Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues and surgical fellows, to the operating theater and the complex domain of joint-preserving hip surgery. Today, we are embarking on an exhaustive journey into the hip joint, a highly constrained, multiaxial articulation that has become an increasingly recognized source of profound morbidity in both athletic and general populations. With exponential advancements in high-resolution imaging, precision arthroscopic instrumentation, and our evolving biomechanical understanding of chondrolabral pathologies, hip arthroscopy has fundamentally transitioned from a rudimentary diagnostic modality to a highly sophisticated, joint-preserving therapeutic intervention. We will meticulously deconstruct every facet of this discipline, moving from foundational surgical anatomy to advanced intraoperative fixation techniques, and concluding with rigorous postoperative rehabilitation protocols.
The epidemiology of intra-articular hip pathology has undergone a paradigm shift over the last two decades. We now recognize that what was historically deemed "idiopathic osteoarthritis" is frequently the end-stage clinical manifestation of subtle, long-standing morphologic abnormalities, most notably Femoroacetabular Impingement (FAI) syndrome. FAI, characterized by abnormal contact between the proximal femur and the acetabular rim, induces a predictable cascade of labral degeneration, chondral delamination, and progressive joint failure. The prevalence of asymptomatic cam morphology in athletic populations can approach 30-40%, yet it is the dynamic interplay of this morphology with supraphysiologic joint loading that precipitates the symptomatic chondrolabral dysfunction we treat surgically.
Understanding the pathogenesis of these common hip pathologies is an absolute prerequisite for executing effective surgical interventions. Cam impingement typically arises from a loss of normal femoral head-neck offset—an aspherical extension of the femoral head that forcefully enters the acetabulum during flexion and internal rotation. This creates massive shear forces at the chondrolabral junction, leading to "carpet delamination" of the adjacent articular cartilage and subsequent labral tearing. Conversely, pincer impingement stems from global or focal acetabular overcoverage, such as cranial retroversion or coxa profunda. Here, the labrum is crushed between the femoral neck and the prominent acetabular rim, acting as a fulcrum that can paradoxically lever the femoral head posteriorly, causing contrecoup chondral lesions.
Beyond FAI, the spectrum of intra-articular pathology encompasses isolated labral tears (often seen in micro-instability or borderline dysplasia), traumatic chondral shear injuries, loose bodies secondary to synovial chondromatosis or osteochondritis dissecans, and ligamentum teres hypertrophy or avulsion. Synovial proliferative disorders, including pigmented villonodular synovitis (PVNS) and inflammatory arthropathies, also present unique challenges that are exquisitely amenable to arthroscopic synovectomy. Ultimately, our surgical objective in addressing these diverse pathologies is not merely palliative pain relief, but the meticulous restoration of native joint kinematics, the re-establishment of the labral suction seal, and the mitigation of progressive degenerative joint disease.
Detailed Surgical Anatomy and Biomechanics
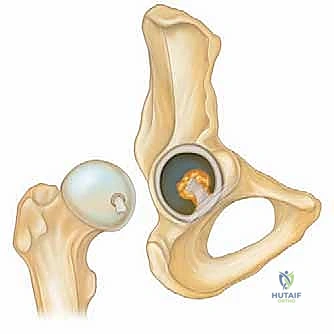
Before we introduce a scalpel or a spinal needle, a profound, three-dimensional spatial awareness of the hip's surrounding anatomy is paramount. The hip is a deeply seated, highly congruent ball-and-socket synovial joint. The osteology dictates the biomechanical envelope: the spherical femoral head is enveloped by articular cartilage, save for the fovea capitis where the ligamentum teres anchors. The acetabulum, a hemispherical socket, features a horseshoe-shaped lunate articular surface. Crucially, the articular cartilage does not extend to the inferiormost region of the acetabulum; this non-articular cotyloid fossa is spanned inferiorly by the transverse acetabular ligament, a critical landmark during arthroscopic navigation and capsular orientation.
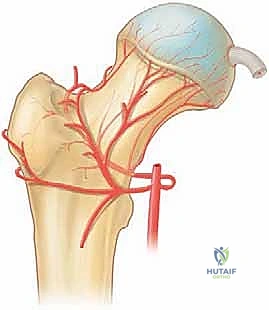
The acetabular labrum is a triangular fibrocartilaginous ring that attaches to the bony rim of the acetabulum, effectively deepening the socket by 21% and increasing the articular surface area by 28%. Biomechanically, the labrum is indispensable; it creates a fluid seal that maintains intra-articular pressurization, thereby protecting the underlying articular cartilage from peak contact stresses. Its microvascular anatomy is critical for surgical decision-making: the labrum receives its blood supply exclusively from the capsular side via the obturator, superior gluteal, and inferior gluteal arteries. The inner articular two-thirds are largely avascular, explaining the inherently poor healing potential of complex, degenerative tears and reinforcing the surgical mandate to preserve and repair rather than resect this vital structure.
