Orthopedic Ob B Reconst Review | Dr Hutaif Hip & Knee R -...
Key Takeaway
Discover the latest medical recommendations for ORTHOPEDIC MCQS ONLINE OB 20 2B RECONSTRUCTION. Inflammatory arthropathy is a significant preoperative factor leading to joint replacement failure, making it a contraindication for unicompartmental knee arthroplasty. This necessitates conversion to a total knee replacement due to disease progression. Careful patient selection is crucial, much like considerations following total hip replacement, to prevent subsequent complications and ensure long-term success.
Orthopedic Ob B Reconst Review | Dr Hutaif Hip & Knee R -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
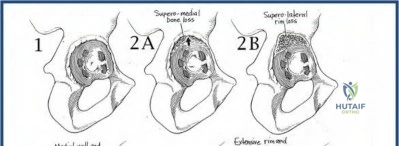
A 72-year-old female is undergoing revision total hip arthroplasty for aseptic loosening. Intraoperative assessment of the acetabulum reveals superior migration of the cup of 3.5 cm, medial migration past the Kohler line, and an ischiolytic lesion. There is severe superior bone loss with less than 40% host bone contact available for the new component, but the anterior and posterior columns remain intact. What is the most appropriate acetabular reconstruction strategy?
Explanation
Question 2
A 65-year-old male is evaluated for a painful total knee arthroplasty (TKA) 2 years postoperatively. Serum CRP is 18 mg/L and ESR is 45 mm/hr. Synovial fluid aspiration demonstrates a WBC count of 4,800 cells/µL with 75% PMNs. An alpha-defensin test is positive. According to the 2018 International Consensus Meeting (ICM) criteria, what is the most appropriate next step in management?
Explanation
Question 3
During a primary TKA, the surgeon uses spacer blocks to assess gap kinematics. The extension gap is symmetric and well-balanced. However, the flexion gap is symmetric but significantly tight, preventing adequate knee flexion with the trial components. Which of the following technical adjustments is the most appropriate next step to balance the knee?
Explanation
Question 4
A 60-year-old male with a metal-on-polyethylene THA presents with an 8-month history of progressive groin pain. Radiographs show a well-fixed stem and cup. MRI reveals a large, thick-walled cystic fluid collection surrounding the hip joint. Aspiration yields yellow fluid, negative cultures, and a WBC count of 500 cells/µL. Serum cobalt is 18 ppb and chromium is 2 ppb. What is the primary pathophysiologic mechanism driving this complication?

Explanation
Question 5
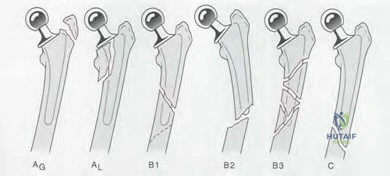
In planning a revision total hip arthroplasty, the surgeon evaluates the femoral bone stock. There is complete loss of metaphyseal cancellous bone, and diaphyseal bone loss extends 2 cm distal to the lesser trochanter. However, the diaphyseal isthmus remains intact with 5 cm of scratch fit available. What is the correct Paprosky Femoral classification and the most appropriate reconstructive strategy?
Explanation
Question 6
A 72-year-old female is scheduled for a primary THA. She has a history of a multi-level lumbar spinal fusion (L2-S1). Preoperative lateral pelvic radiographs demonstrate a sacral slope of 35 degrees standing and 33 degrees sitting. Recognizing this spinopelvic pathology, how should the surgeon adjust the target acetabular cup positioning to minimize the risk of posterior dislocation?
Explanation
Question 7
During a complex primary TKA for a severe fixed valgus deformity, the medial collateral ligament (MCL) is inadvertently transected mid-substance and is deemed completely incompetent and irreparable. Which of the following implant constraints is required to provide adequate stability?
Explanation
Question 8
A surgeon is performing a primary THA using a direct anterior (Smith-Petersen) approach. Which of the following neurologic structures is at highest risk during the superficial dissection, and what is its expected sensory distribution if injured?
Explanation
Question 9
A 78-year-old female presents with a periprosthetic femur fracture around a cemented polished taper slip stem, 10 years post-op. Radiographs show a spiral fracture extending to the distal tip of the stem. The stem cement mantle is debonded and the implant has subsided, but the proximal femoral bone stock remains robust. What is the Vancouver classification and the recommended standard of care?

Explanation
Question 10
What is the primary cellular cascade responsible for aseptic loosening and periprosthetic osteolysis in a total hip arthroplasty?
Explanation
Question 11
A 66-year-old patient undergoes revision TKA. The surgeon utilizes thick tibial and femoral augments to manage bone loss. Postoperatively, the patient reports a painful catch and mid-flexion instability. Lateral radiographs show the inferior pole of the patella is abnormally close to the tibial plateau. What intraoperative technical error most likely led to this complication?
