

Orthopedic Ob Reconstru Review | Dr Hutaif Hip & Knee R -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
During a primary total knee arthroplasty, the surgeon evaluates the gaps and finds the knee is tight in extension and symmetrical in flexion. Which of the following is the most appropriate next step in management?
Explanation
Question 2
To improve patellar tracking during a total knee arthroplasty without modifying the patellar cut itself, which of the following component position changes is most effective?
Explanation
Question 3
A 72-year-old female presents with recurrent posterior dislocation of her total hip arthroplasty. Intraoperatively, the acetabular cup is found to be well-fixed in 30 degrees of abduction and 0 degrees of anteversion. The femoral stem is well-fixed in 15 degrees of anteversion. Which of the following is the most appropriate management?

Explanation
Question 4
A 78-year-old female sustains a periprosthetic femur fracture around a cemented total hip arthroplasty stem. Radiographs demonstrate a fracture at the tip of the stem. The stem is radiographically loose, but there is excellent bone stock proximally and distally. What is the Vancouver classification and appropriate treatment?

Explanation
Question 5
In modern total hip arthroplasty, highly cross-linked polyethylene is commonly used to reduce wear. What is the primary purpose of remelting the polyethylene after it undergoes gamma irradiation?
Explanation
Question 6
In a posterior-stabilized (PS) total knee arthroplasty design, what is the primary biomechanical function of the cam-and-post mechanism?
Explanation
Question 7
Which of the following is considered an absolute contraindication to medial unicompartmental knee arthroplasty (UKA)?

Explanation
Question 8
A 55-year-old man with a metal-on-metal total hip arthroplasty presents with groin pain and a palpable mass. MRI shows a large cystic mass communicating with the joint. Blood cobalt and chromium levels are significantly elevated. Histopathology of the excised periprosthetic tissue is most likely to show:
Explanation
Question 9
During TKA, the surgeon decides to use an intramedullary guide for distal femoral resection. If the patient has a significant lateral femoral bowing that is not radiographically recognized, what is the most likely error in the coronal plane alignment of the femoral component?
Explanation
Question 10
A patient presents with pain and swelling 5 years after a primary THA utilizing a large metal head on a highly cross-linked polyethylene liner with a titanium stem. Joint aspiration is negative for infection, but serum cobalt levels are markedly elevated while chromium levels are normal or slightly elevated. What is the most likely source of the metal ions?
Explanation
Question 11
In revision total hip arthroplasty, a Paprosky Type IIIB acetabular defect is specifically characterized by which of the following findings?
Explanation
Question 12
A 68-year-old female is undergoing a revision total knee arthroplasty. Intraoperatively, she is found to have a completely deficient medial collateral ligament (MCL) but an intact lateral collateral ligament (LCL) and extensor mechanism. Which of the following constraint levels is required for her revision prosthesis?

Explanation
Question 13
Which of the following statements best describes the mechanical design principle of a 'taper-slip' cemented femoral stem (e.g., Exeter stem)?
Explanation
Question 14
During total hip arthroplasty via a posterior approach, the surgeon utilizes the transverse acetabular ligament (TAL) to guide cup positioning. Aligning the opening of the trial cup parallel to the TAL provides a reliable intraoperative reference for which of the following parameters?
Explanation
Question 15
What is the primary mechanism of polyethylene wear in a well-functioning, well-aligned total knee arthroplasty without third-body debris?
Explanation
Question 16
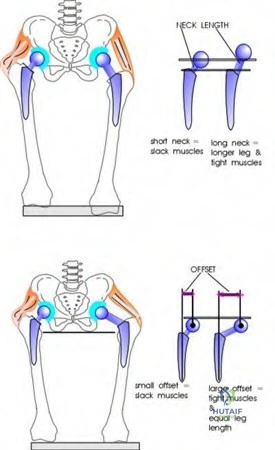
After a total hip arthroplasty, a patient has a noticeable Trendelenburg gait. Radiographic evaluation shows that the femoral offset of the prosthesis is significantly less than the contralateral native hip. How does decreased femoral offset contribute to this gait abnormality?
Explanation
Question 17
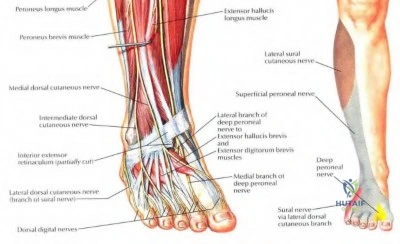
A 60-year-old female undergoes a primary TKA for a severe fixed valgus deformity. On postoperative day 1, she exhibits a foot drop and decreased sensation over the dorsum of her foot. Which of the following was the most likely immediate precipitating cause of her complication?
