Mastering Patella Tendon Repair: An Intraoperative Guide to Acute and Chronic Ruptures
Key Takeaway
This masterclass guides fellows through the intricacies of patella tendon repair. We cover comprehensive surgical anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative techniques for both acute and chronic ruptures. Emphasis is placed on precise instrument use, critical decision-making, and advanced augmentation strategies. We also delve into potential pitfalls, their salvage, and comprehensive postoperative care protocols to ensure optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Disruption of the extensor mechanism via patella tendon rupture represents a catastrophic biomechanical failure of the knee joint, rendering the patient unable to actively extend the lower extremity or maintain stability during the stance phase of gait. While statistically less common than quadriceps tendon ruptures, patella tendon ruptures present a unique set of surgical challenges due to the limited local tissue available for mobilization and the critical need to restore precise patellar kinematics. The injury typically exhibits a bimodal demographic distribution. We most frequently encounter this in athletic patients under the age of forty who experience a sudden, violent eccentric contraction of the quadriceps muscle against a fixed, flexed knee—such as landing from a jump or rapidly decelerating. A secondary peak occurs in older populations or those with underlying systemic comorbidities that compromise collagen integrity and tendon architecture.
Understanding the underlying pathogenesis is essential for both surgical planning and managing patient expectations. Healthy patella tendons rarely rupture under physiologic loads; biomechanical studies suggest a force of up to 17.5 times body weight is required to fail a healthy extensor mechanism. Therefore, the vast majority of these injuries occur in the setting of pre-existing, often asymptomatic, tendinosis. This degenerative cascade is characterized by myxoid degeneration, fibrinoid necrosis, and a loss of the normal parallel orientation of type I collagen fibers. Microvascular compromise within the tendon substance further exacerbates this structural weakening, creating a biomechanical environment primed for catastrophic failure under sudden load.
Systemic factors play a profound role in the epidemiology of this injury. Chronic systemic corticosteroid use is perhaps the most notorious culprit, directly inhibiting collagen synthesis and altering the biomechanical properties of the tendon. End-stage renal disease, particularly in patients undergoing long-term hemodialysis, leads to secondary hyperparathyroidism and amyloid deposition within the tendon substance, drastically reducing its tensile strength. Furthermore, the use of fluoroquinolone antibiotics has been definitively linked to tendinopathy and acute rupture due to their direct cytotoxic effects on tenocytes and disruption of the extracellular matrix. Recognizing these predisposing factors is critical, as they not only increase the risk of contralateral rupture but also significantly compromise the healing potential of our surgical repair.
The clinical presentation of an acute complete rupture is usually unmistakable. Patients report a distinct "pop" or tearing sensation, followed by immediate, profound weakness and an inability to bear weight. The hallmark physical finding is a palpable defect in the infrapatellar region coupled with an absolute inability to perform a straight leg raise or maintain active knee extension against gravity. The patella is typically displaced proximally by the unopposed pull of the quadriceps muscle, a condition known as patella alta. It is imperative to perform a meticulous physical examination, as partial tears or injuries masked by massive hemarthrosis can occasionally be misdiagnosed, leading to delayed treatment, chronic retraction, and a vastly more complex reconstructive challenge.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the extensor mechanism's surgical anatomy is the foundation of a successful repair. The patella tendon is a remarkably robust, ligamentous-like structure that serves as the terminal linkage of the quadriceps muscle complex. In the average adult, it measures approximately 30 to 50 millimeters in length, 25 to 30 millimeters in width, and 5 to 7 millimeters in thickness. It originates from the inferior pole of the patella, where its fibers interdigitate deeply with the articular cartilage posteriorly and blend seamlessly with the thick periosteal layer anteriorly. This proximal footprint is the most frequent site of failure, often presenting as an avulsion with or without small osseous fragments. Distally, the tendon narrows slightly to insert onto the prominent tibial tubercle, fanning out to interweave with the local periosteum and the deep fascia of the leg.

The vascular supply to the patella tendon is a critical consideration, particularly regarding its healing capacity and the pathogenesis of rupture. The tendon receives its blood supply primarily from the inferior medial and inferior lateral genicular arteries, which form an anastomotic ring within the infrapatellar fat pad and the overlying peritenon. However, microangiographic studies have consistently demonstrated a relative "watershed" zone of hypovascularity in the proximal third of the tendon, just distal to the inferior pole of the patella. This tenuous vascularity not only explains why the majority of ruptures occur in this specific location but also underscores the absolute necessity of preserving the peritenon during our surgical dissection. The peritenon is a highly vascularized, cellular sheath that serves as the primary source of mesenchymal stem cells and neovascularization required for intrinsic tendon healing post-repair.