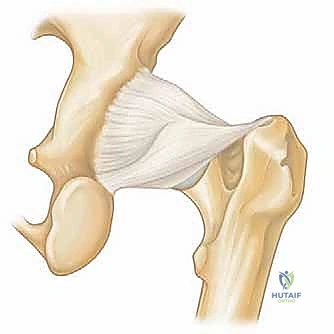
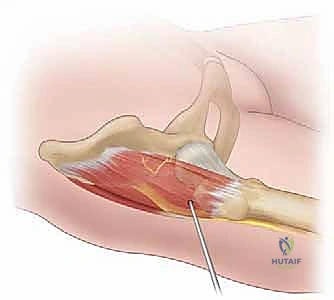
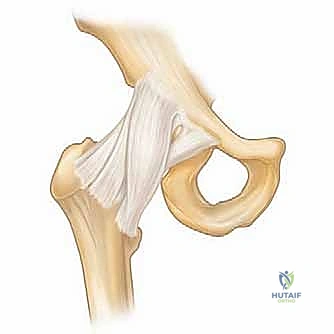
The hip joint is encased by a robust, spiraling capsuloligamentous complex that dictates terminal ranges of motion and provides static stability. The capsule is reinforced anteriorly by the massive iliofemoral ligament (the Y-ligament of Bigelow), widely considered the strongest ligament in the human body, which resists hyperextension and anterior translation. The pubofemoral ligament limits abduction and extension, while the posterior ischiofemoral ligament restricts internal rotation in extension. Iatrogenic violation of these structures during arthroscopic capsulotomy, if left unrepaired, can lead to devastating micro-instability, particularly in patients with underlying ligamentous laxity or borderline dysplasia. Extracapsularly, the ligamentum teres originates from the transverse acetabular ligament and inserts into the fovea, acting as a secondary stabilizer during combined flexion and external rotation.
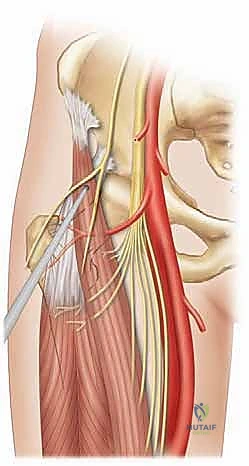
Navigating the neurovascular "no-go" zones demands meticulous precision, as the hip is surrounded by vital structures vulnerable to iatrogenic injury. The Lateral Femoral Cutaneous Nerve (LFCN), derived from L2-L3, is highly variable and superficial, making it exquisitely susceptible to injury during anterolateral portal placement. The femoral neurovascular bundle (nerve, artery, vein, from lateral to medial) lies anteriorly; the femoral nerve is approximately 3.2 cm medial to the standard anterior portal. Posteriorly, the sciatic nerve lies a mere 2.9 cm from the posterolateral portal. Crucially, externally rotating or flexing the hip prior to establishing posterior portals brings the sciatic nerve perilously close to the trochar trajectory. Furthermore, the ascending branch of the lateral circumflex femoral artery traverses the anterior capsule and is at risk during aggressive capsulotomy or anterior rim trimming.
Exhaustive Indications and Contraindications
The indications for hip arthroscopy have expanded dramatically, mirroring advancements in instrumentation and our understanding of hip preservation biomechanics. Historically reserved for the extraction of loose bodies or diagnostic lavage, the modern indications are overwhelmingly therapeutic. The primary indication remains symptomatic Femoroacetabular Impingement (FAI) syndrome—both cam and pincer morphologies—that has failed a rigorous course of conservative management, including targeted physical therapy and intra-articular diagnostic/therapeutic injections. Associated labral tears, whether traumatic or degenerative secondary to FAI, are prime indications for arthroscopic repair or reconstruction.
Beyond FAI, indications have broadened to address extra-articular and peritrochanteric spaces. Arthroscopic management is now considered the gold standard for recalcitrant internal or external snapping hip syndromes (iliopsoas fractional lengthening or iliotibial band release, respectively). Furthermore, endoscopic repair of full-thickness gluteus medius and minimus tendon tears (the so-called "rotator cuff tears of the hip") yields excellent clinical outcomes. Deep gluteal syndrome, encompassing sciatic nerve entrapment by the piriformis or fibrovascular bands, and ischiofemoral impingement are emerging indications where endoscopic decompression provides a minimally invasive alternative to extensive open exposures.
