Paralytic Hand: Principles of Tendon Transfer and Surgical Reconstruction

Key Takeaway
The surgical rehabilitation of the paralytic hand requires a profound understanding of hand biomechanics, precise timing, and meticulous tendon transfer techniques. This guide details the evaluation of muscle imbalance, correction of claw deformities, and evidence-based protocols for restoring pinch, opposition, and intrinsic function following peripheral nerve injuries, tetraplegia, or systemic neuromuscular diseases.
Comprehensive Introduction and Patho-Epidemiology
The paralytic hand represents one of the most profound reconstructive challenges in orthopedic and hand surgery. It is characterized by a complex interplay of dynamic muscle imbalance, loss of motor function, and often, debilitating sensory deficits. The fundamental pathophysiology revolves around the disruption of the delicate equilibrium between the extrinsic musculature (originating in the forearm) and the intrinsic musculature (originating within the hand). When normal antagonistic muscle tension is lost due to denervation, the unopposed functioning muscles gradually drive the hand into fixed, non-functional, and often grotesque postures. If left unaddressed, dynamic deformities inevitably progress to rigid myostatic contractures and secondary joint capsular stiffness.
The etiology of the paralytic hand is diverse, encompassing peripheral nerve trauma, brachial plexus injuries, spinal cord injuries (tetraplegia), and a variety of systemic or neurodegenerative diseases. Peripheral nerve injuries are the most common cause in the trauma setting, with radial, median, and ulnar nerve palsies each presenting distinct, predictable patterns of deformity. For instance, isolated radial nerve palsy yields a profound drop wrist and inability to extend the digits, whereas combined median and ulnar nerve lesions result in a catastrophic "intrinsic-minus" hand, devoid of pinch, grip, and opposition. Epidemiologically, penetrating trauma, traction injuries, and fractures (such as the classic Holstein-Lewis humeral shaft fracture) account for the majority of peripheral nerve deficits encountered by the upper extremity surgeon.
Sensation in the paralytic hand varies significantly according to the underlying etiology, dictating both the surgical approach and the ultimate functional prognosis. In poliomyelitis, an anterior horn cell disease, motor paralysis is present, but sensation remains entirely normal, allowing for excellent postoperative motor re-education. Conversely, peripheral nerve lesions present with sensory deficits that follow specific dermatomal or autonomous nerve distributions depending on the level and severity of the nerve lesion. In Hansen Disease (Leprosy), a major cause of paralytic hand globally, sensation is typically absent in a progressive, glove-like distribution, predisposing the patient to repetitive microtrauma and subsequent digit resorption. Syringomyelia presents a unique challenge; patients exhibit a dissociated sensory loss (loss of pain and temperature sensation with preserved fine touch and proprioception), which requires meticulous patient education to prevent postoperative thermal injuries.
Furthermore, it is critical to distinguish between flaccid paralysis (lower motor neuron lesions) and spastic paralysis (upper motor neuron lesions, such as cerebral palsy or stroke). Upper motor neuron lesions introduce muscle spasticity, which disrupts hand balance because the tension of spastic muscles cannot be effectively controlled or balanced by opposing normal muscles. Tendon transfers in the spastic hand require entirely different biomechanical considerations, often prioritizing the release of spastic contractures and the augmentation of weakened antagonists, compared to the reconstructive paradigm of the flaccid paralytic hand.
