Mastering Preoperative Evaluation and Surgical Preparation in Total Knee Arthroplasty
Key Takeaway
A meticulous preoperative evaluation is the cornerstone of a successful Total Knee Arthroplasty (TKA). This phase demands rigorous radiographic templating to determine mechanical axes, comprehensive medical optimization to mitigate perioperative risks, and strategic anesthetic selection. By integrating detailed anatomical assessments with tailored regional or general anesthesia protocols, orthopedic surgeons can minimize complications, optimize biomechanical alignment, and ensure superior postoperative functional outcomes for patients undergoing joint reconstruction.
Comprehensive Introduction and Patho-Epidemiology
Total Knee Arthroplasty (TKA) stands as one of the most transformative and clinically successful surgical interventions in the history of modern medicine. Originally developed as a salvage procedure for severely crippled patients with rheumatoid arthritis, TKA has evolved into a highly reproducible, durable solution for end-stage degenerative joint disease. The primary objectives of the procedure remain steadfast: the eradication of debilitating pain, the restoration of functional ambulation, and the correction of complex coronal, sagittal, and axial plane deformities. As surgical techniques, implant metallurgy, and tribology have advanced, the survivorship of modern TKA constructs routinely exceeds 90% to 95% at two decades of follow-up, solidifying its status as the gold standard for refractory knee arthropathy.
The patho-epidemiology driving the exponential increase in TKA volume is multifactorial, rooted deeply in demographic shifts, the global obesity epidemic, and an aging population that demands a higher quality of life and sustained athletic participation well into their later decades. Osteoarthritis (OA) is the predominant underlying pathology, characterized by the progressive, mechanically and biochemically mediated degradation of articular cartilage, subchondral bone sclerosis, osteophyte formation, and variable degrees of synovial inflammation. Unlike a simple "wear and tear" phenomenon, OA is now understood as a complex disease of the entire joint organ, involving pro-inflammatory cytokines (such as IL-1β and TNF-α), matrix metalloproteinases (MMPs), and altered chondrocyte metabolism that ultimately leads to catastrophic failure of the joint surface.
Beyond primary osteoarthritis, orthopedic surgeons frequently encounter secondary arthritides necessitating arthroplasty. Rheumatoid arthritis (RA) and other seronegative spondyloarthropathies present unique challenges, often characterized by severe symmetric joint space narrowing, profound osteopenia, and complex soft-tissue contractures secondary to chronic synovitis. Post-traumatic arthritis, resulting from prior intra-articular fractures (e.g., tibial plateau or distal femoral fractures), ligamentous instability, or meniscectomy, often presents with retained hardware, distorted anatomical landmarks, and compromised soft-tissue envelopes. These varied etiologies demand a highly individualized approach to preoperative evaluation, as the underlying pathology dictates the choice of surgical approach, the necessity for specialized implant constraints, and the anticipated postoperative rehabilitation trajectory.
The economic burden and epidemiological projections surrounding TKA are staggering. In the United States alone, primary TKA volume is projected to grow exponentially, driven by the expanding indications for younger, more active patients and the rising prevalence of obesity, which exponentially increases the mechanical load across the tibiofemoral articulation. This surge in procedural volume has catalyzed a paradigm shift toward value-based care, outpatient arthroplasty, and rapid-recovery protocols. Consequently, the modern orthopedic surgeon must not only be a master technician but also a meticulous perioperative physician, capable of optimizing complex medical comorbidities to mitigate complications, reduce length of stay, and ensure the long-term survivorship of the arthroplasty construct.
Detailed Surgical Anatomy and Biomechanics
Osteology and Capsuloligamentous Anatomy
A profound mastery of the osseous and capsuloligamentous anatomy of the knee is the non-negotiable foundation of successful TKA. The knee is a complex, modified hinge joint comprising three distinct articulations: the medial tibiofemoral, lateral tibiofemoral, and patellofemoral joints. The distal femur expands into the medial and lateral condyles, separated by the intercondylar notch. The medial condyle is larger, extends further distally, and has a more complex multi-radial geometry, whereas the lateral condyle projects further anteriorly, serving as a critical buttress against lateral patellar subluxation. The proximal tibia features a medial plateau that is concave and a lateral plateau that is convex in the sagittal plane, sloping posteriorly at an average of 7 to 10 degrees. The patella, the largest sesamoid bone in the human body, functions to increase the mechanical advantage of the quadriceps mechanism.
