Operative Management of Biceps Brachii and Posterior Tibial Tendon Displacement
Key Takeaway
Tendon displacement, particularly involving the long head of the biceps brachii and the posterior tibial tendon, presents unique biomechanical challenges. Surgical management requires meticulous approach selection, ranging from open subpectoral tenodesis to arthroscopic release, often dictated by concurrent rotator cuff pathology. This guide details the indications, step-by-step operative techniques, and evidence-based rehabilitation protocols necessary to restore optimal kinematics and prevent recurrent subluxation in high-demand patients.
Comprehensive Introduction and Patho-Epidemiology
Tendon displacement—encompassing the entire spectrum from dynamic subluxation to frank, irreducible dislocation—represents a complex biomechanical failure of the intricate retinacular and ligamentous pulley systems that stabilize musculotendinous units across diarthrodial joints. While complete tendon ruptures and ischemic myositis (such as acute or chronic exertional compartment syndrome) often dominate the academic discourse on soft-tissue trauma, the subtle yet functionally debilitating nature of tendon instability requires an equally rigorous diagnostic and surgical approach. The failure of these anatomical restraints alters the vector of muscle pull, leading to pathological joint kinematics, accelerated wear of adjacent articular surfaces, and profound chronic pain syndromes that are frequently refractory to non-operative management.
This masterclass focuses on two distinct but biomechanically analogous manifestations of tendon instability: the displacement of the long head of the biceps brachii (LHB) in the upper extremity and the dislocation of the posterior tibial tendon (PTT) in the lower extremity. The patho-epidemiology of LHB displacement reveals that it is rarely an isolated clinical event; it is intimately associated with advanced pathology of the rotator cuff, specifically involving the subscapularis and the supraspinatus tendons. Epidemiologically, LHB instability presents in a bimodal distribution: acute traumatic avulsions of the biceps pulley in young, overhead-throwing athletes, and chronic, attritional failures in the elderly population secondary to progressive rotator cuff arthropathy and degenerative fibrocartilaginous metaplasia.
Conversely, posterior tibial tendon dislocation is an exceedingly rare clinical entity, frequently misdiagnosed in emergency departments and primary care settings as a routine medial ankle sprain. The patho-epidemiology of PTT displacement is heavily tied to acute trauma involving forced dorsiflexion coupled with sudden inversion or eversion of the ankle. This mechanism forcefully avulses or ruptures the flexor retinaculum, allowing the PTT to subluxate anteriorly over the medial malleolus. A critical predisposing anatomical factor is the presence of a shallow or dysplastic retromalleolar groove, which significantly lowers the threshold for retinacular failure. When the groove is morphologically deficient, even low-energy torsional trauma can precipitate chronic, recurrent subluxation.
Synthesizing the clinical burden of both conditions, it becomes evident that delayed diagnosis is the primary enemy of optimal surgical outcomes. Chronic displacement leads to severe tendinosis, longitudinal split tears, and eventual fixed deformities due to the continuous mechanical attrition of the tendon against anomalous bony prominences. Therefore, the orthopedic surgeon must maintain a high index of suspicion when evaluating atypical shoulder or medial ankle pain. Both conditions demand a profound understanding of local anatomy, precise surgical execution, and tailored postoperative rehabilitation to restore native joint kinematics, prevent recurrent pathology, and mitigate the onset of secondary degenerative joint disease.
Detailed Surgical Anatomy and Biomechanics
The Biceps Pulley Complex and Glenohumeral Kinematics
The stability of the long head of the biceps tendon within the bicipital groove is maintained by a highly specialized capsuloligamentous complex known as the "biceps pulley." This anatomical sling is primarily composed of the superior glenohumeral ligament (SGHL), the coracohumeral ligament (CHL), and the distal fascial attachment of the subscapularis tendon. Historically, orthopedic texts heavily emphasized the transverse humeral ligament as the primary restraint to anterior bowstringing of the LHB. However, modern biomechanical and micro-anatomical studies have relegated its importance, demonstrating that the transverse humeral ligament is merely a fascial extension of the subscapularis and pectoralis major, offering negligible resistance to medial subluxation. The true primary stabilizers are the SGHL and CHL, which form a U-shaped suspension sling at the proximal entrance of the intertubercular groove.