Detailed Surgical Anatomy and Biomechanics
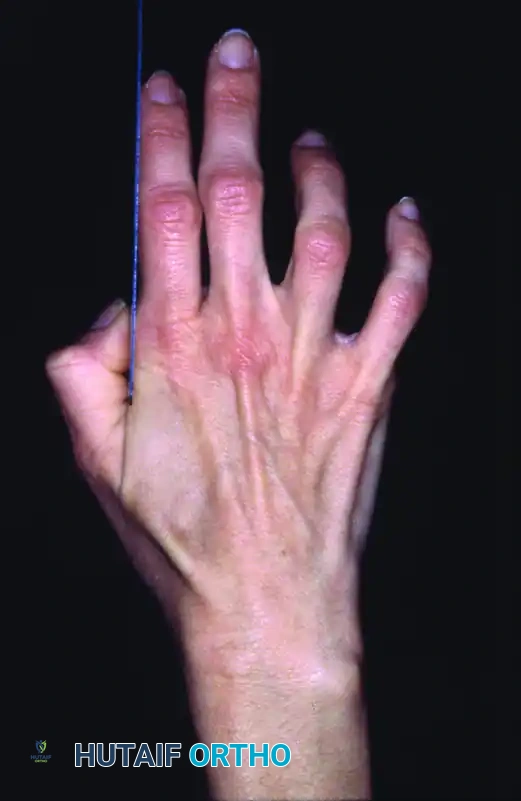
A profound understanding of hand biomechanics is the bedrock of successful tendon transfer surgery. The hand operates through a highly synchronized system of intercalated joints controlled by a multi-articular tendon system. The most iconic presentation of intrinsic muscle paralysis is the "claw hand" (intrinsic-minus posture). This deformity is a direct result of the disruption of the delicate balance between the extrinsic and intrinsic musculature of the hand.

In a normal hand, the intrinsic muscles (lumbricals and interossei) are responsible for flexing the metacarpophalangeal (MCP) joints and extending the proximal and distal interphalangeal (PIP and DIP) joints via their insertion into the lateral bands of the extensor mechanism. When these intrinsic muscles are paralyzed, typically due to ulnar or combined ulnar/median nerve palsy, the extrinsic extensor digitorum communis (EDC) acts unopposed at the MCP joint, driving it into hyperextension.
Concurrently, the extrinsic flexors (flexor digitorum superficialis [FDS] and flexor digitorum profundus [FDP]) act unopposed at the IP joints, pulling them into acute flexion. The hyperextension of the MCP joint alters the moment arm of the EDC, effectively dissipating its excursion and rendering it mechanically incapable of extending the PIP and DIP joints.
This mechanical dependency is classically described by the Bouvier Principle. The long finger extensors are mechanically capable of extending the interphalangeal joints only if the hyperextension of the metacarpophalangeal joints is prevented. If the MCP joint is allowed to hyperextend, the EDC tendon bowstrings dorsally, losing its mechanical advantage to extend the PIP and DIP joints.

This biomechanical phenomenon is the foundation of the Bouvier test, a critical component of the preoperative physical examination. When the examiner manually blocks the MCP joints from hyperextending (simulating intrinsic muscle function), the patient is asked to actively extend their fingers. If the patient's extrinsic extensors can successfully extend the IP joints, the test is positive. A positive Bouvier test indicates that the extensor apparatus is intact and a simple MCP joint stabilization procedure (such as a Zancolli lasso, capsulodesis, or bone-block operation) will correct the clawing.
If IP extension is not achieved despite MCP stabilization (a negative Bouvier test), the central slip and lateral bands of the extensor apparatus are attenuated or non-functional. In this scenario, simply blocking the MCP joint is insufficient; a dynamic tendon transfer routed directly to the lateral bands (such as a modified Stiles-Bunnell or Brand transfer) is required to actively restore PIP and DIP extension.
Beyond the claw deformity, the surgeon must intimately understand the concepts of muscle excursion (amplitude) and the length-tension relationship (the Blix curve). Muscle excursion is proportional to fiber length. Wrist flexors and extensors have an excursion of approximately 33 mm, finger extensors 50 mm, and finger flexors 70 mm. A wrist flexor cannot fully substitute for a finger flexor based on absolute excursion alone. However, the effective excursion can be augmented by the tenodesis effect of the wrist. By allowing the wrist to extend during finger flexion, the functional amplitude of a transferred wrist flexor is increased, allowing it to achieve full digital flexion.
Exhaustive Indications and Contraindications
The decision to proceed with tendon transfer surgery must be meticulously weighed. Tendon transfer is the final, definitive step in the rehabilitation of the paralytic hand. To achieve predictable, functional outcomes, the surgeon must adhere strictly to established indications and recognize absolute contraindications.
Indications for Tendon Transfer
The primary indication for tendon transfer is the permanent loss of motor function where nerve repair or grafting is impossible, has failed, or has reached its maximum potential without functional recovery. Tendon transfers are also indicated as "internal splints" in cases where nerve recovery is anticipated but prolonged (e.g., high radial nerve palsy). Early transfer of the pronator teres to the extensor carpi radialis brevis (ECRB) immediately restores wrist extension, eliminating the need for cumbersome external orthoses, improving grip strength via the tenodesis effect, and preventing flexion contractures of the wrist while awaiting radial nerve regeneration.
