the spermatic cord to pass through. The tails of the mesh are crossed lateral to the cord and secured. Once the dual-layer construct is secure, the spermatic cord is returned to its anatomical bed. The external oblique aponeurosis is then meticulously closed over the cord using a running absorbable suture, reconstructing the external inguinal ring.

Finally, Scarpa's fascia is reapproximated to eliminate dead space, and the skin is closed with a running subcuticular suture. This dual-layer approach provides immediate biomechanical stability, addressing both the posterior wall attenuation and the aponeurotic plate disruption, allowing the athlete to begin early, aggressive rehabilitation.
Complications, Incidence Rates, and Salvage Management
While the dual-layer mesh repair for athletic pubalgia boasts a high success rate in carefully selected patients, the procedure is not without risk, and a thorough understanding of potential complications is mandatory. The most devastating and functionally limiting complication is iatrogenic nerve injury. The ilioinguinal, iliohypogastric, and the genital branch of the genitofemoral nerve are all at risk during dissection, mesh placement, and suturing. Injury can occur via direct transection, crush injury from clamps, or entrapment within sutures or the fibrotic scar tissue induced by the mesh. Patients present postoperatively with sharp, burning, neuropathic pain radiating into the scrotum, labia, or medial thigh, often refractory to standard analgesics.
Management of neuropathic pain begins conservatively with membrane-stabilizing agents such as gabapentin or pregabalin, combined with targeted, ultrasound-guided local anesthetic and corticosteroid nerve blocks. If conservative measures fail and a distinct neuroma or entrapment is identified, surgical re-exploration with targeted neurectomy and proximal burying of the nerve stump into the retroperitoneal musculature becomes the salvage procedure of choice. Another significant complication is recurrence or persistence of groin pain. This occurs in approximately 5-10% of cases and is most frequently attributed to a missed concomitant diagnosis, particularly femoroacetabular impingement (FAI) or a primary adductor avulsion that was not addressed during the index procedure.
Infectious and mesh-related complications, while rare (incidence < 1-2%), require aggressive management. Superficial surgical site infections can typically be managed with oral antibiotics and local wound care. However, deep space infections involving the prosthetic mesh represent a surgical emergency. Patients present with erythema, induration, fever, and purulent drainage. In the setting of a deep mesh infection, conservative management almost universally fails. The salvage protocol mandates immediate return to the operating room for wide debridement, complete explantation of the infected mesh, copious irrigation, and closure over drains, accepting that the patient will likely develop a recurrent fascial defect that will require complex abdominal wall reconstruction with biologic grafts at a later, uninfected date.
Complications and Salvage Protocols
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Ilioinguinal Neuralgia | 2% - 5% | Meticulous identification and mobilization; avoiding mesh fixation near nerve path. | Gabapentinoids, diagnostic nerve blocks; eventual targeted neurectomy if refractory. |
| Genitofemoral Neuralgia | 1% - 3% | Gentle handling of spermatic cord; avoiding tight closure of the internal ring around the cord. | Corticosteroid injections; difficult to manage surgically, may require retroperitoneal neurectomy. |
| Recurrent/Persistent Pain | 5% - 10% | Comprehensive pre- |