Explanation
Question 12
In a revision THA setting, a patient presents with massive acetabular osteolysis. Preoperative radiographs reveal a distinct transverse fracture line through the acetabular fossa and medial translation of the inferior hemipelvis relative to the superior hemipelvis. What is the diagnosis, and what is the most appropriate intraoperative implant consideration?

Explanation
Question 13
A 75-year-old male with Parkinson's disease and a history of recurrent posterior hip dislocations is scheduled for revision THA. A dual mobility construct is selected. What is the primary biomechanical advantage of a dual mobility bearing that reduces dislocation risk?
Explanation
Question 14
Intravenous Tranexamic Acid (TXA) is routinely utilized in total joint arthroplasty to reduce perioperative blood loss. Which of the following accurately describes its pharmacological mechanism of action?
Explanation
Question 15
A 55-year-old patient underwent the first stage of a two-stage exchange for a chronic MRSA periprosthetic hip infection. An articulating antibiotic spacer was placed. According to established protocols, when is the optimal time to evaluate the patient for the second-stage reimplantation?
Explanation
Question 16
A 68-year-old female presents 3 years post-TKA with the sudden inability to actively extend her knee after a fall. Examination reveals a palpable gap at the superior pole of the patella. For this chronic, full-thickness quadriceps tendon tear in the setting of a TKA, what is the most reliable surgical treatment option to restore extensor mechanism continuity?
Explanation
Question 17
A 45-year-old female is scheduled for a TKA. She reports a history of severe localized blistering and eczematous rash whenever she wears inexpensive jewelry or metal watch bands. Which of the following pre-operative steps and implant choices represents the most appropriate evidence-based management?
Explanation
Question 18
Which of the following intraoperative variables most significantly increases the risk of posterior dislocation following a primary THA performed via a posterior approach?
Explanation
Question 19
A 62-year-old male is evaluated 8 weeks after a primary TKA complaining of severe stiffness. His active range of motion is 15 to 75 degrees. Radiographs demonstrate well-fixed and well-positioned components. Inflammatory markers (CRP/ESR) are strictly within normal limits, and pain is minimal at rest. Supervised physical therapy has reached a plateau over the last 3 weeks. What is the most appropriate next step in management?

Explanation
Question 20
A patient presents 6 months after a right THA complaining that the operative leg feels longer. On physical examination, the distance from the anterior superior iliac spine (ASIS) to the medial malleolus is strictly equal bilaterally. However, the distance from the umbilicus to the medial malleolus is 2 cm greater on the right. Anteroposterior pelvic radiographs demonstrate that the lesser trochanters are perfectly level relative to the ischial tuberosities. What is the most likely etiology of the patient's symptoms?
Explanation
Question 21
A 55-year-old active male is undergoing total hip arthroplasty. The surgeon chooses a highly cross-linked polyethylene (HXLPE) liner. Which of the following is an expected trade-off compared to conventional ultra-high-molecular-weight polyethylene (UHMWPE)?
Explanation
Question 22
In total hip arthroplasty, the 'jump distance' is defined as the distance the femoral head center must travel to dislocate over the rim of the acetabular component. Which of the following modifications most significantly increases the jump distance without altering the component position?
Explanation
Question 23
During a total knee arthroplasty (TKA), the surgeon decides to use a posterior-stabilized (PS) design instead of a cruciate-retaining (CR) design. Which of the following biomechanical phenomena is exclusively facilitated by the cam-and-post mechanism in the PS design?
Explanation
Question 24
Following the initial bone cuts in a cruciate-retaining total knee arthroplasty, the surgeon assesses the gaps with spacer blocks. The knee is tight in flexion and symmetric in extension. Which of the following is the most appropriate next step to balance the knee?
Explanation
Question 25
A 65-year-old female presents with a painful total knee arthroplasty 3 years postoperatively. Her serum CRP is 15 mg/L (normal < 10) and ESR is 40 mm/hr. A joint aspiration is performed. Which of the following synovial fluid profiles is most definitively diagnostic of a chronic periprosthetic joint infection according to the 2018 Evidence-Based International Consensus Meeting criteria?
Explanation
Question 26
A direct anterior approach to the hip is chosen for a primary total hip arthroplasty. The superficial surgical dissection utilizes an internervous plane between muscles supplied by which two nerves?
Explanation
Question 27
A patient presents with aseptic loosening and extensive periprosthetic osteolysis 15 years after a cementless total hip arthroplasty. What is the primary biological mediator responsible for osteoclast activation in this process?
Explanation
Question 28
A surgeon aims to increase femoral offset during a total hip arthroplasty without increasing leg length. Which of the following techniques will best achieve this goal?
Explanation
Question 29
Following trial reduction in a total knee arthroplasty, the patella is found to track laterally and tilts during flexion.
Which of the following component position errors is the most likely cause?