Neurologically, the anterior aspect of the knee is innervated by a complex arborization of cutaneous nerves, the most critical of which is the infrapatellar branch of the saphenous nerve (IPBSN). The IPBSN typically courses transversely across the proximal tibia and the distal aspect of the patella tendon, highly variable in its exact trajectory. During our standard anterior midline surgical approach, this nerve is at extreme risk of iatrogenic transection or traction injury. Damage to the IPBSN can result in a frustrating area of numbness over the anterolateral proximal tibia or, more severely, the formation of a painful neuroma that can significantly impede the patient's postoperative rehabilitation and overall satisfaction. Meticulous blunt dissection within the subcutaneous tissues is mandatory to identify and protect these neural branches whenever feasible.
Biomechanically, the patella tendon must withstand extraordinary forces. During normal level walking, the tendon experiences loads approximately 0.5 times body weight. However, during activities such as stair climbing, deep squatting, or athletic jumping, these forces escalate exponentially, reaching up to 7 to 8 times body weight. The patella functions as a dynamic fulcrum, increasing the moment arm of the quadriceps muscle and thereby maximizing the mechanical advantage of the extensor mechanism. A successful surgical repair must not only re-establish structural continuity but also precisely restore the anatomic length of the tendon. If the repair is tensioned too tightly (leading to patella baja), the resulting increased patellofemoral contact pressures will cause devastating early-onset arthrosis and restricted knee flexion. Conversely, if the repair is too loose (patella alta), the extensor mechanism will suffer an extensor lag, profound weakness, and potential patellar instability.
Exhaustive Indications and Contraindications
The management of patella tendon ruptures is overwhelmingly surgical. Non-operative management is reserved for an infinitesimally small subset of patients and requires strict adherence to specific criteria. For the vast majority of the population, a complete disruption of the extensor mechanism is an absolute indication for operative intervention to restore the ability to ambulate independently. The timing of the surgery is critical; acute repairs performed within the first two to three weeks yield vastly superior functional outcomes compared to delayed reconstructions. As time progresses, the quadriceps muscle undergoes contracture, the patella tendon stump retracts and degenerates, and the tissue planes become obliterated by dense, disorganized scar tissue, transforming a straightforward repair into a formidable reconstructive challenge.
Non-operative management may be considered in cases of truly partial tears where the patient retains the ability to actively extend the knee against gravity and perform a straight leg raise without extensor lag. In these rare instances, immobilization in full extension for 4 to 6 weeks, followed by a rigorously supervised, progressive rehabilitation program, may yield acceptable results. Furthermore, non-operative management is the unfortunate default for patients with absolute medical contraindications to surgery. This includes individuals with severe, unoptimized cardiopulmonary disease, active systemic infections, or profound baseline non-ambulatory status (e.g., severe advanced dementia or paraplegia) where the risks of anesthesia and surgical intervention far outweigh any theoretical functional benefit.
The distinction between an acute and chronic rupture fundamentally alters our surgical algorithm. Acute ruptures (typically defined as those presenting within 3 weeks of injury) are amenable to direct end-to-end primary repair or direct reattachment to bone. The tissue quality is generally sufficient to hold heavy non-absorbable sutures, and the quadriceps has not yet undergone irreversible contracture. Chronic ruptures (presenting beyond 4 to 6 weeks) represent a distinct pathologic entity. Direct repair is often impossible due to massive gap formation and profound tissue degeneration. These cases mandate complex reconstructive techniques, including V-Y quadricepsplasty to mobilize the patella, and augmentation with autograft (e.g., hamstring) or allograft (e.g., Achilles tendon with a bone block) to bridge the defect and provide structural integrity.
