Orthopedic Adult Reconstructive Surgery MCQs & Review | Hip & Knee Arthroplasty Exam Prep

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Adult Reconstructive Surgery MCQs & Review | Hip & Knee Arthroplasty Exam Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
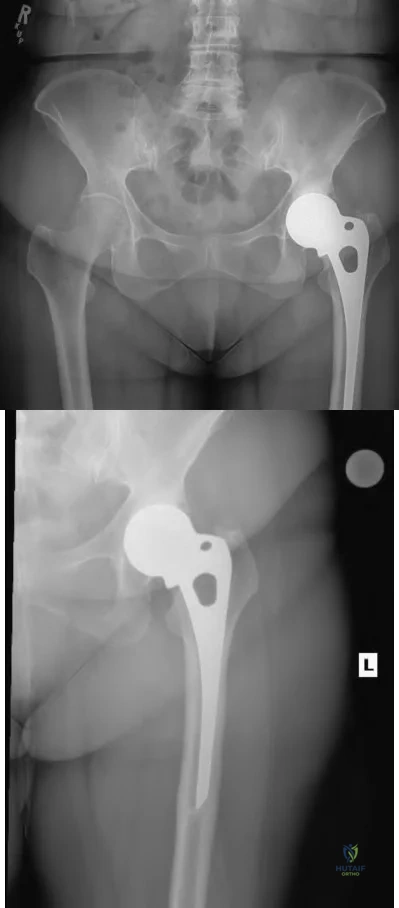
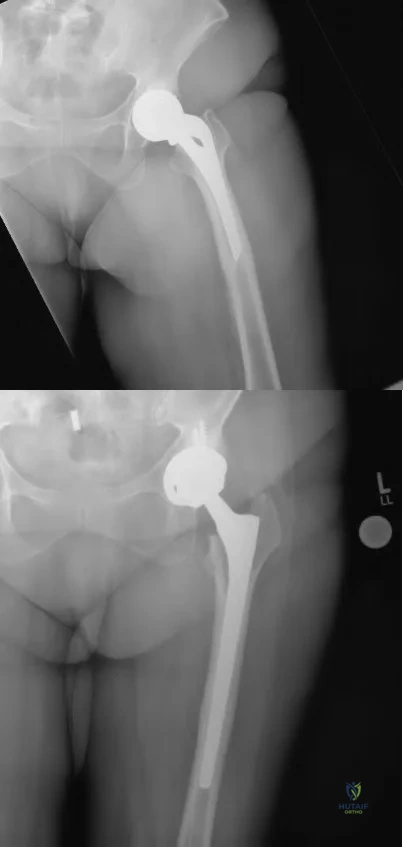
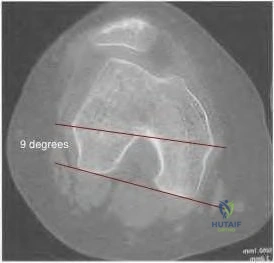
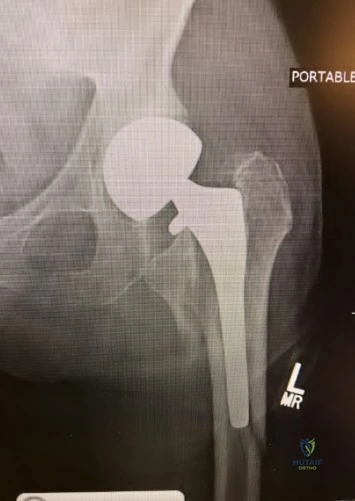
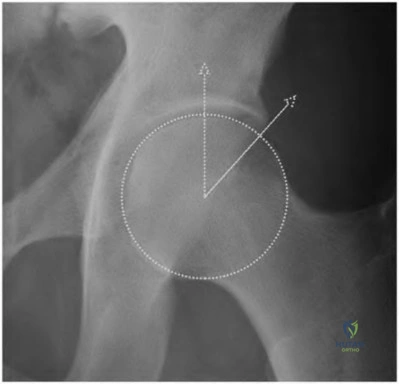
A 72-year-old female presents with progressive left thigh and knee pain for the last year. 5 years ago she sustained a femoral neck fracture treated with a cementless hemiarthroplasty. The thigh pain is worse with weight-bearing. CRP and ESR are within normal limits. Based on her clinical presentation and radiographs, what is the most likely cause of her pain?
Explanation
Question 2
A 68-year-old man undergoes a primary total hip arthroplasty via a posterior approach. Six weeks postoperatively, he sustains a posterior dislocation while bending forward. What is the most common cause of early posterior dislocation following THA?
Explanation
Question 3
Which of the following is considered an absolute contraindication for a unicompartmental knee arthroplasty (UKA)?