Explanation
Question 18
A 70-year-old female is evaluated for a primary THA. She has a history of a solid multilevel lumbar spinal fusion from L2 to the sacrum. How should the surgeon adjust the target acetabular cup position to minimize the risk of posterior dislocation?
Explanation
Question 19
Following a high tibial osteotomy for varus gonarthrosis, a patient undergoes a total knee arthroplasty. The surgeon notes significant difficulty everting the patella and exposing the joint due to patella baja. Which step is most appropriate to manage the exposure difficulty without permanently compromising the extensor mechanism?
Explanation
Question 20
During femoral preparation in a TKA, a posterior referencing sizing guide is used. The femur measures between sizes, and the surgeon chooses the larger size. Assuming the posterior cuts remain constant, what is the most likely consequence of this decision?
Explanation
Question 21
A 68-year-old man with advanced ankylosing spondylitis undergoes primary THA. Preoperative radiographs demonstrate a fully fused lumbar spine. Which of the following best describes his spinopelvic biomechanics and the optimal surgical strategy to minimize dislocation risk?
Explanation
Question 22
A 62-year-old man presents with progressive groin pain 7 years after a primary metal-on-polyethylene THA. Radiographs show well-fixed components with normal alignment. A metal artifact reduction sequence (MARS) MRI reveals a solid and cystic mass surrounding the hip joint. Laboratory analysis shows elevated serum cobalt levels with normal chromium levels. What is the primary mechanism of failure?
Explanation
Question 23
A 70-year-old woman complains of a 'giving way' sensation in her knee, particularly when descending stairs, 18 months following a posterior-stabilized TKA. On physical examination, her knee is perfectly stable to varus and valgus stress at 0 degrees and 90 degrees of flexion, but demonstrates significant laxity at 45 degrees of flexion. Which of the following intraoperative technical errors most likely caused this complication?
Explanation
Question 24
An 82-year-old woman with a history of a cemented THA placed 15 years ago sustains a fall. Radiographs demonstrate a displaced periprosthetic fracture around the femoral stem. The fracture extends to the mid-diaphysis. The femoral stem is loose, and there is severe proximal femoral bone loss (less than 2 cm of intact diaphyseal bone proximal to the fracture). According to the Vancouver classification, what is the most appropriate management?
Explanation
Question 25
According to the 2018 International Consensus Meeting (ICM) criteria, which of the following findings alone is considered a definitive major criterion for diagnosing a periprosthetic joint infection?
Explanation
Question 26
A 65-year-old man undergoes a two-stage exchange arthroplasty for a methicillin-resistant Staphylococcus aureus (MRSA) periprosthetic hip infection. An articulating antibiotic-loaded cement spacer is placed during the first stage. Which of the following properties is most essential for the antibiotic selected for inclusion in the polymethylmethacrylate (PMMA) spacer?
Explanation
Question 27
A 72-year-old woman is undergoing revision THA for aseptic loosening. Preoperative radiographs and intraoperative findings reveal severe acetabular bone loss with complete separation of the superior and inferior halves of the hemipelvis. The remaining iliac bone is inadequate for biological fixation of a standard hemispherical cup. What is the most appropriate acetabular reconstruction option?
Explanation
Question 28
In a posterior-stabilized (PS) total knee arthroplasty, the cam and post mechanism is primarily designed to replicate the function of the posterior cruciate ligament (PCL). At what angle of knee flexion does the femoral cam typically engage the tibial post to initiate femoral rollback?
Explanation
Question 29
A 64-year-old man presents with a painful catching sensation in his right knee 14 months after a primary posterior-stabilized TKA. He notes a distinct 'clunk' when actively extending the knee from a flexed position, typically occurring between 30 and 45 degrees of flexion. Non-operative management has failed. What is the most appropriate surgical treatment?
Explanation
Question 30
A 69-year-old woman sustains a chronic, recurrent patellar tendon rupture 2 years following a primary TKA. Previous primary repair with cerclage wire augmentation failed. Her knee is well-aligned and components are radiographically well-fixed. She has an extension lag of 45 degrees. Which of the following reconstruction techniques offers the best long-term outcome for this salvage situation?
Explanation
Question 31
A surgeon is performing a primary THA using the Direct Anterior Approach (Smith-Petersen interval). Which of the following nerves is at the greatest risk of iatrogenic injury during the superficial dissection, and what is the corresponding sensory deficit?