However, strict adherence to contraindications is what separates the master surgeon from the novice. Patient selection is the ultimate determinant of surgical success. Advanced degenerative joint disease is an absolute contraindication; patients with Tönnis Grade 2 or 3 osteoarthritis, or those with less than 2mm of joint space on weight-bearing radiographs, experience unacceptably high failure rates and rapid progression to total hip arthroplasty following arthroscopy. Severe developmental dysplasia of the hip (Lateral Center Edge Angle < 20 degrees) is another absolute contraindication, as arthroscopic intervention (particularly labral debridement or un-repaired capsulotomy) will acutely destabilize the joint, accelerating catastrophic failure. Active intra-articular infection and profound medical comorbidities precluding safe anesthesia also represent absolute barriers to elective arthroscopy.
Relative contraindications require nuanced clinical judgment. Borderline dysplasia (LCEA 20-25 degrees) is a highly debated topic; these patients may undergo arthroscopy for labral repair, but extreme caution must be exercised to avoid over-resection of the acetabular rim, and meticulous, water-tight capsular plication is mandatory to prevent iatrogenic instability. Advanced age (typically > 50 years) is a relative contraindication, not strictly due to chronological age, but due to the high correlation with occult chondral wear. Morbid obesity significantly complicates portal placement, increases the required traction forces (elevating the risk of neuropraxia), and makes fluoroscopic visualization challenging. Finally, profound joint stiffness or adhesive capsulitis may preclude safe joint distraction, necessitating an initial capsular release prior to addressing intra-articular pathology.
Clinical Decision Matrix: Indications and Contraindications
| Category | Specific Pathologies / Conditions | Clinical Considerations |
|---|---|---|
| Primary Indications | Symptomatic FAI (Cam/Pincer), Labral Tears, Loose Bodies, Chondral Flaps | Must have failed conservative management. Requires correlating clinical and radiographic findings. |
| Emerging Indications | Gluteus Medius Tears, Iliopsoas Impingement, Deep Gluteal Syndrome | Endoscopic extra-articular techniques. High success rate in properly selected candidates. |
| Absolute Contraindications | Tönnis Grade 2/3 OA, Joint Space < 2mm, Severe Dysplasia (LCEA < 20°), Active Infection | Arthroscopy will accelerate failure or cause catastrophic instability. Arthroplasty or PAO indicated. |
| Relative Contraindications | Borderline Dysplasia (LCEA 20-25°), Morbid Obesity, Age > 50, Severe Stiffness | Requires advanced surgical skill, capsular plication, and meticulous preoperative counseling regarding failure risk. |
Pre-Operative Planning, Templating, and Patient Positioning
Successful hip arthroscopy is architected long before the patient enters the operating room; it is predicated on an exhaustive clinical evaluation and meticulous radiographic templating. The patient history must dissect the exact quality, location, and mechanical nature of the pain. The classic "C-sign"—where the patient grasps their hip just above the greater trochanter with the thumb posterior and fingers deep into the anterior groin—is pathognomonic for intra-articular pathology. We must differentiate this from lateral trochanteric pain (bursitis/abductor tears) or posterior pain radiating below the knee (lumbar radiculopathy). Mechanical symptoms such as catching, locking, or sharp stabbing pain transitioning from flexion to extension are highly indicative of unstable chondrolabral lesions.

The physical examination is a systematic stress-testing of the joint's biomechanical limits. While resting inspection rarely yields findings, dynamic testing is critical. The FADIR test (Flexion, Adduction, Internal Rotation) is highly sensitive for anterior FAI and labral pathology; a positive test reproduces the patient's sharp groin pain. The FABER test (Flexion, Abduction, External Rotation) helps differentiate intra-articular pain (anterior groin) from sacroiliac pathology (posterior pain). We also rigorously assess for hyperlaxity (Beighton score) and abductor strength (Trendelenburg test). The Dial test and Log Roll test assess for capsular laxity and isolated intra-articular irritability, respectively. Every examination must include a thorough neurovascular assessment of the lower extremity to establish a preoperative baseline.


High-quality imaging is the cornerstone of our surgical blueprint. A standardized radiographic series is non-negotiable: an AP pelvis (to assess global version, LCEA, Tönnis angle, and crossover signs for retroversion), a cross-table lateral or Dunn 45-degree view (to quantify the alpha angle and assess anterior cam morphology), and a false profile view (to evaluate anterior coverage and joint space). Advanced imaging typically involves a high-resolution, non-contrast 3-Tesla MRI or MR Arthrogram. This allows for precise grading of labral tears, assessment of the chondral surfaces (looking for delamination or subchondral edema), and evaluation of the ligamentum teres. Increasingly, 3D CT reconstructions with dynamic impingement simulation software are utilized to map the exact location and volume of cam and pincer lesions, allowing the surgeon to virtually template the osteochondroplasty before making an incision.