Explanation
Question 4
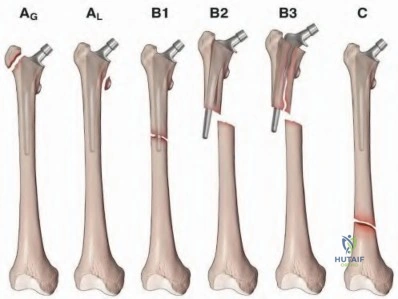
A patient presents with a periprosthetic femur fracture occurring around a loose, polished tapered slip stem, with adequate remaining bone stock. According to the Vancouver classification, what is the most appropriate management?

Explanation
Question 5
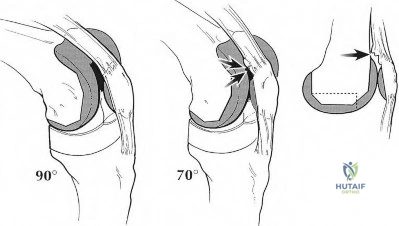
During a total knee arthroplasty (TKA), after making the initial bone cuts, the surgeon notes that the extension gap is tight but the flexion gap is perfectly balanced. What is the most appropriate surgical step to correct this mismatch?
Explanation
Question 6
Conversely, if during TKA the extension gap is perfectly balanced but the flexion gap is excessively tight, which of the following maneuvers is the most appropriate corrective action?

Explanation
Question 7
A patient presents 1 year after posterior-stabilized (PS) total knee arthroplasty complaining of an audible and painful "pop" when extending the knee from a flexed position. What is the most likely diagnosis?

Explanation
Question 8
Which of the following spinopelvic conditions represents the greatest risk for anterior impingement and posterior dislocation following total hip arthroplasty?

Explanation
Question 9
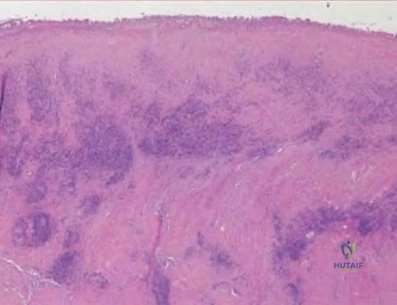
A patient with a large diameter metal-on-metal total hip arthroplasty presents with groin pain and a large cystic mass. Aspiration reveals thick, grayish fluid. Histological analysis of the periprosthetic tissue will most likely demonstrate:
Explanation
Question 10
A patient with a ceramic-on-ceramic total hip arthroplasty complains of a new-onset "squeaking" noise from the hip with every step. Which of the following biomechanical issues is the most highly associated cause of this phenomenon?

Explanation
Question 11
When performing a total hip arthroplasty on a patient with Crowe Type IV developmental dysplasia of the hip (DDH), which of the following surgical strategies is most often required to safely bring the hip center down to the true acetabulum without causing sciatic nerve palsy?
Explanation
Question 12
A patient with severe rheumatoid arthritis is undergoing THA for protrusio acetabuli. During acetabular preparation, the medial wall is found to be extremely thin and functionally incompetent. What is the most appropriate method to manage this defect and restore the hip center?
Explanation
Question 13
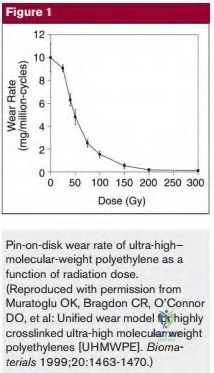
In modern total hip arthroplasty, highly cross-linked polyethylene (HXLPE) is used to drastically reduce volumetric wear. Which process is essential after irradiation to prevent the polyethylene from undergoing in vivo oxidation and subsequent failure?