Explanation
Question 32
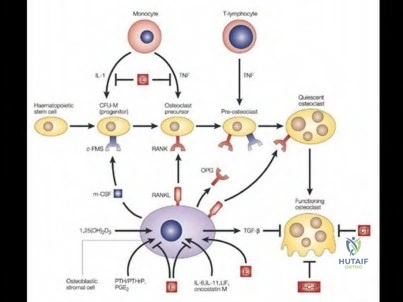
In the pathophysiology of aseptic loosening following total joint arthroplasty, which cell type acts as the primary effector in initiating the foreign-body inflammatory response upon phagocytosis of submicron polyethylene wear debris?
Explanation
Question 33
A 75-year-old patient with Parkinson's disease and a history of recurrent hip dislocations after a primary THA is undergoing revision surgery. The surgeon decides to use a dual mobility articulation. What is the primary biomechanical advantage of this bearing design in preventing dislocation?
Explanation
Question 34
A 55-year-old woman with a ceramic-on-ceramic total hip arthroplasty presents with a loud, audible squeaking noise coming from her hip during walking. She is otherwise asymptomatic. Radiographs show a well-fixed cementless stem and a cementless cup. Which of the following surgical factors is most strongly associated with this phenomenon?
Explanation
Question 35
During a complex revision total knee arthroplasty, the surgeon notes complete absence of the medial collateral ligament (MCL) after removal of the previous implants. The lateral collateral ligament (LCL) and extensor mechanism are intact. Which of the following implant constraints is most appropriate for this patient?
Explanation
Question 36
The introduction of highly cross-linked polyethylene (HXLPE) has significantly reduced wear rates in total hip arthroplasty. Which step in the manufacturing process of HXLPE is specifically designed to eliminate free radicals and prevent subsequent oxidative degradation?
Explanation
Question 37
A 45-year-old woman with a metal-on-metal hip resurfacing presents with unexplained pain and swelling 3 years postoperatively. Infection workup is negative. Histological analysis of the periprosthetic tissue obtained during revision surgery reveals a massive perivascular infiltrate of T-lymphocytes and plasma cells, with minimal macrophages. This histological picture is characteristic of:
Explanation
Question 38
A 70-year-old patient with severe rheumatoid arthritis presents for a primary TKA. Examination reveals a fixed 20-degree valgus deformity. The surgeon plans a lateral parapatellar approach. Which of the following structures is typically the first to be released off the lateral femoral condyle to balance the extension gap in a fixed valgus knee?
Explanation
Question 39
Lewinnek's 'safe zone' for acetabular component positioning in total hip arthroplasty was historically described to minimize the risk of dislocation. What are the specific angular parameters defined by this safe zone?
Explanation
Question 40
In revision total hip arthroplasty for a patient with severe proximal femoral bone loss (Vancouver B3 or Paprosky IIIA), a modular fluted tapered titanium stem is chosen. What is the primary biomechanical mechanism by which this stem achieves initial rotational stability?
Explanation
Question 41
In the treatment of a chronic patellar tendon rupture following Total Knee Arthroplasty (TKA) using a full extensor mechanism allograft, which of the following intraoperative technical steps is most critical to prevent the most common mode of failure (extensor lag)?
Explanation
Question 42
A 65-year-old male with a metal-on-polyethylene THA 8 years ago presents with groin pain. Radiographs show a well-fixed stem and cup. MARS MRI demonstrates a mixed solid and cystic periarticular mass. Hip aspiration reveals low synovial white blood cells but significantly elevated levels of cobalt and chromium. What is the most likely underlying etiology?
Explanation
Question 43
A surgeon is utilizing a gap balancing technique during a primary TKA. After the proximal tibial cut is made and osteophytes are removed, the knee is brought into 90 degrees of flexion. Using a tensor, the flexion gap is noted to be asymmetric, being significantly tighter medially than laterally. What is the most appropriate next step to achieve a rectangular flexion gap before making the femoral cuts?
Explanation
Question 44
A 78-year-old female sustains a periprosthetic femur fracture 10 years after a THA. Radiographs show a spiral fracture around the tip of a cemented polished taper slip stem. The stem has subsided 3 cm. The proximal femur demonstrates severe comminution and osteopenia, rendering it unsupportive. Distal bone stock is excellent. What is the most appropriate classification and treatment plan?