Contraindications to Tendon Transfer
Attempting a tendon transfer across a stiff joint or through a scarred soft-tissue bed is a recipe for failure. The transferred tendon provides dynamic motor power; it cannot overcome fixed joint contractures. A satisfactory range of passive joint motion is an absolute prerequisite. Furthermore, progressive neurological disorders require cautious consideration, as the donor muscle itself may eventually succumb to the disease process.
| Parameter | Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Neurological Status | Permanent, irreversible nerve injury; Delayed presentation of nerve injury (>18 months) | Acute injury where primary nerve repair is feasible and timely | Progressive neuromuscular disease (e.g., ALS, severe CMT) |
| Joint Mobility | Full, supple passive range of motion (PROM) equal to desired active ROM | Fixed joint contractures; Severe arthrofibrosis | Mild, correctable capsular stiffness |
| Soft Tissue Bed | Healthy, vascularized, pliable subcutaneous tissue | Dense scar tissue; Exposed avascular bone or hardware | Previous severe crush injury requiring flap coverage |
| Donor Muscle | MRC Grade 4 or 5 strength; Expendable function; Adequate excursion | MRC Grade 3 or less; Non-expendable muscle (e.g., sole remaining wrist flexor) | Spastic donor muscle (requires specific modifications) |
| Patient Factors | Compliant, motivated, capable of complex motor re-education | Severe cognitive impairment; Unwillingness to participate in therapy | Advanced age with low functional demands |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for tendon transfers is an intellectual exercise requiring a comprehensive inventory of functioning muscles, joint mobility, and soft tissue integrity. The timing of surgical intervention is critical and varies fundamentally based on the etiology of the paralysis.
In peripheral nerve injuries, definitive transfers should generally be delayed to allow for nerve regeneration following neurorrhaphy. Nerve regeneration occurs at a rate of approximately 1 mm per day. In a high median nerve lesion, clinical signs of reinnervation in the proximal muscles (e.g., pronator teres) should be evident within 4 months. If no clinical or electromyographic (EMG) evidence of recovery is present within the calculated timeframe, tendon transfers should be executed. Conversely, in poliomyelitis, spontaneous recovery can occur for up to 18 months; therefore, definitive transfers are delayed until this period has elapsed and the neurological deficit is stable.
Donor Muscle Selection Principles
The selection of the donor muscle must adhere to the classic principles popularized by Boyes, Brand, and Smith:
1. Strength: A muscle loses approximately one grade of strength (on the MRC 0-5 scale) following transfer. Therefore, only muscles with a preoperative strength of Grade 4 or 5 should be selected.
2. Excursion: The excursion of the donor tendon must closely match the physiological requirement of the paralyzed muscle (the 33/50/70 mm rule).
3. Synergy: Muscles that normally work together (e.g., wrist extensors and finger flexors) are easier for the patient to consciously control postoperatively. Synergistic transfers require significantly less cortical re-education.
4. Straight Line of Pull: The transferred tendon should be routed in the straightest possible line between its origin and new insertion. Acute angles increase friction, reduce mechanical efficiency, and predispose to rupture or adherence.
5. Expendability: The removal of the donor muscle must not create an unacceptable secondary functional deficit. For example, the flexor carpi radialis (FCR) is highly expendable, whereas the flexor carpi ulnaris (FCU) is the primary power flexor of the wrist and should be preserved if possible.
Patient Positioning and Preparation
The patient is positioned supine with the operative arm extended on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (brachial plexus block) is highly preferred, as it provides excellent intraoperative analgesia and profound sympathetic block, which aids in peripheral perfusion. However, if intraoperative patient cooperation is desired for tensioning (the "wide-awake local anesthesia no tourniquet" or WALANT technique), local infiltration with lidocaine and epinephrine is utilized. The surgeon must use loupe magnification (minimum 2.5x to 3.5x) for meticulous handling of the paratenon and precise execution of the tendon weave.