Explanation
Question 14
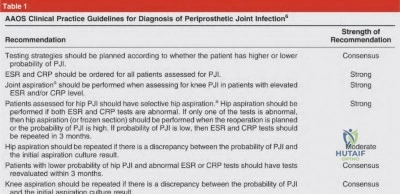
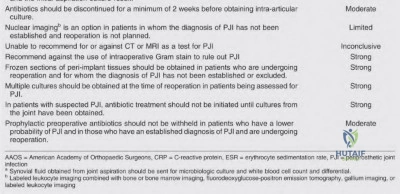
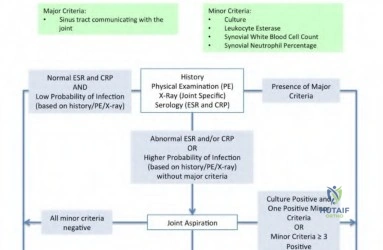
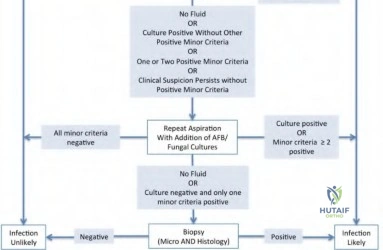
Which diagnostic test provides the highest specificity for ruling in a periprosthetic joint infection (PJI) by measuring a synovial biomarker produced directly by activated neutrophils?

Explanation
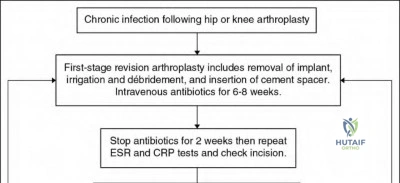
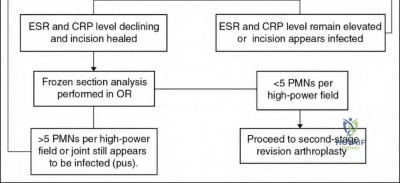
Question 15
The gold standard treatment for a chronic periprosthetic joint infection of the hip is a two-stage revision. Which of the following accurately describes the key components of the first stage?
Explanation
Question 16
A patient presents with massive acetabular bone loss and pelvic discontinuity (complete separation of the superior and inferior halves of the hemipelvis). During revision THA, what is the most mechanically sound construct to achieve rigid fixation?
Explanation
Question 17
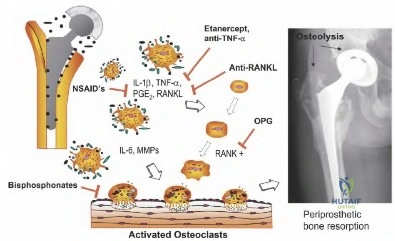
What is the primary biologic mechanism leading to osteolysis and aseptic loosening in total joint arthroplasty?
Explanation
Question 18
When cementing a femoral stem during THA, what is the optimal thickness of the cement mantle to ensure long-term survivorship and limit the risk of cement fracture?
Explanation
Question 19
In a patient with standard risk for deep vein thrombosis undergoing primary elective total knee arthroplasty, what agent is strongly supported by recent guidelines for chemical VTE prophylaxis?
Explanation
Question 20
A constrained condylar knee (CCK) prosthesis utilizes a large, tall tibial post fitting into a deep femoral box. Which of the following is the primary indication to upgrade to a CCK design during revision TKA?

Explanation
Question 21
A 65-year-old female presents with thigh pain. She has been taking oral alendronate for 7 years. Radiographs show a transverse fracture of the lateral cortex of the subtrochanteric femur with focal cortical thickening ("beaking"). What is this injury, and what is the underlying mechanism?
Explanation
Question 22
When performing a Total Hip Arthroplasty (THA) via the direct anterior (Smith-Petersen) approach, the surgeon utilizes a true internervous plane. Which two muscles define this superficial surgical interval?

Explanation
Question 23
A surgeon performing a TKA internally rotates the femoral component excessively in relation to the epicondylar axis. What is the most likely clinical consequence of this technical error?