Explanation
Question 45
A patient presents with a painful 'catch' and 'pop' when extending the knee from 45 degrees of flexion following a posterior-stabilized TKA. Which of the following implant design factors most contributes to this specific complication?
Explanation
Question 46
During a primary Total Hip Arthroplasty (THA), restoring the center of rotation is critical. If the surgeon increases the femoral offset without altering the vertical height of the femoral head or leg length, what is the expected biomechanical effect on the abductor mechanism and the joint reaction force?
Explanation
Question 47
A 68-year-old female complains of recurrent knee swelling, a feeling of the knee 'giving way' when walking down stairs, and anterior knee pain 2 years after a primary TKA. Examination reveals recurvatum and anteroposterior laxity at 90 degrees of flexion, but excellent stability in full extension. What intraoperative error most likely led to this presentation?
Explanation
Question 48
To mitigate the risk of oxidative degradation while preserving fatigue strength in highly cross-linked polyethylene used in THA, which of the following manufacturing treatments is most modernly utilized?
Explanation
Question 49
A 55-year-old female reports a history of severe, blistering cutaneous reactions to costume jewelry and watch clasps. She requires a primary TKA for end-stage osteoarthritis. What is the most widely recommended perioperative management regarding her metal hypersensitivity?
Explanation
Question 50
A revision THA is planned for an aseptic loose cup. Preoperative radiographs demonstrate superior migration of the hip center by 3.5 cm, complete destruction of the teardrop, and medial migration of the hip center past Kohler's line. What is the Paprosky classification and most appropriate reconstruction strategy?
Explanation
Question 51
A 62-year-old male is 8 weeks postoperative from a primary TKA. Despite strict adherence to aggressive physical therapy, his range of motion remains 10 to 75 degrees. Radiographs show well-positioned components without evidence of loosening or infection. What is the most appropriate next step in management?
Explanation
Question 52
A 70-year-old male with a history of multi-level instrumented lumbar fusion from L2 to the Pelvis presents for a primary THA. Which of the following describes his expected spinopelvic biomechanics, and how should acetabular component positioning be adjusted?
Explanation
Question 53
During a revision TKA for aseptic loosening, the surgeon notes an absent anterior cruciate ligament, absent posterior cruciate ligament, and an incompetent medial collateral ligament (MCL). The extensor mechanism is intact. Significant metaphyseal bone loss is present. Which of the following implant constraints is absolutely indicated?
Explanation
Question 54
A 58-year-old female presents with persistent anterior groin pain 1 year after a primary THA. The pain is strongly exacerbated by active hip flexion against resistance and when lifting her leg to get into a car. Radiographs show a well-fixed, ingrown acetabular component with 15 degrees of anteversion. The anterior edge of the cup projects 4 mm beyond the native anterior acetabular rim. What is the most appropriate initial diagnostic/therapeutic step?
Explanation
Question 55
A 72-year-old male presents with worsening knee pain 5 years after a primary TKA. The pain occurs exclusively with weight-bearing and is rapidly relieved by rest. ESR and CRP are within normal limits. Serial radiographs show a progressive radiolucent line of 3 mm in all zones around the tibial component. What is the most likely diagnosis?
Explanation
Question 56
Which of the following patient profiles represents the strongest and most widely accepted indication for the use of a dual mobility articulation in a primary total hip arthroplasty?
Explanation
Question 57
In the design and surgical technique of Total Knee Arthroplasty (TKA), what is the primary biomechanical rationale for medializing the patellar component on the native resected patella?
Explanation
Question 58
During a complex revision THA, the surgeon identifies a transverse fracture through the acetabulum separating the superior and inferior hemipelvis. Intraoperatively, the superior and inferior halves move completely independently of one another. Which of the following is the most appropriate definitive management for this chronic pelvic discontinuity associated with severe bone loss in a medically fit patient?
Explanation
Question 59
According to the Evidence-Based Musculoskeletal Infection Society (MSIS) criteria for diagnosing Periprosthetic Joint Infection (PJI), which of the following is considered a major criterion, providing definitive evidence of infection?
Explanation
Question 60
A 65-year-old female with severe rheumatoid arthritis presents with bilateral hip pain. Radiographs reveal bilateral severe protrusio acetabuli (Kohler's line is crossed by the femoral head). During primary THA, which of the following is the most appropriate surgical technique to address the medial acetabular wall defect?

Explanation
Question 61
During a primary total knee arthroplasty, the surgeon assesses the gaps and finds the knee is tight in flexion but symmetric and balanced in extension. Which of the following steps is the most appropriate to balance the knee?