Biomechanically, the LHB acts as a dynamic depressor of the humeral head, particularly during the cocking and acceleration phases of overhead throwing. When the biceps pulley system fails—most commonly due to an articular-sided partial tear of the subscapularis—the LHB is permitted to subluxate or dislocate medially into the glenohumeral joint. This medial displacement creates a mechanical disadvantage, altering the tendon's line of pull and inducing a "sawing" effect across the lesser tuberosity and the anterior leading edge of the supraspinatus. Over time, this pathological kinematics leads to hypertrophic tendinopathy, creating an "hourglass" configuration of the biceps tendon that mechanically catches within the joint during shoulder elevation and internal rotation.
The Retromalleolar Groove and Flexor Retinaculum
In the lower extremity, the posterior tibial tendon is anatomically stabilized immediately posterior to the medial malleolus by the rigid retromalleolar groove and the overlying flexor retinaculum (laciniate ligament). The retromalleolar groove is a fibro-osseous tunnel lined with a specialized gliding epitenon layer. The osseous morphology of this groove is highly variable; in a normal anatomical state, it is sufficiently deep (averaging 3-4 mm) to house the PTT securely. The flexor retinaculum, extending from the medial malleolus to the calcaneus, acts as the primary soft-tissue roof, preventing anterior and medial bowstringing of the tendon during active ankle motion.
Biomechanically, the PTT is the primary dynamic stabilizer of the medial longitudinal arch and the principal invertor of the midfoot. During the stance phase of the gait cycle, the PTT undergoes significant excursion and tensile loading, generating forces that can exceed three times body weight. If the retromalleolar groove is congenitally shallow or flattened, the vector forces generated during forced dorsiflexion and inversion are transmitted entirely to the flexor retinaculum. Once the retinaculum ruptures or stretches plastically, the tendon subluxates anteriorly over the medial malleolus. This displacement not only causes acute mechanical snapping and pain but also profoundly diminishes the tendon's mechanical advantage, leading to secondary hindfoot valgus and progressive flatfoot deformity if left untreated.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention in tendon displacement relies heavily on a thorough clinical examination, advanced imaging, and an assessment of the patient's functional demands. Surgical intervention is generally indicated in patients with symptomatic, MRI-confirmed tendon displacement who have failed exhaustive conservative management, including non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy focusing on eccentric strengthening, and judicious use of corticosteroid injections (though contraindicated directly within the tendon substance).
For the long head of the biceps, surgical management has evolved from simple ligamentous repair to definitive tenodesis or tenotomy. Medial dislocation of the biceps tendon is pathognomonic for a subscapularis tear; thus, isolated repair of the LHB pulley without addressing the rotator cuff is universally condemned due to unacceptably high failure rates. Indications for LHB tenodesis include chronic subluxation with associated subscapularis tears, >25% tearing of the LHB substance, an "hourglass" biceps causing mechanical locking, and superior labral anterior-posterior (SLAP) lesions in patients over the age of 40. Contraindications include profound medical comorbidities precluding anesthesia, active glenohumeral infection, and asymptomatic displacement discovered incidentally on imaging.
For the posterior tibial tendon, operative intervention is the absolute gold standard for recurrent dislocation, as conservative management universally fails to restore the mechanical block required to prevent subluxation. Indications include acute traumatic dislocation in high-demand athletes, chronic recurrent subluxation with persistent medial ankle pain, and MRI evidence of longitudinal split tears secondary to mechanical attrition over the malleolus. Contraindications encompass fixed rigid hindfoot valgus deformities (which require corrective osteotomies or arthrodesis rather than isolated soft-tissue procedures), advanced peripheral vascular disease compromising the surgical watershed zone, and profound peripheral neuropathy (e.g., Charcot arthropathy) where soft-tissue reconstruction will inevitably fail.