Explanation
Question 24
When sizing the femoral component in TKA, an anterior referencing system measures from the anterior cortex to establish component size. If the surgeon encounters an "in-between" size and decides to downsize the component using an anterior referencing guide, what happens to the joint gaps?
Explanation
Question 25
A 70-year-old female presents with a severely stiff TKA (ROM 10-60 degrees) two years post-op. Workup for infection is completely negative. She undergoes a revision TKA. Which of the following surgical maneuvers is absolutely critical to successfully expose the joint and avoid catastrophic extensor mechanism avulsion?
Explanation
Question 26
A popliteal artery injury during total knee arthroplasty is a rare but limb-threatening complication. During which specific step of the procedure is this vessel at the greatest anatomic risk of direct transection or injury?
Explanation
Question 27
A 68-year-old female presents with a severe valgus knee deformity (knock-knee) and undergoes TKA. Post-operatively, she exhibits foot drop. Which nerve is most likely injured, and what is the primary mechanism?
Explanation
Question 28
A 40-year-old female with osteoarthritis of the hip desires a hip resurfacing arthroplasty (HRA) to maintain high-impact activities. Which of the following is considered an absolute contraindication to this procedure?
Explanation
Question 29
A patient undergoes a direct lateral (Hardinge) approach for a total hip arthroplasty. Post-operatively, the patient has a severe limp and drops the contralateral pelvis during the stance phase of gait. Which nerve was most likely injured due to excessive superior splitting of the abductor mechanism?
Explanation
Question 30
A dual-mobility (DM) articulation in total hip arthroplasty provides excellent resistance to dislocation. How does the biomechanics of a DM cup achieve this stability compared to a standard bearing?
Explanation
Question 31
A patient presents with an infected TKA and massive extensor mechanism necrosis requiring radical resection. After eradicating the infection, reconstruction of the extensor mechanism is planned. Which of the following is considered the most durable and reliable material for massive full-thickness extensor mechanism defects?
Explanation
Question 32
A 55-year-old male with end-stage hip osteoarthritis also has a stiff, arthrodesed (fused) ipsilateral knee from childhood trauma. Which of the following complications is he at uniquely high risk for after undergoing a standard primary Total Hip Arthroplasty?

Explanation
Question 33
In evaluating a patient with a painful primary THA, you suspect a diagnosis of aseptic loosening due to massive osteolysis. What material property of modern titanium (Ti-6Al-4V) alloy stems helps reduce stress shielding compared to Cobalt-Chromium (CoCr) stems?

Explanation
Question 34
What is the primary function of the "screw-home" mechanism in the normal human knee during terminal extension?

Explanation
Question 35
A 62-year-old male with a history of intravenous drug use and Hepatitis C presents with a completely destroyed, infected knee joint. After failed multiple 2-stage revisions, he undergoes a knee arthrodesis (fusion). What is the optimal position for knee arthrodesis to maximize ambulation efficiency?

Explanation
Question 36
Trabecular metal (highly porous Tantalum) is frequently used in acetabular revision components. What is its main mechanical advantage over traditional sintered titanium bead porous coatings?

Explanation
Question 37
A 65-year-old patient who previously sustained an intra-articular tibial plateau fracture treated with ORIF now presents with severe post-traumatic arthritis requiring TKA. The surgeon must carefully plan the incision. What is a cardinal rule regarding parallel incisions around the knee?
Explanation
Question 38
During a revision TKA for a stiff knee, the surgeon decides to perform a Tibial Tubercle Osteotomy (TTO) to evert the extensor mechanism safely. What is a critical technical requirement when performing a TTO?
Explanation
Question 39
A patient with a history of an arthrodesed (fused) hip from a childhood infection now presents with severe low back pain and ipsilateral knee pain. He requests a takedown of the hip fusion and conversion to a Total Hip Arthroplasty. He must be heavily counseled about the high rate of complications. What is the most likely neuromuscular complication following this specific procedure?
Explanation
Question 40
A 75-year-old male with gouty arthritis of the knee undergoes an aspiration of an acutely swollen joint. What is the classic finding under polarized light microscopy for this condition?
Explanation
Question 41
A 55-year-old female presents with bilateral knee pain. Joint aspiration yields synovial fluid analyzing for positively birefringent, rhomboid-shaped crystals. Radiographs show linear calcifications within the menisci (chondrocalcinosis). What is the diagnosis?
Explanation
Question 42
A 60-year-old diabetic patient with neuropathy presents with a massively swollen, painless knee. Radiographs reveal severe osseous destruction, debris, dislocation, and dense sclerosis. You diagnose Charcot arthropathy. If conservative bracing fails, what is the required component constraint if performing a Total Knee Arthroplasty?