Step-by-Step Surgical Approach and Fixation Technique
Surgical execution of a tendon transfer demands meticulous soft-tissue handling to prevent postoperative adhesions. The fundamental goal is the restoration of tissue equilibrium. A transferred tendon must glide freely to function; it cannot be routed through dense scar tissue or placed directly over raw bone.
Incisions and Tendon Routing
Incisions must be planned to avoid crossing the path of the transferred tendon at a right angle, which can cause bowstringing or restrictive adhesions. Brunner-type zigzag incisions or mid-axial incisions are preferred in the digits, while longitudinal or gently curved incisions are used in the forearm. The optimal route for a transferred tendon is through the healthy subcutaneous fat layer. Routing tendons through fascial windows or the interosseous membrane (e.g., in median nerve palsy transfers) increases the risk of adhesions. If an interosseous route is necessary, a wide window must be excised in the interosseous membrane to prevent tethering.
The Pulvertaft Weave
The gold standard for tendon coaptation in transfers is the Pulvertaft weave. This technique provides immense immediate biomechanical strength, preventing gap formation and allowing for early active mobilization protocols without the risk of rupture.
1. The recipient tendon is split longitudinally with a #11 blade in the center of its substance.
2. The donor tendon is passed through the split using a tendon passer or curved hemostat.
3. The recipient tendon is split again, 5 to 10 mm distal to the first split, rotated 90 degrees to the original axis.
4. The donor tendon is passed through this second split.
5. This process is repeated for a minimum of three to four passes, alternating the axis of the split by 90 degrees each time.
6. Once the desired tension is set, each pass is secured with a figure-of-eight or mattress suture using a 3-0 or 4-0 non-absorbable braided suture (e.g., Ethibond or FiberWire). The ends of the tendons are buried or tapered to ensure smooth gliding.
Tensioning the Transfer
Setting the correct tension is arguably the most difficult, subjective, and critical step of the operation. The muscle must be tensioned at its optimal resting length to maximize the number of actin-myosin cross-bridges—the peak of the Blix curve.
* If tensioned too loosely, the muscle will expend its entire excursion simply taking up the slack, resulting in no joint movement.
* If tensioned too tightly, the muscle will undergo ischemic necrosis or permanent stretch-induced weakness, and the antagonistic joint motion will be restricted.
As a general rule, the transfer is tensioned such that the resting posture of the hand mimics the normal physiological cascade when the wrist is in neutral. For example, when transferring the FCR to the EDC for radial nerve palsy, the tension is set so that with the wrist in neutral, the MCP joints are held in 0 to 10 degrees of extension. The tenodesis effect is then tested intraoperatively: passive flexion of the wrist should cause automatic extension of the digits, and passive extension of the wrist should allow full, unhindered passive flexion of the digits into the palm.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, complications in tendon transfer surgery can occur and often require complex salvage procedures. The most common cause of failure is improper indication, specifically attempting a transfer in the presence of fixed joint contractures.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| Tendon Adhesions | 10 - 15% | Routing through scar; Prolonged immobilization; Poor paratenon handling | Prevention: Subcutaneous routing; Early active motion. Salvage: Tenolysis after 6 months of plateaued therapy. |
| Transfer Rupture | 1 - 3% | Inadequate weave (e.g., end-to-end instead of Pulvertaft); Non-compliant patient | Prevention: Minimum 3-pass Pulvertaft weave; Strict orthosis use. Salvage: Re-exploration, debridement, and revision transfer or grafting. |
| Over-tensioning (Minus Deformity) | 5 - 10% | Securing transfer under maximal stretch; Failure to account for tenodesis effect | Prevention: Tension at resting cascade; Check intraoperative tenodesis. Salvage: Z-lengthening of the transferred tendon. |
| Under-tensioning (Extensor/Flexor Lag) | 10 - 20% | Securing transfer too loosely; Stretching of the weave during rehab | Prevention: Slightly over-tension at surgery to account for physiological relaxation. Salvage: Tendon plication or advancement. |
| Joint Stiffness / Contracture | 5 - 15% | Pre-existing stiffness; Failure to mobilize antagonist joints | Prevention: Preoperative therapy to achieve full passive ROM. Salvage: Intensive therapy, serial casting, or surgical capsulotomy. |
| Complex Regional Pain Syndrome (CRPS) | 2 - 5% | Undue nerve traction; Poor pain control; Psychological factors | Prevention: Meticulous hemostasis; Avoid tight casts; Vitamin C prophylaxis. Salvage: Aggressive therapy, gabapentinoids, sympathetic blocks. |
Phased Post-Operative Rehabilitation Protocols
The success of a tendon transfer relies as much on the postoperative rehabilitation as it does on the surgical execution. A poorly rehabilitated, perfectly executed transfer will yield a suboptimal functional result. The rehabilitation protocol must be tailored to the specific transfer, the strength of the fixation, and the patient's cognitive capacity.