| Pathology | Primary Surgical Indications | Relative & Absolute Contraindications |
|---|---|---|
| LHB Displacement | - Medial dislocation with subscapularis tear - "Hourglass" biceps with mechanical catching - >25% structural tearing of the LHB substance - Failed conservative management > 3 months |
- Asymptomatic incidental finding on MRI - Active glenohumeral joint infection - Severe adhesive capsulitis (requires release first) - Patient inability to comply with postoperative restrictions |
| PTT Displacement | - Acute traumatic anterior dislocation - Chronic recurrent snapping with active dorsiflexion - MRI-confirmed longitudinal split tears of the PTT - Dysplastic/shallow retromalleolar groove |
- Rigid, fixed hindfoot valgus deformity - Severe peripheral vascular disease (poor healing) - Charcot neuroarthropathy - Active soft-tissue infection in the medial ankle |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful surgical outcomes in tendon displacement surgery. For LHB pathology, standard radiographic series (AP, true AP/Grashey, axillary, and scapular Y views) are obtained to rule out concurrent osseous pathology, such as proximal humerus fractures or advanced glenohumeral osteoarthritis. Magnetic Resonance Imaging (MRI) without contrast is the gold standard for evaluating the biceps pulley, the integrity of the LHB, and the status of the rotator cuff. The axial MRI sequences are scrutinized specifically to identify the position of the LHB relative to the bicipital groove and to evaluate the upper border of the subscapularis. Dynamic ultrasound is an excellent adjunctive tool, allowing the surgeon to visualize real-time medial subluxation during active internal and external rotation of the shoulder.
For PTT displacement, weight-bearing radiographs of the foot and ankle are mandatory to assess the medial longitudinal arch and rule out secondary deformities. An axial Computed Tomography (CT) scan is highly recommended to precisely quantify the depth and morphology of the retromalleolar groove, which dictates the necessity and extent of osseous groove deepening. MRI is utilized to assess the structural integrity of the flexor retinaculum and to identify longitudinal split tears within the PTT substance. Templating for PTT surgery involves selecting appropriate high-speed burrs (typically 3.0 mm or 4.0 mm round burrs) for groove deepening and ensuring the availability of micro-suture anchors if the native retinaculum is insufficient for transosseous repair.
Patient positioning must be meticulously executed to optimize surgical exposure and ensure patient safety. For LHB tenodesis (whether performed via an anterior deltopectoral approach or an anterosuperior mini-open approach), the patient is typically placed in the beach-chair position at approximately 45 to 60 degrees of elevation. General anesthesia is routinely supplemented with an ultrasound-guided interscalene regional block to minimize intraoperative volatile anesthetic requirements and optimize postoperative pain control. The operative arm is prepped and draped free, allowing for dynamic manipulation, which is critical for evaluating tendon tension and ensuring the tenodesis is set at the appropriate physiological resting length.
For PTT reconstruction, the patient is placed in the supine position. A crucial positioning pearl is to place a substantial bump under the ipsilateral hip (or contralateral hip, depending on the natural resting rotation of the patient's limb) to externally rotate the operative leg, thereby bringing the medial malleolus directly into the surgeon's line of sight. A pneumatic thigh tourniquet is applied to provide a bloodless surgical field, which is essential for identifying the delicate retinacular structures and the posterior tibial neurovascular bundle. The limb is prepped and draped above the knee, and a sterile bump is placed under the calf to allow free manipulation of the ankle joint throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
LHB Subpectoral Tenodesis Technique
In cases of LHB displacement, particularly when accompanied by chronic tendinosis or partial tearing, a subpectoral tenodesis is the preferred definitive management. This approach removes the diseased tendon entirely from the inflammatory environment of the bicipital groove. The procedure begins with a diagnostic arthroscopy to evaluate the glenohumeral joint, confirm the subscapularis pathology, and perform an arthroscopic tenotomy of the LHB at its superior labral origin. Once the tendon is released, it retracts distally into the bicipital groove.