Explanation
Question 43
A patient presents with thigh pain 10 years after receiving a cementless THA. Radiographs show a well-fixed stem but extensive expansile osteolysis in Gruen zones 1 and 7, localized around the metaphysis. The liner is severely worn. What is the most appropriate surgical treatment?

Explanation
Question 44
Which of the following approaches to the hip has historically been associated with the highest risk of postoperative dislocation if careful soft-tissue repair is not performed?

Explanation
Question 45
A 65-year-old male with end-stage hip osteoarthritis is being templated for a THA. It is critical to restore the femoral offset. If the surgeon selects a femoral stem with a high offset option (standard vs high offset neck), what is the primary biomechanical effect on the hip joint?
Explanation
Question 46
A 55-year-old female presents with bilateral osteoarthritis of the hip secondary to developmental dysplasia. She undergoes a THA. The acetabular cup is placed in the "safe zone" defined by Lewinnek. What are the specific angular parameters of the Lewinnek safe zone?
Explanation
Question 47
During routine primary TKA, the surgeon utilizes an anterior referencing system to size the femur. The surgeon selects a size that requires a large amount of anterior bone resection. If the anterior femoral cut notches the anterior cortex of the femur, what catastrophic complication is the patient at high risk for?
Explanation
Question 48
A 30-year-old male with sickle cell disease develops bilateral osteonecrosis (avascular necrosis) of the femoral heads. He has Ficat Stage III disease (subchondral collapse with crescent sign) and severe pain. Core decompression has failed. What is the most appropriate definitive surgical management?