Explanation
Question 62
A 65-year-old active male underwent a total hip arthroplasty with a ceramic-on-ceramic bearing. Three years postoperatively, he complains of an audible squeaking sound from the hip during walking, but denies pain. What is the most significant risk factor for this phenomenon?
Explanation
Question 63
To optimize patellar tracking during a total knee arthroplasty, the femoral component is traditionally externally rotated relative to the posterior condylar axis. What is the primary anatomical landmark used to establish this rotation?
Explanation
Question 64
A surgeon is performing a primary total hip arthroplasty using the direct anterior approach. During the superficial dissection, which of the following nerve injuries is the most common complication?
Explanation
Question 65
A 70-year-old female presents with severe groin pain 6 years after a metal-on-metal total hip arthroplasty. Aspiration yields fluid with low cell count but imaging shows a large cystic mass extending into the pelvis. What is the most likely underlying pathophysiological mechanism?
Explanation
Question 66
A patient requires revision of a total hip arthroplasty due to an extensively loose, cemented femoral stem with deficient metaphyseal bone but an intact diaphysis (Vancouver Type B2). Which of the following is the most appropriate reconstructive option for the femur?
Explanation
Question 67
During a primary total knee arthroplasty utilizing an anterior referencing system, the surgeon decides to upsize the femoral component. What is the most likely biomechanical consequence of this adjustment?
Explanation
Question 68
A 55-year-old female presents with recurrent anterior dislocations of her total hip arthroplasty. Radiographs reveal the acetabular component is placed in 45 degrees of abduction and 40 degrees of anteversion. The femoral stem is in 15 degrees of anteversion. What is the most appropriate surgical management?
Explanation
Question 69
A patient develops a foot drop and numbness over the first web space of the foot immediately following a primary total knee arthroplasty for a severe valgus deformity (25 degrees). What is the most likely etiology of this complication?
Explanation
Question 70
A patient presents with a draining sinus tract on the anterior knee 8 weeks after a primary total knee arthroplasty. According to the Musculoskeletal Infection Society (MSIS) criteria, what is the next best step to confirm the diagnosis of a periprosthetic joint infection?
Explanation
Question 71
During a complex primary total knee arthroplasty, the medial collateral ligament (MCL) is completely avulsed from its femoral origin and cannot be reliably repaired. The joint exhibits gross instability in coronal opening. Which of the following implant designs is strictly indicated?
Explanation
Question 72
When exposing the hip via the posterior approach (Moore), which of the following vascular structures is at greatest risk of injury during the release of the short external rotators and the quadratus femoris?
Explanation
Question 73
During a primary total knee arthroplasty, the flexion gap is assessed and found to be excessively tight, while the extension gap is perfectly balanced. Which of the following is the most appropriate surgical step to balance the knee?
Explanation
Question 74
In total hip arthroplasty, successfully increasing the femoral offset without significantly changing the leg length will have which of the following primary biomechanical effects?
Explanation
Question 75
A 68-year-old male presents with new-onset groin pain 5 years after a primary metal-on-polyethylene total hip arthroplasty. Radiographs show a well-fixed stem and cup. Serum laboratory analysis reveals significantly elevated cobalt levels with normal chromium levels. What is the most likely diagnosis?
Explanation
Question 76
A 75-year-old female sustains a periprosthetic femur fracture 8 years after a total hip arthroplasty.
Radiographs reveal a fracture extending just distal to the tip of the stem. The stem demonstrates subsidence and is clinically loose, but the proximal femoral bone stock remains adequate. According to the Vancouver classification, what is the most appropriate management?
Explanation
Question 77
During a complex revision total knee arthroplasty, the surgeon notes complete incompetence of the medial collateral ligament (MCL). Which level of prosthetic constraint is most appropriate to ensure coronal plane stability?
Explanation
Question 78
When utilizing the direct anterior approach for a primary total hip arthroplasty, the primary superficial internervous plane is developed between which two muscles?
Explanation
Question 79
A patient presents with a painful total knee arthroplasty 2 years postoperatively. Diagnostic synovial fluid aspiration reveals a white blood cell count of 45,000 cells/mcL with 92% polymorphonuclear leukocytes. According to current MSIS criteria, what is the most appropriate definitive management?
Explanation
Question 80
Excessive internal rotation of the femoral component during a primary total knee arthroplasty is most likely to result in which of the following biomechanical complications?
Explanation
None
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-mcqs-online-ob-20-reconstruction-1d