The soft-tissue envelope dictates the kinematic stability of the joint. The medial collateral ligament (MCL) complex consists of the superficial MCL (originating from the medial epicondyle and inserting on the proximal tibial metaphysis) and the deep MCL (meniscofemoral and meniscotibial ligaments). The posteromedial corner is reinforced by the posterior oblique ligament (POL) and the semimembranosus expansions. Laterally, the lateral collateral ligament (LCL) originates from the lateral epicondyle and inserts on the fibular head, functioning in concert with the popliteus tendon and the popliteofibular ligament to form the posterolateral corner (PLC), which resists varus and external rotation forces. The central pivot consists of the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), which govern anterior-posterior translation and dictate the complex rollback mechanism during knee flexion.
Kinematics of the Native Knee
The native knee does not operate as a simple hinge with a fixed axis of rotation; rather, it exhibits complex, six-degrees-of-freedom kinematics. As the knee flexes from full extension, the tibia internally rotates relative to the femur (the "screw-home" mechanism), unlocking the joint. During deep flexion, the femoral condyles exhibit posterior translation (rollback) on the tibial plateau, a motion primarily driven by the tensioning of the PCL and the anatomical geometry of the lateral compartment. The medial compartment acts as a highly constrained pivot point with minimal anterior-posterior translation, while the lateral compartment is highly mobile, allowing the lateral femoral condyle to glide posteriorly. This asymmetric rollback is critical for maximizing knee flexion and preventing posterior impingement of the extensor mechanism.
Biomechanical Principles of Arthroplasty
The primary biomechanical objective of a standard mechanically aligned TKA is to restore the mechanical axis of the lower extremity to a neutral alignment (0 degrees Hip-Knee-Ankle angle), ensuring symmetrical load distribution across the polyethylene bearing surface. The mechanical axis of the femur is defined by a line from the center of the femoral head to the center of the intercondylar notch, while the mechanical axis of the tibia runs from the center of the tibial plateau to the center of the tibial plafond.
Restoring this axis within ±3 degrees of neutral has historically been considered critical to preventing eccentric polyethylene wear, aseptic loosening, and premature catastrophic failure. Furthermore, the surgeon must meticulously recreate the native joint line elevation and balance the flexion and extension gaps. Alteration of the joint line alters the kinematics of the collateral ligaments and the patellofemoral joint. Patellofemoral tracking is governed by the Q-angle, the depth of the prosthetic trochlear groove, and the rotational alignment of the femoral and tibial components. Malrotation of the femoral component (e.g., internal rotation) medializes the trochlear groove, increasing the Q-angle and predisposing the patient to lateral patellar subluxation, accelerated wear, and anterior knee pain.
Exhaustive Indications and Contraindications
The decision to proceed with Total Knee Arthroplasty is predicated on a meticulous synthesis of the patient's subjective symptomatology, objective clinical findings, and radiographic evidence of advanced joint destruction. The primary indication for TKA is severe, end-stage osteoarthritis, rheumatoid arthritis, or post-traumatic arthritis that has proven unequivocally refractory to a comprehensive, prolonged course of conservative management. The patient must exhibit debilitating pain that significantly impairs activities of daily living (ADLs), disrupts sleep architecture, and restricts functional mobility. It is imperative that the surgeon correlates the patient's primary pain generator with the radiographic findings; a patient with severe radiographic OA but minimal clinical symptoms is not a candidate for surgical intervention.
Conservative management must be exhausted prior to surgical consideration. This non-operative armamentarium includes activity modification, aggressive weight loss strategies (critical for reducing joint reactive forces), the optimized use of non-steroidal anti-inflammatory drugs (NSAIDs) or selective COX-2 inhibitors, and targeted physical therapy aimed at strengthening the dynamic stabilizers of the knee (quadriceps, hamstrings, and hip abductors). Intra-articular therapeutic modalities, including corticosteroid injections for acute inflammatory flares and hyaluronic acid (viscosupplementation) for symptomatic relief, should be utilized appropriately. Only when these modalities fail to provide durable relief, and the patient's quality of life is unacceptably compromised, does surgical intervention become indicated.