Explanation
Question 49
In patients undergoing TKA, leaving the patella unresurfaced may be chosen by some surgeons. What is the most common complication and reason for reoperation in patients who receive a TKA without patellar resurfacing?
Explanation
Question 50
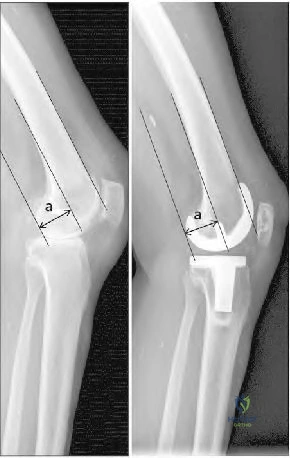
A 60-year-old male with a history of a high tibial osteotomy (HTO) 10 years ago now requires a TKA for end-stage arthritis. A classic anatomic complication of a previous closing-wedge HTO is "patella baja". What surgical difficulty does patella baja present during the TKA?
Explanation
Question 51
Intraoperatively during a primary total knee arthroplasty (TKA), the surgeon notes the joint is excessively tight in flexion but symmetric and well-balanced in extension. Which of the following is the most appropriate next step to achieve a balanced gap?
Explanation
Question 52
A 65-year-old male presents with a painful TKA 2 years postoperatively. Aspiration yields a synovial fluid WBC count of 4,500 cells/µL with 85% polymorphonuclear leukocytes (PMNs). Serum CRP is 15 mg/L. According to MSIS criteria, what is the most appropriate next step in management?
Explanation
Question 53
A 55-year-old active female with a ceramic-on-ceramic total hip arthroplasty (THA) complains of a squeaking noise from her hip when walking or bending. Radiographs show a well-fixed stem and cup. What is the most likely biomechanical cause of this phenomenon?
Explanation
Question 54
A 78-year-old female sustains a fall and presents with thigh pain. Radiographs reveal a periprosthetic fracture around the stem of her THA. The fracture extends just below the tip of the stem. The stem is visibly loose, but the proximal femoral bone stock is adequate. What is the most appropriate treatment?
Explanation
Question 55
A 72-year-old man undergoes revision TKA. Six months later, he presents with an inability to actively extend his knee and a palpable gap at the patellar tendon. Which reconstruction method provides the most reliable long-term clinical outcome for this chronic disruption?
Explanation
Question 56
A 62-year-old male with a metal-on-metal hip resurfacing complains of groin pain and swelling 5 years postoperatively. Joint aspiration is negative for infection. MRI with MARS reveals a large cystic mass communicating with the joint. What histological finding is most expected?
Explanation
Question 57
Following a primary TKA, the surgeon observes lateral patellar tracking during the trial range of motion. Which of the following technical errors most commonly causes this issue?
Explanation
Question 58
A 68-year-old female presents with a painful catching sensation at 30 degrees of flexion when actively extending her knee. She underwent a posterior-stabilized TKA 1 year ago. What is the most appropriate definitive management?
Explanation
Question 59
A surgeon is performing a direct anterior approach for a THA. Postoperatively, the patient notes numbness and a burning sensation over the anterolateral aspect of the operative thigh. Which surgical maneuver most likely caused this complication?
Explanation
Question 60
During a complex revision TKA, the surgeon encounters complete avulsion and absence of the medial collateral ligament (MCL). The lateral collateral ligament is intact. Which level of implant constraint is strictly required?
Explanation
Question 61
A 75-year-old male with a history of recurrent THA dislocations secondary to severe abductor deficiency is planned for revision surgery. His acetabular cup is well-fixed and correctly positioned. Which of the following is the most appropriate reconstructive option?
Explanation
Question 62
When utilizing an anterior referencing system during TKA, downsizing the femoral component will result in which of the following gap changes?
Explanation
Question 63
A 60-year-old male presents with unilateral hip pain 7 years after a metal-on-polyethylene THA utilizing a large-diameter cobalt-chrome head. Inflammatory markers are normal, but serum cobalt levels are significantly elevated while chromium is normal. What is the most likely diagnosis?
Explanation
Question 64
A 55-year-old active male underwent a primary total hip arthroplasty using a ceramic-on-ceramic bearing. Three years postoperatively, he complains of an audible squeaking noise from the hip during ambulation, though he is pain-free. What is the most likely risk factor for this phenomenon?
Explanation
Question 65
During a primary posterior-stabilized total knee arthroplasty, the surgeon uses spacer blocks and notes that the knee is well-balanced in extension but tight in flexion. Which of the following is the most appropriate next step to balance the knee?
Explanation
Question 66
A 60-year-old male presents with isolated medial compartment osteoarthritis of the knee. Which of the following is a classic contraindication to performing a medial unicompartmental knee arthroplasty (UKA) in this patient?
Explanation
Question 67
A 70-year-old female presents with a painful total knee arthroplasty 3 years postoperatively. Synovial fluid analysis reveals an elevated alpha-defensin level. What is the biological function of the molecule being measured?
Explanation
Question 68
A 78-year-old female with a history of a cementless total hip arthroplasty falls and sustains a periprosthetic femoral fracture. Radiographs show a fracture around the tip of the stem with subsidence of the component, but the proximal femoral bone stock remains adequate. According to the Vancouver classification, what is the most appropriate management?
Explanation
Question 69
A 65-year-old male with a metal-on-polyethylene total hip arthroplasty presents with new-onset groin pain 5 years postoperatively. Serum cobalt and chromium levels are significantly elevated, and MRI demonstrates a solid/cystic pseudotumor. What is the most likely source of the metal ions?
Explanation
Question 70
Highly cross-linked polyethylene (HXLPE) was developed to reduce wear rates in total hip arthroplasty. Which of the following material properties is most significantly DECREASED as a result of the irradiation and remelting process used to create HXLPE?