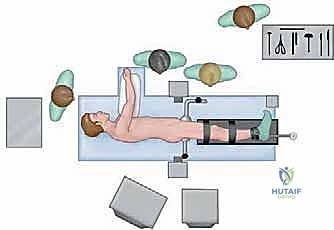
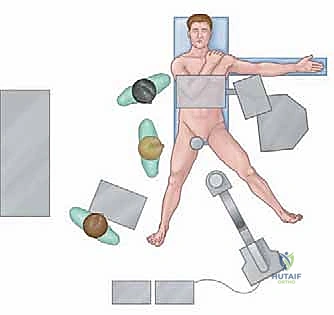
Patient positioning in the operating theater requires obsessive attention to detail to ensure safe joint distraction and mitigate traction-related complications. The procedure can be performed in either the supine or lateral decubitus position, largely dictated by surgeon preference. In the supine position, the patient is placed on a specialized traction table with a well-padded, oversized perineal post positioned eccentric to the operative side, lateralizing the vector of force against the medial thigh rather than the delicate perineal structures. The hip is positioned in slight flexion (10-15 degrees) to relax the anterior capsule, neutral rotation, and roughly 15 degrees of abduction. Traction is applied slowly and meticulously under continuous fluoroscopic guidance until a vacuum seal is broken (often visualized as a "nitrogen bubble" on the monitor) and approximately 10-12 mm of joint space is achieved, allowing safe instrument passage into the central compartment.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with the precise establishment of arthroscopic portals, guided by fluoroscopy and surface anatomy. The Anterolateral (AL) portal is the workhorse viewing portal, established first. It is located 1 cm anterior and 1 cm superior to the tip of the greater trochanter. A spinal needle is advanced under fluoroscopic guidance, aiming for the superior-lateral quadrant of the femoral head, traversing the gluteus medius to enter the capsule. Once the guidewire is passed and the joint insufflated, the Mid-Anterior Portal (MAP) is established under direct arthroscopic visualization. The MAP is located roughly 5-7 cm distal and slightly medial to the AL portal, entering the joint in the safe triangle bounded by the labrum superiorly, the femoral head inferiorly, and the iliofemoral ligament laterally.


Once access is secured, capsular management is the next critical step. An interportal capsulotomy is performed, connecting the AL and MAP portals with a specialized arthroscopic blade parallel to the labrum, roughly 5-8 mm away from the rim. For extensive cam lesions or complex labral reconstructions, a vertical T-capsulotomy extending distally along the femoral neck may be required to optimize visualization and instrument maneuverability. Following capsulotomy, a systematic diagnostic sweep of the central compartment is executed. The ligamentum teres is probed for partial avulsions, the acetabular fossa is cleared of pulvinar overgrowth, and the chondral surfaces are meticulously probed. Cartilage lesions are graded (e.g., Beck or ALAD classifications), and unstable chondral flaps are debrided to stable vertical margins.



Addressing the labrum requires precision. If a pincer lesion is present, the labrum is carefully detached from the chondrolabral junction using an elevator, and a motorized burr is used to perform acetabular rim trimming. This corrects the overcoverage and provides a bleeding bony bed for subsequent labral repair. Labral fixation is achieved using knotless or knotted suture anchors placed strategically along the acetabular rim. The anchors must be angled away from the articular surface to prevent iatrogenic cartilage penetration. Sutures are passed through or around the labrum using specialized curved penetrating devices. The goal is to restore the anatomical footprint and re-establish the critical suction seal against the femoral head, utilizing looped or mattress configurations depending on tear morphology.


Following central compartment work, traction is released, allowing the hip to be flexed and the arthroscope to enter the peripheral compartment to address the cam lesion. The cam deformity is visualized dynamically by rotating the hip. A high-speed burr is utilized to perform a femoral osteochondroplasty, systematically resecting the aspherical bone at the head-neck junction to restore normal offset. Extreme care must be taken to preserve the lateral epiphyseal vessels superiorly and avoid over-resection, which could precipitate a femoral neck fracture. The resection is confirmed both arthroscopically and fluoroscopically, putting the hip through a dynamic range of motion to ensure impingement-free kinematics. Finally, the procedure concludes with a meticulous, water-tight closure of the capsulotomy using heavy, non-absorbable sutures to restore static stability and prevent postoperative micro-instability.