| Parameter | Indications for Surgical Intervention | Contraindications / Non-Operative Management |
|---|---|---|
| Complete Rupture (Acute) | Absolute indication. Inability to perform straight leg raise. Palpable defect. | Absolute medical contraindications to anesthesia. Baseline non-ambulatory status. |
| Complete Rupture (Chronic) | Severe extensor lag, instability, falls. Requires reconstruction/allograft. | Active overlying soft tissue infection. Severe, uncorrectable vascular compromise. |
| Partial Tear | Failure of conservative management. Persistent weakness or pain > 3-6 months. | Intact extensor mechanism (can do straight leg raise). Managed with bracing and PT. |
| Concomitant Injuries | Open ruptures (requires immediate I&D). Associated tibial plateau or patella fractures. | N/A - Open injuries or fractures with rupture mandate surgical stabilization. |
| Patient Factors | High-demand athletes, active adults, independent ambulators. | Severe dementia, non-compliance with post-op restrictions, active injection drug use. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the blueprint for surgical success. This begins with a comprehensive radiographic evaluation. Standard plain radiographs, including weight-bearing anteroposterior, true lateral, and Merchant (sunrise) views, are mandatory. The lateral radiograph is particularly crucial for assessing patellar height. We utilize established indices such as the Insall-Salvati ratio (ratio of patella tendon length to patella bone length, normally ~1.0) or the Caton-Deschamps index to objectively quantify the degree of patella alta. Radiographs will also reveal any associated avulsion fractures at the inferior pole of the patella or the tibial tubercle, which dictate our fixation strategy.
Magnetic Resonance Imaging (MRI) has become the gold standard for preoperative templating. A high-resolution, non-contrast MRI precisely delineates the exact location of the tear (proximal avulsion, midsubstance, or distal avulsion), quantifies the degree of tendon retraction, and assesses the quality of the remaining tissue. Furthermore, MRI is invaluable for identifying concomitant intra-articular pathology, such as meniscal tears or cruciate ligament disruptions, which occur in a significant percentage of high-energy traumatic ruptures. If a chronic reconstruction is anticipated based on imaging and clinical chronicity, the surgeon must proactively coordinate with the tissue bank to ensure the availability of appropriate allograft tissue, typically a fresh-frozen Achilles tendon allograft with a calcaneal bone block, or a robust tibialis anterior allograft.
In the operating room, patient positioning and setup must be executed with precision. The patient is placed in the supine position on a standard radiolucent operating table. A crucial, often overlooked step is the preparation and draping of both lower extremities. Prepping the contralateral, uninjured leg allows the surgeon to use it as an intraoperative template. By comparing the patellar height and the tension of the extensor mechanism on the uninjured side, we can accurately gauge the appropriate tensioning of our repair on the injured side, mitigating the risk of iatrogenic patella baja or alta. A sterile tourniquet is applied high on the operative thigh to ensure a bloodless field during the meticulous dissection and identification of the tendon ends.
The surgical equipment must be meticulously verified prior to incision. The scrub tech should have a standard orthopedic soft tissue tray, supplemented with heavy, non-absorbable braided sutures (e.g., No. 2 or No. 5 FiberWire or Ethibond). Depending on the anticipated tear location and the surgeon's preferred technique, a variety of fixation devices must be available. For proximal or distal avulsions, we frequently utilize double-loaded, vented biocomposite suture anchors (e.g., 4.75mm or 5.5mm). Alternatively, if transosseous tunnels are preferred, the appropriate drill bits, K-wires, and suture passers (such as a Hewson slider or Beath pins) must be on the sterile field. For chronic reconstructions, oscillating saws, osteotomes, and augmentation materials (such as Dall-Miles cables, Mersilene tape, or heavy PDS bands) are absolute requirements.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach utilizes a generous anterior midline longitudinal incision. The incision typically begins at the superior pole of the patella and extends distally over the midline of the patella tendon, terminating approximately 2 centimeters distal to the tibial tubercle. This extensile approach provides unhindered access to the entire extensor mechanism and allows for proximal extension if a quadriceps release becomes necessary.
Following the skin incision, dissection proceeds through the subcutaneous tissues. Extreme vigilance is required here to identify and protect the infrapatellar branches of the saphenous nerve. While complete preservation is not always possible given the trauma, careful blunt dissection and retraction can minimize iatrogenic neuroma formation. We then encounter the superficial infrapatellar bursa, which is often filled with organized hematoma and inflammatory debris; this should be excised to clearly visualize the underlying pathology. The peritenon is then identified. It is imperative to incise the peritenon longitudinally and meticulously peel it back as a distinct layer. Preserving the peritenon for an airtight closure at the end of the procedure is paramount, as it provides the essential vascular and cellular milieu for tendon healing.
Acute Midsubstance Tears
For tears occurring within the main body of the tendon, primary end-to-end repair is the standard of care. The initial step is rigorous debridement. The frayed, necrotic, and hematoma-infiltrated ends of both the proximal and distal tendon stumps must be sharply excised back to healthy, organized, and bleeding collagenous tissue. Failure to adequately debride compromised tissue will inevitably lead to suture pull-out and catastrophic repair failure. Once healthy margins are established, we proceed with core suture placement using heavy, non-absorbable braided suture (e.g., No. 2 FiberWire).