Phase I: Immobilization (0 to 3-4 Weeks)
Immediately postoperatively, the limb is immobilized in a rigid cast or a custom thermoplastic orthosis. The joints are positioned to remove all tension from the tendon anastomosis. For example, following a standard radial nerve tendon transfer (e.g., FCR to EDC, PT to ECRB, PL to EPL), the wrist is immobilized in 40 to 45 degrees of extension, the MCP joints in neutral (0 degrees), and the thumb in maximal radial abduction and extension. Elevation and strict edema control are paramount during this phase to prevent fibrotic induration of the soft tissues.
Phase II: Early Active Mobilization (3-4 to 6 Weeks)
At 3 to 4 weeks, the cast is removed, and a removable protective splint is fabricated. The patient begins supervised, gravity-eliminated active range of motion. The primary goal of this phase is motor re-education and the prevention of adhesions.
* Motor Re-education: Cortical plasticity is essential. The patient is instructed to perform the original action of the donor muscle to achieve the new action. For instance, if the Pronator Teres was transferred to the ECRB, the patient is asked to forcefully pronate the forearm against isometric resistance, which will now result in wrist extension. Biofeedback, functional electrical stimulation (FES), and mirror therapy are highly effective adjuncts during this phase to facilitate cortical remapping.
* Passive stretching of the transfer is strictly prohibited during this phase to prevent elongation or rupture of the healing Pulvertaft weave.
Phase III: Strengthening and Integration (6 to 12 Weeks)
By 6 weeks, the tendon healing is robust enough to withstand gentle passive stretching to overcome any mild antagonist contractures. Progressive resistance exercises are initiated using putty, hand grippers, and weighted activities. The protective splint is gradually weaned during the day but may be worn at night until 8 to 10 weeks postoperatively to prevent inadvertent stretch during sleep.
Full integration of the transfer into subconscious, spontaneous hand use is the ultimate goal. This requires extensive occupational therapy focusing on activities of daily living (ADLs), fine motor dexterity, and grip strength. Maximum functional improvement may take 6 to 12 months, as the central nervous system slowly adapts to the altered biomechanical pathways.
Summary of Landmark Literature and Clinical Guidelines
The principles of tendon transfer for the paralytic hand have evolved over a century, built upon the foundational work of surgical pioneers. Paul Brand’s extensive work with Hansen's disease patients in India established the fundamental biomechanical principles of muscle excursion, tensioning, and the critical importance of a supple soft-tissue bed. His text, Clinical Mechanics of the Hand, remains mandatory reading for any reconstructive surgeon.
Joseph Boyes expanded on these principles, particularly in the management of radial nerve palsy, advocating for the superficialis transfer to restore finger extension. Eduardo Zancolli revolutionized the understanding of the intrinsic-minus hand, detailing the biomechanics of the claw deformity and introducing the "lasso" procedure for MCP joint stabilization, drastically simplifying the surgical management of ulnar nerve palsy.
Modern clinical guidelines, supported by the American Society for Surgery of the Hand (ASSH) and the American Academy of Orthopaedic Surgeons (AAOS), emphasize a multidisciplinary approach. Preoperative optimization of joint mobility, precise intraoperative execution using the Pulvertaft weave, and structured, phased postoperative therapy are universally recognized as the triad of success in paralytic hand reconstruction.
📚 Medical References
- paralytic hand, J Bone Joint Surg 57A:730, 1975.
- Brown PW: Zancolli capsulorrhaphy for ulnar claw hand: appraisal of forty-four cases, J Bone Joint Surg 52A:868, 1970.
- Brown PW: Reconstruction for pinch in ulnar intrinsic palsy, Orthop Clin North Am 2:323, 1974.
- Bruner JM: Tendon transfer to restore abduction of the