Contraindications to TKA must be rigorously evaluated to prevent catastrophic perioperative and long-term complications. Absolute contraindications preclude surgical intervention due to an unacceptably high risk of failure, limb loss, or mortality. Active local or systemic infection is the most critical absolute contraindication; placing a massive foreign body into a contaminated field guarantees periprosthetic joint infection (PJI). A compromised extensor mechanism (e.g., chronic, irreparable patellar tendon rupture) renders the joint functionally useless and highly unstable postoperatively. Relative contraindications require careful multidisciplinary optimization and shared decision-making. Severe peripheral vascular disease requires clearance by a vascular surgeon, as the use of a tourniquet or the surgical trauma itself can precipitate acute limb ischemia.
| Category | Specific Conditions | Clinical Rationale and Surgical Implications |
|---|---|---|
| Indications | End-stage Osteoarthritis (Kellgren-Lawrence Grade IV) | Loss of joint space, bone-on-bone articulation causing intractable mechanical pain. |
| Indications | Inflammatory Arthritides (RA, Psoriatic Arthritis) | Progressive joint destruction, severe deformity, and pain despite optimal medical management (DMARDs/Biologics). |
| Indications | Post-Traumatic Arthritis | Articular incongruity leading to rapid cartilage degradation; often requires complex reconstruction. |
| Absolute Contraindications | Active Local or Systemic Infection | Guarantees bacterial colonization of the implant (PJI), necessitating immediate explantation and complex salvage. |
| Absolute Contraindications | Incompetent Extensor Mechanism | Inability to actively extend the knee results in profound instability and functional failure of the arthroplasty. |
| Absolute Contraindications | Neuropathic Joint (Charcot Arthropathy) | Loss of proprioception and protective pain sensation leads to rapid, catastrophic loosening and implant failure. |
| Relative Contraindications | Severe Peripheral Vascular Disease (PVD) | High risk of impaired wound healing, tissue necrosis, and acute limb ischemia postoperatively. |
| Relative Contraindications | Morbid Obesity (BMI > 40-45) | Exponentially increased risk of PJI, aseptic loosening, and complex wound complications. |
| Relative Contraindications | Unoptimized Diabetes Mellitus (HbA1c > 7.5%) | Severe impairment of leukocyte function and microvascular circulation, directly correlating with high PJI rates. |
Pre-Operative Planning, Templating, and Patient Positioning
Radiographic Evaluation
A rigorous, standardized radiographic evaluation is the cornerstone of preoperative planning. The standard TKA series must include a weight-bearing anteroposterior (AP) view, a true lateral view, and a skyline (Merchant or sunrise) view of the patellofemoral joint. The standing AP radiograph is essential for assessing the degree of medial or lateral compartment collapse, the presence of marginal osteophytes, and the overall coronal alignment (varus or valgus deformity). The lateral radiograph provides critical information regarding the posterior tibial slope, the presence of posterior condylar osteophytes (which can limit flexion), and the height of the patella (patella alta or baja). The skyline view allows the surgeon to evaluate patellar tracking, lateral facet sclerosis, and the morphology of the trochlear groove.
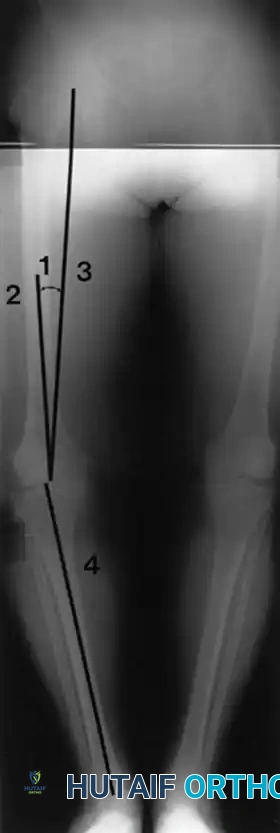
A long-leg standing radiograph (hip-to-ankle) is considered the gold standard for determining the mechanical axis of the lower extremity. This imaging modality allows the surgeon to precisely calculate the angle between the anatomical axis of the femur (the intramedullary canal) and the mechanical axis of the femur (a line from the center of the femoral head to the center of the knee). This specific angle, which typically ranges from 5 to 7 degrees in the normal population, dictates the valgus cut angle that must be set on the distal femoral intramedullary alignment guide. Furthermore, the long-leg film is indispensable for identifying extra-articular deformities, such as diaphyseal bowing, malunited fractures, or retained hardware, which may preclude standard intramedullary referencing and necessitate the use of computer-assisted navigation or robotic-assisted platforms.