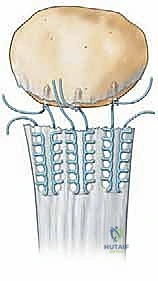
We advocate for the use of the Krackow locking stitch technique, which provides superior biomechanical pull-out strength compared to simple running or Kessler stitches. Two separate heavy sutures are used for each stump. Starting approximately 1.5 to 2.0 centimeters from the torn edge, the needle is passed through the tendon substance, looped around the tendon edge, and passed back through its own loop to create a locking mechanism. This is repeated 3 to 4 times along the medial and lateral borders of both the proximal and distal stumps. The result is four robust suture strands exiting the proximal stump and four exiting the distal stump.
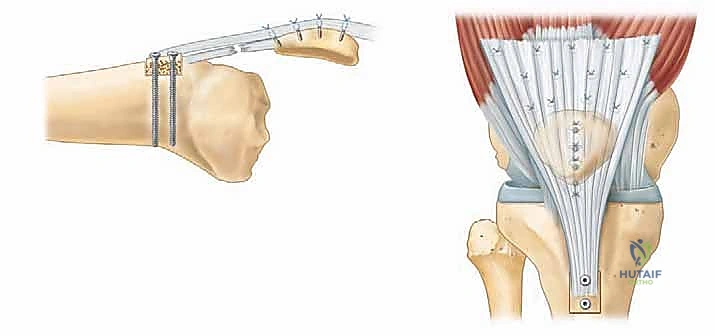
Before tying the core sutures, attention must be directed to the medial and lateral patellar retinacula. These structures are almost universally torn in conjunction with the main tendon. The retinacula should be repaired first using interrupted absorbable sutures (e.g., #1 Vicryl). This crucial step centralizes the patella, reduces tension on the primary tendon repair, and restores the coronal plane stability of the extensor mechanism. Once the retinacula are approximated, the knee is brought into full, 0-degree extension. The proximal and distal core sutures are then tied to each other with the knee fully extended. Tying the sutures in any degree of flexion will result in an overly tight repair, causing severe patella baja and permanent loss of knee flexion.
Acute Proximal Avulsion (Inferior Pole of Patella)
Avulsions from the inferior pole of the patella are the most common presentation of this injury. The surgical strategy here involves reattaching the tendon directly to its bony footprint. After debriding the tendon stump, the inferior pole of the patella is prepared. All soft tissue debris is removed, and the cortical bone is lightly decorticated using a rongeur or a high-speed burr to expose a bleeding, cancellous bone bed, which is vital for osteotendinous integration.
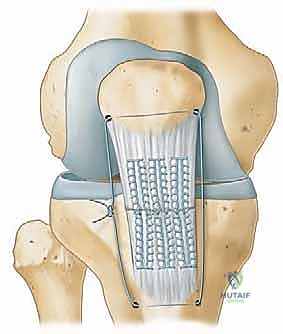
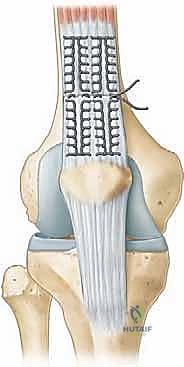
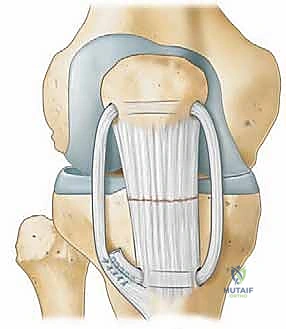
Fixation can be achieved using either transosseous tunnels or suture anchors. For the transosseous technique, three parallel longitudinal tunnels are drilled from the inferior pole of the patella, exiting at the superior pole. The tendon stump is secured using the Krackow technique with heavy non-absorbable sutures. The free ends of these sutures are then passed through the osseous tunnels using a Hewson slider or suture passing wire. The sutures are tied over the superior pole of the patella, often over a cortical bone bridge, while the knee is held in full extension.
Alternatively, modern biocomposite suture anchors provide excellent biomechanical strength and eliminate the need for transosseous drilling. Two or three double-loaded suture anchors (e.g., 4.75mm or 5.5mm) are placed directly into the prepared footprint at the inferior pole. The sutures are then passed through the tendon stump using a Krackow or Mason-Allen configuration. The tendon is firmly reduced to the bony bed, and the sutures are tied securely with the knee in full extension, ensuring intimate contact between the tendon and the bleeding bone.