Explanation
Question 71
In total hip arthroplasty, increasing the femoral offset without changing the leg length or neck-shaft angle has which of the following biomechanical effects?
Explanation
Question 72
During a direct anterior approach for a total hip arthroplasty, an intern retracts the tensor fasciae latae laterally and the sartorius medially. A nerve running over the anterior aspect of the thigh is inadvertently injured. This nerve originates from which nerve roots?
Explanation
Question 73
A 68-year-old female is 1 year out from a posterior-stabilized (PS) total knee arthroplasty. She complains of a painful catching and popping sensation in the anterior knee when extending from a flexed position. What is the most likely etiology?
Explanation
Question 74
A patient undergoing revision total hip arthroplasty has massive acetabular bone loss. Intraoperative assessment reveals pelvic discontinuity, and the superior rim of the acetabulum is absent with greater than 3 cm of superomedial component migration. Which Paprosky classification best describes this defect?
Explanation
Question 75
A 72-year-old male presents with inability to perform a straight leg raise 3 months following a primary total knee arthroplasty. Imaging demonstrates an avulsion of the patellar tendon from the tibial tubercle. What is the most reliable surgical management for this complication?
Explanation
Question 76
A patient is undergoing a total knee arthroplasty for a severe valgus deformity. During the surgical exposure and balancing, a structure is injured leading to a postoperative foot drop. At what specific step of the procedure is this nerve at highest risk of injury?
Explanation
Question 77
A 75-year-old patient with Parkinson's disease and abductor deficiency experiences recurrent posterior dislocations following a primary THA. A revision to a constrained acetabular liner is planned. What is the most critical prerequisite for the successful use of a constrained liner?
Explanation
Question 78
A patient with a metal-on-metal total hip arthroplasty presents with a large fluid collection and tissue necrosis around the hip joint. Histological examination of the periprosthetic tissue is most likely to show:
Explanation
Question 79
A patient complains of the operative leg feeling "too long" immediately following a THA. Radiographs show the tip of the greater trochanter is perfectly aligned with the center of the femoral head, but the lesser trochanter is 15 mm distal to the ischial tuberosity compared to the contralateral side. The femoral offset is symmetric. What error occurred intraoperatively?
Explanation
Question 80
In mechanically aligned total knee arthroplasty, the distal femoral cut is typically made at what angle relative to the intramedullary axis of the femur?
Explanation
Question 81
According to the 2018 International Consensus Meeting (ICM) criteria, which of the following is considered a major criterion for the diagnosis of periprosthetic joint infection (PJI)?
Explanation
Question 82
Dual mobility components in total hip arthroplasty reduce the risk of dislocation primarily through which biomechanical mechanism?
Explanation
Question 83
A 65-year-old female presents with persistent knee pain 2 years after a primary TKA. Infection workup is negative. She reports her knee feels unstable when walking down stairs. Examination reveals 15 degrees of recurvatum, 130 degrees of flexion, and a mid-flexion instability. What is the most likely cause of her mid-flexion instability?
Explanation
Question 84
A 55-year-old male is scheduled for a total hip arthroplasty. He has a history of severe developmental dysplasia of the hip (Crowe Type IV). You plan a subtrochanteric shortening osteotomy. Which of the following is the most critical advantage of this technique compared to a greater trochanteric slide osteotomy?
Explanation
Question 85
A 70-year-old woman presents with sudden onset groin pain 6 weeks after an uncomplicated uncemented total hip arthroplasty. Radiographs show a Vancouver B2 periprosthetic femur fracture. Which of the following is the most appropriate management?
Explanation
Question 86
Which of the following bearing surface combinations in total hip arthroplasty is most closely associated with the phenomenon of "stripe wear"?
Explanation
Question 87
A 62-year-old male undergoes a primary total knee arthroplasty. Postoperatively, the patient develops a foot drop and paresthesias over the dorsum of the foot. The surgeon suspects a common peroneal nerve palsy. Which of the following preoperative deformities is most commonly associated with this complication?
Explanation
Question 88
A 58-year-old male presents with groin pain 3 years after a metal-on-metal total hip arthroplasty. Inflammatory markers are normal. A MARS MRI shows a large, thick-walled cystic mass communicating with the joint. What is the most appropriate next step in management?
Explanation
Question 89
In assessing a patient for a potential unicompartmental knee arthroplasty (UKA), which of the following MRI findings is an absolute contraindication for a medial UKA?
Explanation
Question 90
During a revision total knee arthroplasty for aseptic loosening, the surgeon encounters a large uncontained (Type 3) diaphyseal bone defect in the proximal tibia. What is the most appropriate method for managing this specific defect?
Explanation
Question 91
A 70-year-old female with a previous L2-Pelvis fusion presents for a primary THA. Standing and sitting lateral radiographs reveal less than 10 degrees of change in her sacral slope. Due to her stiff spinopelvic complex, she is at the highest risk for which of the following complications, and how should cup position be adjusted?
Explanation
Question 92
A 68-year-old man undergoes primary THA via a direct anterior approach. Postoperatively, he has weakness with active knee extension and diminished sensation over the anterior thigh. Which of the following structures was most likely injured during the surgical approach?
Explanation
None