Digital Templating and Sizing
Preoperative digital templating is a mandatory exercise that allows the surgeon to anticipate the surgical execution and prepare for potential intraoperative challenges. Templating serves to estimate the approximate sizes of the femoral and tibial components, ensuring that the necessary inventory is available in the operating theater. On the lateral radiograph, femoral sizing is determined by matching the anteroposterior dimension of the implant to the native femur, aiming to restore the posterior condylar offset without overstuffing the patellofemoral joint or notching the anterior femoral cortex. Tibial templating focuses on maximizing cortical coverage without medial or lateral overhang, which can cause painful soft-tissue impingement. Additionally, templating helps identify severe uncontained bone defects (e.g., in severe valgus knees with lateral plateau hypoplasia) that may require the use of metal augments, diaphyseal stems, or metaphyseal cones.
Medical Optimization and Patient Positioning
The preoperative medical optimization of a TKA candidate is an exhaustive, multidisciplinary endeavor. The physiological stress of a major orthopedic procedure, combined with anticipated blood loss, demands adequate cardiopulmonary reserve. Modifiable risk factors must be aggressively managed: smoking cessation is mandated to mitigate wound necrosis and infection risks; glycemic control must be optimized (HbA1c strictly < 7.5%); and nutritional deficiencies (Albumin < 3.5 g/dL) must be corrected.
In the operating theater, precise patient positioning is the first step of the surgical procedure. The patient is placed supine on a radiolucent operating table. A well-padded pneumatic tourniquet is applied to the proximal thigh, though its inflation is subject to surgeon preference, with many modern protocols favoring a "tourniquet-less" approach to minimize ischemic pain and quadriceps inhibition. A lateral post is securely fixed to the bed at the level of the greater trochanter to prevent external rotation of the hip during the procedure. A foot piece or specialized leg holder is utilized, allowing the knee to be smoothly transitioned from full extension to hyperflexion (>120 degrees) and held rigidly during critical bone resections and cementation.
Step-by-Step Surgical Approach and Fixation Technique
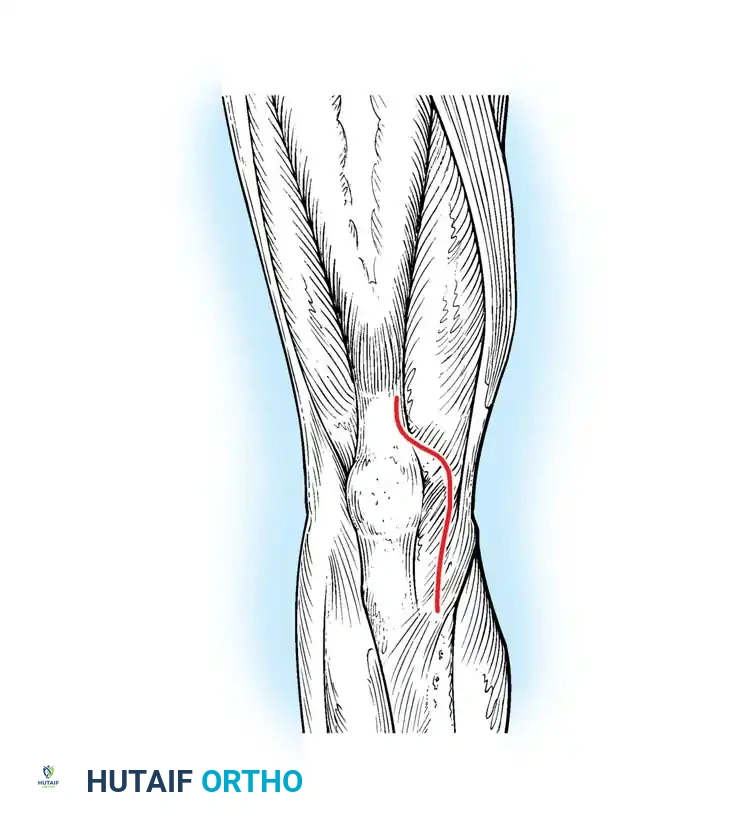
The Medial Parapatellar Arthrotomy
The surgical approach dictates the exposure, and the medial parapatellar arthrotomy remains the undisputed gold standard for primary and revision TKA. It provides unparalleled, extensible access to all three compartments of the knee while preserving the integrity of the extensor mechanism.