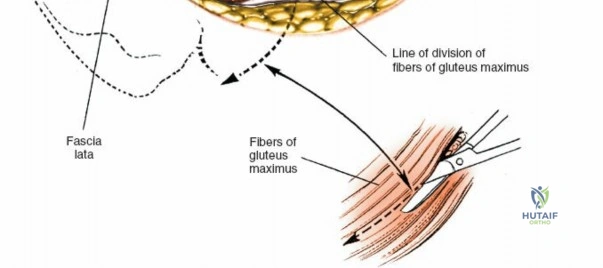
The open portion of the procedure utilizes a 3-4 cm longitudinal incision centered over the inferior border of the pectoralis major tendon, approximately 1 cm proximal to the axillary fold. The subcutaneous tissues are sharply dissected, and the fascia overlying the short head of the biceps and coracobrachialis is incised. Blunt finger dissection is used to sweep laterally, identifying the inferior border of the pectoralis major. A blunt retractor is placed superiorly under the pectoralis major to protect the neurovascular structures. The long head of the biceps tendon is identified within the bicipital groove just proximal to the pectoralis insertion. It is retrieved using a right-angle clamp and externalized. The diseased proximal portion of the tendon is sharply resected.
The proximal stump of the healthy tendon is then whipstitched using a #2 high-tensile non-absorbable suture. The cortical bone at the base of the bicipital groove, approximately 1 cm distal to the superior border of the pectoralis major, is decorticated. A guide pin is placed perpendicularly into the humeral shaft, and a unicortical socket is reamed to match the measured diameter of the tendon (typically 7 to 8 mm). The whipstitched tendon is then tensioned appropriately—ensuring the musculotendinous junction rests at the inferior border of the pectoralis major—and secured into the socket using a bio-composite interference screw. The fixation is tested by cycling the elbow through a full range of motion, ensuring no pistoning occurs at the tenodesis site.
PTT Retinacular Reconstruction and Groove Deepening
Operative intervention for PTT dislocation requires a dual approach: addressing the osseous dysplasia of the retromalleolar groove and reconstructing the incompetent flexor retinaculum. A 6-8 cm curvilinear incision is made posterior to the medial malleolus, carefully following the anatomical course of the PTT. Extreme care is taken during the subcutaneous dissection to identify and protect the saphenous vein and nerve anteriorly, as well as the posterior tibial neurovascular bundle located posterolaterally to the tendon. The attenuated flexor retinaculum is identified and incised longitudinally, leaving a 2-3 mm cuff of tissue on the medial malleolus to facilitate subsequent repair.
The PTT is externalized and meticulously inspected. Any degenerative, hypertrophic tenosynovium is debrided. If longitudinal split tears are identified, they are sharply debrided and tubularized using a running 5-0 non-absorbable monofilament suture to restore the tendon's cylindrical morphology. Attention is then turned to the medial malleolus. A sharp periosteal elevator is used to raise a thick, continuous periosteal flap from the posterior aspect of the malleolus. Using a high-speed 4.0 mm round burr with continuous saline irrigation to prevent thermal necrosis, the retromalleolar groove is deepened by 3 to 5 millimeters. Alternatively, a cortical trapdoor technique can be employed, where a rectangular osteotome is used to elevate the cortical roof, the underlying cancellous bone is impacted, and the roof is tamped back down to preserve the native fibrocartilaginous gliding surface.
Once the groove is adequately deepened, the PTT is relocated into its anatomical position. The ankle is brought through a full range of motion to ensure the tendon no longer subluxates during forced dorsiflexion and inversion. The flexor retinaculum is then repaired tightly over the tendon using heavy #0 non-absorbable sutures. If the native retinaculum is severely deficient or irreparably attenuated, the repair is augmented using a strip of local periosteum, a slip of the Achilles tendon, or suture anchors placed directly into the medial malleolus. The subcutaneous tissues are closed in a layered fashion to eliminate dead space, and the skin is approximated with tension-free mattress sutures to prevent wound breakdown in this critical watershed area.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for tendon displacement, while highly successful when executed correctly, carries a distinct profile of potential complications. The orthopedic surgeon must be intimately familiar with these risks, properly counsel the patient pre-operatively, and possess the technical armamentarium to execute salvage procedures when necessary. Complications can be broadly categorized into neurovascular injuries, failure of fixation, cosmetic deformities, and chronic pain syndromes.