Acute Distal Avulsion (Tibial Tubercle)
Distal avulsions from the tibial tubercle are less common but require equally robust fixation. The principles remain identical: debridement of the tendon stump, preparation of a bleeding bony bed at the anatomic footprint on the tibial tubercle, and secure reattachment.
For distal avulsions, we strongly prefer the use of suture anchors. Two fully threaded, double-loaded biocomposite anchors (e.g., 5.0 Bio-Corkscrew FT, Arthrex, Inc.) are placed into the tibial tubercle, meticulously recreating the anatomic footprint. The heavy non-absorbable sutures are passed through the distal tendon stump using a locking Krackow technique. The knee is brought into full extension, and the tendon is anatomically reduced to the tubercle. The sutures are tied sequentially, ensuring rigid fixation.
Regardless of the tear location, the final step involves a rigorous intraoperative assessment of the repair. With the sutures securely tied, the knee is slowly and gently flexed. The surgeon visually monitors the repair site for any gap formation or excessive tension. A meticulous repair should allow for at least 90 degrees of passive flexion without compromising the integrity of the construct. Finally, the preserved peritenon is meticulously closed over the repaired tendon using a fine absorbable suture, encapsulating the repair in a biologically active, healing environment.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, patella tendon repair is fraught with potential complications, largely due to the immense biomechanical forces the extensor mechanism must endure during rehabilitation. A thorough understanding of these risks is essential for prompt recognition and appropriate salvage management. The most devastating complication is re-rupture, which occurs in approximately 2% to 5% of cases. Re-rupture typically occurs during the early postoperative phase (within the first 3 months) due to patient non-compliance, an aggressive rehabilitation slip/fall, or failure of the suture material/bone interface. Management of a re-rupture is exceedingly difficult and almost universally requires complex reconstruction with allograft tissue and augmentation, carrying a significantly worse prognosis for return to pre-injury function.
Alterations in patellar height are among the most common, yet frequently underreported, complications. Patella baja (a low-riding patella) occurs when the repair is tensioned too tightly, usually as a result of tying the core sutures while the knee is in flexion rather than full extension. Patella baja leads to significantly increased patellofemoral contact pressures, resulting in early-onset, severe patellofemoral osteoarthritis, anterior knee pain, and a permanent, mechanical block to knee flexion. Conversely, patella alta (a high-riding patella) occurs due to an overly loose repair or gradual stretching of the healing tendon. This results in an extensor lag, profound quadriceps weakness, and a predisposition to patellar instability and subluxation.
Postoperative knee stiffness is nearly universal and requires a delicate balance between protecting the repair and mobilizing the joint. Arthrofibrosis, characterized by dense intra-articular and suprapatellar scarring, can severely limit both flexion and extension. If aggressive physical therapy fails to restore functional range of motion by 3 to 6 months postoperatively, surgical intervention may be required. This typically involves an arthroscopic or open lysis of adhesions, coupled with a gentle manipulation under anesthesia, taking extreme care not to avulse the healed tendon repair.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Re-Rupture | 2% - 5% | Non-compliance, early falls, poor tissue quality, technical failure. | Revision surgery with allograft reconstruction (Achilles bone-block) and augmentation. |
| Patella Baja | 10% - 15% | Tying sutures in flexion, over-tensioning the repair. | Difficult to treat. May require tibial tubercle osteotomy (proximalization) in severe cases. |
| Patella Alta | 5% - 10% | Loose repair, gradual stretching, missed chronic retraction. | Tibial tubercle osteotomy (distalization) or revision reconstruction. |
| Arthrofibrosis (Stiffness) | 15% - 25% | Prolonged immobilization, poor pain control, inadequate physical therapy. | Aggressive PT. Arthroscopic lysis of adhesions and manipulation under anesthesia. |
| Surgical Site Infection | 1% - 3% | Diabetes, obesity, smoking, prolonged operative time. | Immediate superficial/deep I&D, targeted IV antibiotics. Retain hardware if deep, unless loose. |
| IPBSN Neuroma | 5% - 10% | Iatrogenic transection or traction during anterior midline approach. | Desensitization therapy, gabapentinoids. Surgical excision and burying of the nerve stump if refractory. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a patella tendon repair is a complex, multi-phased process that requires constant communication between the orthopedic surgeon, the physical therapist, and the patient. The overarching goal is to protect the fragile surgical repair during the initial phases of biological healing while simultaneously preventing the devastating complications of arthrofibrosis and profound quadriceps atrophy. Modern rehabilitation protocols have largely shifted away from prolonged cast immobilization in favor of early, protected, and highly controlled range of motion.