The procedure begins with a longitudinal midline skin incision, typically extending from 3-4 cm proximal to the superior pole of the patella down to the medial border of the tibial tubercle. Full-thickness fasciocutaneous flaps are meticulously elevated, preserving the prepatellar bursa and the epifascial vascular plexus to minimize the risk of postoperative skin necrosis. The deep arthrotomy is initiated proximally within the quadriceps tendon, leaving a robust 3-4 mm cuff of tendon attached to the vastus medialis obliquus (VMO) to facilitate a secure, watertight closure. The incision is carried distally around the medial border of the patella and along the medial border of the patellar tendon. The patella is then either everted or laterally subluxated into the lateral gutter, and the retropatellar fat pad is partially excised to visualize the lateral tibial plateau and the anterior horn of the lateral meniscus.
Bone Resection and Soft Tissue Balancing
Following exposure, the surgeon must execute a series of precise bone resections to accommodate the implant while simultaneously balancing the soft tissue envelope. The two primary philosophies are "measured resection" and "gap balancing." In the measured resection technique, bone is removed in a thickness equal to the thickness of the implant, relying on anatomical landmarks to set rotation. The distal femoral cut is typically made first, using an intramedullary guide set to the preoperatively templated valgus angle (usually 5-7 degrees). The proximal tibial cut is made perpendicular to the mechanical axis of the tibia in the coronal plane, with a posterior slope matching the patient's native anatomy or the specific implant's requirements (typically 0-3 degrees for posterior-stabilized designs).
Femoral component rotation is a critical step that directly influences the flexion gap and patellofemoral tracking. Rotation is typically established using a combination of three anatomical axes: the surgical transepicondylar axis (sTEA), Whiteside's line (the anteroposterior axis of the trochlea), and 3 degrees of external rotation relative to the posterior condylar axis. Once the bone cuts are complete, the flexion and extension gaps are assessed using spacer blocks or tensioning devices. If the gaps are asymmetric, sequential soft-tissue releases are performed. For example, a tight medial compartment in a varus knee requires sequential release of the deep MCL, the posteromedial corner, and potentially the superficial MCL to achieve a rectangular, balanced gap.
Implant Fixation Technique
The final phase of the surgical procedure is the secure fixation of the prosthetic components to the host bone. While cementless, highly porous titanium implants are gaining traction in younger, biologically active patients, cemented fixation using polymethylmethacrylate (PMMA) remains the global standard for primary TKA. Meticulous cementation technique is paramount to prevent early aseptic loosening. The sclerotic bone surfaces must be aggressively prepared using pulsatile lavage to remove marrow elements, fat, and debris, allowing for optimal micro-interlock of the cement into the cancellous bone trabeculae.
The bone surfaces are dried meticulously. High-viscosity PMMA is applied to both the implant surface and the host bone. The components are impacted into place, and the joint is brought into full extension to axially load the implants and pressurize the cement mantle. The surgeon must meticulously remove all extruded cement from the medial, lateral, and posterior gutters, as retained cement fragments can cause third-body wear of the polyethylene bearing, severe pain, and mechanical clicking. The tourniquet (if used) is typically deflated prior to closure to achieve meticulous hemostasis, and the arthrotomy is closed in multiple layers using heavy, braided absorbable sutures.
Complications, Incidence Rates, and Salvage Management
Despite the high success rate of TKA, complications can and do occur, often requiring complex, resource-intensive salvage procedures. The orthopedic surgeon must be intimately familiar with the diagnosis, prevention, and management of these devastating events. Complications are broadly categorized into early perioperative events (e.g., neurovascular injury, thromboembolism, acute infection) and late-term failures (e.g., aseptic loosening, polyethylene wear, periprosthetic fracture).