In LHB tenodesis, the most visually apparent complication is the "Popeye" deformity, which occurs due to failure of the tenodesis fixation or improper tensioning of the tendon during the procedure. While largely a cosmetic issue, it can be associated with subjective cramping in the biceps muscle belly during sustained elbow flexion. A more severe, albeit rare, complication is iatrogenic injury to the axillary nerve. This typically occurs during an anterosuperior approach if the deltoid split is extended more than 5 cm distal to the acromion. Additionally, the creation of a unicortical socket in the proximal humerus creates a stress riser; if the socket is over-reamed or placed too distal, it can precipitate a spiral fracture of the proximal humerus, particularly in osteoporotic patients.
In PTT reconstruction, the most common complication is recurrent subluxation, which almost universally results from inadequate deepening of the retromalleolar groove or failure to address a concomitant severe hindfoot valgus deformity. Iatrogenic injury to the saphenous nerve or the posterior tibial nerve can result in debilitating neuromas or complex regional pain syndrome (CRPS). Wound dehiscence is a significant concern due to the tenuous vascular supply of the medial ankle skin flap. Furthermore, over-tightening of the flexor retinaculum during repair can lead to stenosing tenosynovitis, restricting tendon excursion and causing severe pain during the stance phase of gait.
| Complication | Estimated Incidence | Pathophysiology & Presentation | Salvage Strategy & Management |
|---|---|---|---|
| LHB "Popeye" Deformity | 2% - 5% | Failure of interference screw fixation or overtensioning. Presents as a distal bulge of the biceps muscle belly. | Often observed if asymptomatic. If severe cramping occurs, revision open subpectoral tenodesis is required. |
| Proximal Humerus Fracture | < 1% | Stress riser created by the tenodesis socket, usually in osteoporotic bone or if reamed >8mm. | Open reduction and internal fixation (ORIF) with a locking compression plate; bypass the socket. |
| PTT Recurrent Subluxation | 3% - 7% | Inadequate groove deepening or unrecognized hindfoot valgus. Presents with recurrent snapping. | Revision surgery: deeper osseous trough creation, robust retinacular augmentation, and medializing calcaneal osteotomy if valgus is present. |
| PTT Stenosing Tenosynovitis | 4% - 6% | Over-tightening of the flexor retinaculum repair. Presents with severe pain on active inversion and reduced excursion. | Aggressive physical therapy. If refractory, surgical release/lengthening of the flexor retinaculum is indicated. |
Phased Post-Operative Rehabilitation Protocols
The success of operative management for tendon displacement is inextricably linked to strict adherence to a phased, biologically sound postoperative rehabilitation protocol. The primary goal of rehabilitation is to protect the surgical repair during the initial phases of soft-tissue and tendon-to-bone healing, followed by a progressive restoration of range of motion, proprioception, and muscular strength.
LHB Tenodesis Rehabilitation
- Phase I: Maximal Protection (Weeks 0-4): The patient is placed in a standard shoulder sling. The primary objective is to protect the tenodesis site while preventing adhesive capsulitis. Passive range of motion (PROM) for the glenohumeral joint is initiated immediately. However, active elbow flexion and active forearm supination are strictly prohibited, as these motions place direct tensile stress on the healing biceps tendon. Pendulum exercises and passive forward elevation are encouraged.
- Phase II: Moderate Protection and Active Motion (Weeks 4-8): The sling is discontinued. The patient transitions to active-assisted range of motion (AAROM) and eventually active range of motion (AROM) for the shoulder and elbow. Gentle, submaximal isometric exercises for the biceps and rotator cuff are initiated. Terminal stretching is avoided to prevent over-lengthening of the tenodesis.