Phase I: Maximum Protection (Weeks 0 to 2)
Immediately following surgery, the patient is placed in a hinged knee brace locked in full (0 degrees) extension. Weight-bearing status is typically restricted to toe-touch or partial weight-bearing with crutches to minimize eccentric loading on the repair. The primary focus during this phase is wound healing, edema control, and the initiation of isometric quadriceps activation. Patients are instructed to perform frequent quadriceps sets, straight leg raises (only if the brace is locked in extension), and ankle pumps to prevent deep vein thrombosis. Passive range of motion is strictly prohibited unless explicitly cleared by the operating surgeon based on the intraoperative tension assessment.
Phase II: Early Controlled Motion (Weeks 2 to 6)
As the surgical wound heals and early collagen cross-linking begins, the focus shifts to restoring passive range of motion. The hinged knee brace is unlocked to allow a gradual, progressive increase in flexion. A common protocol permits 0 to 30 degrees of passive flexion during weeks 2 to 3, advancing to 60 degrees by week 4, and 90 degrees by week 6. It is imperative that flexion is achieved passively or active-assisted; active knee extension against gravity remains strictly contraindicated, as it places immense stress on the healing tendon. Weight-bearing is gradually advanced to full weight-bearing, but the brace must remain locked in full extension during ambulation to prevent sudden buckling and catastrophic eccentric loading.
Phase III: Strengthening and Neuromuscular Control (Weeks 6 to 12)
By week 6, the tendon has achieved sufficient tensile strength to tolerate the initiation of active range of motion and light resistance training. The brace is typically discontinued for ambulation once the patient demonstrates a normal gait pattern and the ability to perform a straight leg raise without an extensor lag. Physical therapy focuses on closed kinetic chain exercises, such as mini-squats, leg presses (with limited depth), and stationary cycling. Proprioceptive training and balance exercises are also incorporated. Open kinetic chain knee extension exercises (e.g., seated leg extensions) are generally avoided until later in the rehabilitation process due to the high shear forces they place on the patellofemoral joint and the maturing tendon.
Phase IV: Return to Sport and Advanced Function (Months 3 to 6+)
The final phase of rehabilitation focuses on restoring full strength, power, and sport-specific agility. Progression to this phase requires full, pain-free range of motion, resolution of any extensor lag, and quadriceps strength that is at least 80% to 85% of the contralateral, uninjured limb. Activities such as jogging, plyometrics, and cutting drills are gradually introduced under the strict supervision of a physical therapist. Return to full, unrestricted athletic competition is rarely achieved before 6 months postoperatively and often requires up to 9 to 12 months for high-demand, jumping sports.
Summary of Landmark Literature and Clinical Guidelines
The evolution of patella tendon repair techniques is deeply rooted in landmark orthopedic literature. Historically, the management of these injuries was fraught with high rates of failure and stiffness due to inadequate fixation and prolonged immobilization. The foundational work by Insall et al. in the 1980s highlighted the critical importance of restoring precise patellar height, utilizing the Insall-Salvati ratio as a mandatory preoperative and intraoperative metric to avoid the devastating consequences of patella baja.
The biomechanical superiority of modern suturing techniques was firmly established by Krackow et al. Their original description of the locking loop suture technique revolutionized the repair of both Achilles and patella tendons. Biomechanical studies have consistently demonstrated that the Krackow stitch provides significantly higher resistance to gap formation and ultimate load to failure compared to traditional Kessler or Bunnell techniques, largely because the locking loops securely grip the longitudinal collagen bundles, preventing suture pull-through.
More recently, the literature has focused on comparing transosseous tunnel fixation with modern suture anchor technology for proximal and distal avulsions. A landmark biomechanical study by Bushnell et al. (Am J Sports Med) demonstrated that suture anchor constructs provide equivalent, if not superior, ultimate load to failure and significantly less gap formation during cyclic loading compared to traditional transosseous tunnels. Furthermore, suture anchors eliminate the risk of iatrogenic patellar fracture associated with drilling large tunnels and significantly reduce operative time. Consequently, the use of biocomposite suture anchors has become the preferred technique for many contemporary orthopedic surgeons.
Finally, the shift