Periprosthetic Joint Infection (PJI) is the most dreaded complication following TKA, representing a catastrophic failure that threatens both the limb and the life of the patient. The diagnosis of PJI is complex and relies on the Musculoskeletal Infection Society (MSIS) or International Consensus Meeting (ICM) criteria, which incorporate serum inflammatory markers (ESR, CRP), synovial fluid analysis (cell count, differential, alpha-defensin), and microbiological cultures. Acute postoperative infections (within 4 weeks) or acute hematogenous infections may be managed with a Debridement, Antibiotics, and Implant Retention (DAIR) procedure, provided the implants remain rigidly fixed. However, chronic PJI necessitates a complex two-stage exchange arthroplasty, involving complete explantation of the components, aggressive osseous debridement, placement of an antibiotic-eluting PMMA spacer, a prolonged course of intravenous antibiotics, and eventual reimplantation once the infection is eradicated.
Instability and extensor mechanism complications represent another major category of failure. Instability can occur in extension (often due to over-resection of the distal femur or inadequate collateral ligament balancing), in flexion (due to an oversized flexion gap or isolated PCL incompetence in a cruciate-retaining knee), or in mid-flexion (often related to joint line elevation). Extensor mechanism disruptions, such as patellar tendon ruptures or severe patellar maltracking resulting in subluxation, are profoundly debilitating. Salvage of a ruptured patellar tendon in the setting of a TKA is notoriously difficult, often requiring reconstruction with synthetic mesh (e.g., Marlex mesh) or massive extensor mechanism allografts, both of which carry high rates of failure and extensor lag.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Periprosthetic Joint Infection (PJI) | 1.0% - 2.5% | Contamination, hematogenous spread, poor host optimization (DM, obesity, smoking). | Acute: DAIR. Chronic: Two-stage exchange arthroplasty with antibiotic spacers. |
| Aseptic Loosening | 2.0% - 3.0% (at 10-15 yrs) | Loss of initial fixation, osteolysis secondary to polyethylene wear debris, malalignment. | Revision TKA with stemmed components, metaphyseal cones, and bone grafting. |
| Venous Thromboembolism (DVT/PE) | 1.0% - 3.0% (Symptomatic) | Virchow's triad (stasis, endothelial injury, hypercoagulability), lack of chemoprophylaxis. | Systemic therapeutic anticoagulation (Heparin bridge to DOAC/Warfarin), IVC filter if contraindicated. |
| Flexion Instability | 1.0% - 2.0% | Excessive posterior condylar resection, failure to balance the flexion gap, PCL rupture in CR knees. | Revision to a higher constraint implant (e.g., Constrained Condylar Knee - CCK) or thicker polyethylene. |
| Extensor Mechanism Disruption | 0.1% - 1.0% | Over-resection of patella, avascular necrosis, aggressive surgical exposure, trauma. | Primary repair with augmentation (Marlex mesh) or complete Extensor Mechanism Allograft. |
| Periprosthetic Fracture | 1.0% - 2.5% | Osteoporosis, anterior femoral notching, trauma, loose components. | ORIF with locking plates (if implant is stable) vs. Revision Arthroplasty with distal femoral replacement. |
Phased Post-Operative Rehabilitation Protocols
The success of a technically flawless surgical procedure can be rapidly unraveled by an inadequate or poorly executed postoperative rehabilitation protocol. Modern TKA rehabilitation is heavily protocol-driven, emphasizing rapid mobilization, multimodal pain management, and the early restoration of functional range of motion. The integration of Enhanced Recovery After Surgery (ERAS) pathways has revolutionized the perioperative experience, significantly reducing length of stay and facilitating the transition to outpatient arthroplasty for appropriately selected candidates.
Immediate Postoperative Phase (Days 0-14)
The immediate postoperative phase focuses on medical stabilization, aggressive pain control, and the initiation of early mobility. Multimodal analgesia is the cornerstone of this phase, designed to minimize opioid consumption and its deleterious side effects (delirium, ileus, respiratory depression). This pathway utilizes scheduled acetaminophen, NSAIDs (e.g., celecoxib or meloxicam), gabapentinoids, and the intraoperative administration of periarticular local anesthetic infiltration (e.g., liposomal bupivacaine mixed with ketorolac and epinephrine).