- Phase III: Strengthening and Return to Activity (Weeks 8-16): Progressive resistive exercises (PREs) are incorporated. Isotonic strengthening of the biceps, rotator cuff, and periscapular stabilizers is the focus. Return to heavy lifting or overhead sports is typically permitted between 3 to 4 months, contingent upon the patient demonstrating symmetrical strength on isokinetic dynamometry and a pain-free full range of motion. Note: If a concurrent rotator cuff repair was performed, the rehabilitation timeline is dictated entirely by the cuff repair, often delaying active shoulder motion for 6 weeks.
PTT Relocation Rehabilitation
- Phase I: Immobilization and Healing (Weeks 0-4): The patient is placed in a well-padded, non-weight-bearing short leg cast. The ankle is immobilized in slight plantarflexion and inversion. This specific positioning is critical as it removes all tensile stress from the repaired flexor retinaculum and the relocated PTT, allowing the soft tissues to heal without mechanical disruption.
- Phase II: Transitional Weight-Bearing (Weeks 4-8): The cast is removed, and the patient is transitioned to a controlled ankle motion (CAM) boot. Weight-bearing is gradually advanced by 25% increments weekly. Gentle, active range of motion is initiated out of the boot, but forced dorsiflexion and active eversion are strictly avoided. Cross-friction massage of the medial ankle incision is performed to prevent deep scar tissue adhesions.
- Phase III: Functional Restoration (Weeks 8-16+): Formal physical therapy commences. The CAM boot is weaned, and the patient transitions to an orthotic-supported shoe. Rehabilitation focuses heavily on PTT eccentric loading, closed-kinetic-chain exercises, and proprioceptive training on unstable surfaces (e.g., BAPS board). Return to high-impact sports or pre-injury activity levels is typically achieved by 4 to 6 months, provided there is no recurrent subluxation and the patient demonstrates normal, pain-free gait mechanics.
Summary of Landmark Literature and Clinical Guidelines
The operative management of tendon displacement is supported by a robust foundation of biomechanical research and long-term clinical outcome studies. Mastery of this literature is essential for the academic orthopedic surgeon to justify surgical indications and optimize operative techniques.
In the realm of long head of the biceps pathology, the landmark biomechanical studies by Werner et al. fundamentally redefined our understanding of the biceps pulley. By demonstrating that the superior glenohumeral ligament and coracohumeral ligament are the primary restraints to medial subluxation, they effectively rendered the historical repair of the transverse humeral ligament obsolete. Furthermore, the extensive clinical trials by Boileau et al. provided the definitive classification system for LHB lesions and established the modern consensus that subpectoral tenodesis provides superior cosmetic and functional outcomes compared to simple tenotomy, particularly in active patients under the age of 60. Current American Academy of Orthopaedic Surgeons (AAOS) guidelines strongly recommend tenodesis over tenotomy in high-demand laborers and athletes to preserve elbow flexion and supination endurance.
Regarding posterior tibial tendon dislocation, the seminal paper by Ouzounian and Myerson remains the definitive text on the subject. Their comprehensive review of recurrent subluxation highlighted that soft-tissue repair alone is associated with unacceptably high failure rates. They established the surgical paradigm that successful outcomes mandate addressing the underlying bony morphology through retromalleolar groove deepening. Subsequent long-term outcome studies by the American Orthopaedic Foot & Ankle Society (AOFAS) have validated this approach, demonstrating high rates of return to sport and near-zero recurrence rates when groove deepening is combined with robust retinacular reconstruction.
Finally, the literature emphasizes the critical importance of differential diagnosis, particularly in the setting of acute trauma or exercise-induced pain. The foundational work by Rorabeck, Mubarak, and Whitesides on Chronic Exertional Compartment Syndrome (CECS) serves as a vital clinical caveat. Medial leg pain mimicking PTT pathology must be rigorously evaluated; if CECS is confirmed via intracompartmental pressure monitoring, isolated tendon surgery is contraindicated, and definitive fasciotomy is required. This synthesis of biomechanical principles, landmark clinical trials, and rigorous diagnostic criteria forms the bedrock of modern orthopedic management for tendon displacement.