Mobilization begins on Postoperative Day 0. Patients are assisted out of bed by physical therapy and encouraged to bear full weight as tolerated on the operative extremity using a walker or crutches. Early weight-bearing is critical for mitigating the risk of deep vein thrombosis (DVT), reversing the physiological effects of surgical trauma, and restoring patient confidence. Cryotherapy and strict elevation are employed to manage acute hemarthrosis and soft-tissue edema. Chemical VTE prophylaxis is initiated immediately; current guidelines heavily favor aspirin (81 mg twice daily) for standard-risk patients, reserving potent anticoagulants (LMWH or DOACs) for patients with a documented history of thromboembolic disease or known hypercoagulable states.
Intermediate Rehabilitation (Weeks 2-6)
As the acute inflammatory phase subsides and the surgical incision heals, the focus shifts to aggressive restoration of knee kinematics and the reversal of quadriceps arthrogenic muscle inhibition. The primary goal during this phase is achieving a functional range of motion, specifically full active extension (0 degrees) and at least 110 to 120 degrees of flexion. Failure to achieve full extension rapidly leads to an abnormal, energy-inefficient gait pattern and persistent anterior knee pain.
Physical therapy interventions include patellar mobilization techniques to prevent capsular adhesions, progressive resistance exercises targeting the quadriceps, hamstrings, and gluteal musculature, and closed-kinetic-chain exercises (e.g., mini-squats, leg presses) to enhance proprioception. Neuromuscular electrical stimulation (NMES) is frequently utilized as an adjunct to overcome profound quadriceps inhibition. Patients are typically weaned off assistive devices during this phase, transitioning from a walker to a cane, and eventually to independent ambulation as their dynamic stability improves.
Late Rehabilitation and Return to Sport (Weeks 6-12+)
The final phase of rehabilitation is tailored to the patient's specific functional goals and desired level of activity. While the prosthesis is mechanically stable, the surrounding soft-tissue envelope requires months of remodeling to achieve maximal strength and endurance. Advanced proprioceptive training, agility drills, and sport-specific simulations are introduced.
The orthopedic surgeon must provide clear, evidence-based guidelines regarding return to sport following TKA. Low-impact, continuous-motion activities such as cycling, swimming, golf, and doubles tennis are highly recommended and generally safe. However, high-impact, repetitive-loading sports (e.g., distance running, singles tennis) and heavy contact sports (e.g., football, martial arts) are strongly discouraged, as they generate extreme joint reactive forces that exponentially increase the risk of accelerated polyethylene wear, osteolysis, and early aseptic loosening.
Summary of Landmark Literature and Clinical Guidelines
The practice of Total Knee Arthroplasty is continually refined by a robust, ever-expanding body of peer-reviewed literature and evidence-based clinical practice guidelines. The American Academy of Orthopaedic Surgeons (AAOS) provides comprehensive, rigorously developed guidelines that dictate standard-of-care practices. Notably, the AAOS strongly recommends the universal use of Tranexamic Acid (TXA) in TKA to significantly reduce perioperative blood loss and transfusion requirements, a practice that has fundamentally altered the safety profile of the procedure. Furthermore, AAOS guidelines strongly endorse the implementation of multimodal pain management protocols and support the use of risk-stratified aspirin protocols as non-inferior to aggressive anticoagulation for VTE prophylaxis in standard-risk patients.
The debate surrounding optimal coronal alignment remains one of the most intensely researched topics in modern arthroplasty. Historically, the landmark papers by Insall and Scott established mechanical alignment (restoring the HKA axis to neutral) as the undisputed gold standard. However, recent literature spearheaded by Howell and others has introduced the concept of Kinematic Alignment (KA), which aims to restore the patient's pre-arthritic, native joint line and individual alignment, even if it leaves the limb in slight varus or valgus. While short-to-mid-term randomized controlled trials have demonstrated excellent clinical outcomes and potentially more "natural" feeling knees with KA, long-term survivorship data regarding the risk of eccentric wear in kinematically aligned implants remains a subject of ongoing, rigorous academic scrutiny.
National joint replacement registries, most notably the Swedish Knee Arthroplasty Register and the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR), provide invaluable, population-level data on implant survivorship and failure mechanisms. These registries have consistently demonstrated that highly cross-linked polyethylene significantly reduces wear rates, and that surgeon volume inversely correlates with complication rates. The registry data also highlights the excellent long-term survivorship of both cruciate-retaining and posterior-stabilized designs