Explanation
Question 30
During a total knee arthroplasty for a severe varus deformity, the medial compartment remains tight in both flexion and extension after initial bone resections. Which of the following is the most appropriate sequence of soft tissue release?
Explanation
Question 31
A 72-year-old female presents with thigh pain following a fall. Radiographs demonstrate a transverse fracture entirely distal to the tip of her well-fixed cementless femoral stem.
According to the Vancouver classification, what is the type and the most appropriate treatment?
Explanation
Question 32
A patient with ankylosing spondylitis is scheduled for a bilateral total hip arthroplasty. To prevent heterotopic ossification (HO), the surgeon plans to administer localized radiation therapy. When is the optimal timing for this prophylaxis?
Explanation
Question 33
A 62-year-old male presents with groin pain and swelling 6 years after a metal-on-polyethylene total hip arthroplasty. Serum cobalt and chromium levels are elevated. Aspiration yields sterile fluid with a high macrophage count. Which of the following implant characteristics is most associated with this condition?
Explanation
Question 34
Which of the following histologic findings is considered the hallmark of an adverse local tissue reaction (ALTR) secondary to metal hypersensitivity (ALVAL) in a patient with a modular total hip arthroplasty?
Explanation
Question 35
A 68-year-old female sustains a complete patellar tendon rupture 4 years after a primary total knee arthroplasty. The components are well-fixed and appropriately positioned. What is the most reliable surgical option to restore active extension?
Explanation
Question 36
A 55-year-old male presents with isolated medial compartment knee osteoarthritis. He is being evaluated for a medial unicompartmental knee arthroplasty (UKA). Which of the following is considered an absolute contraindication to a mobile-bearing UKA?
Explanation
Question 37
In revision total knee arthroplasty, the Anderson Orthopaedic Research Institute (AORI) classification is used to describe bone defects. A femoral defect characterized by metaphyseal bone damage isolated to the medial condyle requiring metal augments, but with an intact joint line and functional collaterals, is classified as:
Explanation
Question 38
A 65-year-old female is undergoing total hip arthroplasty. Preoperative standing and sitting lateral spine radiographs demonstrate that her sacral slope decreases by 5 degrees when moving from standing to sitting. She has no history of spinal fusion. This condition is best described as:
Explanation
Question 39
During a cemented total hip arthroplasty, which of the following techniques is most important to maximize the fatigue strength of the polymethylmethacrylate (PMMA) bone cement?
Explanation
Question 40
According to the American Academy of Orthopaedic Surgeons (AAOS) clinical practice guidelines, which of the following patients undergoing an elective primary total hip arthroplasty is best suited for aspirin alone as a venous thromboembolism (VTE) prophylaxis?
Explanation
Question 41
In a total knee arthroplasty for a patient with a long-standing fixed valgus deformity, the surgeon utilizes a gap-balancing technique. After the initial bone cuts, the lateral side is tight in extension but symmetric and balanced in flexion. Release of which of the following structures is most appropriate as the first step to balance this specific mismatch?
Explanation
Question 42
A 55-year-old male with a metal-on-metal total hip arthroplasty presents with progressive groin pain and a palpable anterior mass. MRI reveals a solid and cystic periprosthetic collection. Histological analysis of the tissue in this condition (ALVAL) is most likely to demonstrate:
Explanation
Question 43
A 45-year-old active male underwent a THA with a ceramic-on-ceramic bearing. Three years postoperatively, he complains of an audible squeaking sound from his hip when walking or bending. Which of the following component positions is most strongly associated with the biomechanical phenomenon causing this sound?
Explanation
Question 44
A 62-year-old male with a primary metal-on-polyethylene THA presents with a 6-month history of worsening hip pain. Blood tests reveal elevated serum cobalt and chromium levels. Radiographs demonstrate a well-fixed modular titanium stem and acetabular cup. What is the most likely source of the metal ion elevation in this specific clinical scenario?
Explanation
Question 45
In revision total knee arthroplasty, management of severe metaphyseal bone defects (AORI Type III) often requires highly porous metaphyseal cones or sleeves. A major biomechanical difference of metaphyseal sleeves compared to traditional unlinked cones is that sleeves:
Explanation
Question 46
A 72-year-old female presents with a chronic patellar tendon rupture 3 years after a primary TKA. Her components are radiographically well-fixed. She has an active extensor lag of 40 degrees. According to recent clinical evidence, which of the following techniques offers the lowest rate of re-rupture and clinical failure for chronic extensor mechanism disruption in TKA?
Explanation
Question 47
Kinematic alignment in total knee arthroplasty aims to restore the patient's pre-arthritic, native joint lines in all three planes. Compared to traditional mechanical alignment, kinematic alignment typically results in which of the following component positions?
Explanation
Question 48
A 75-year-old male requires a revision THA. Preoperative radiographs reveal a loose femoral stem with severe diaphyseal bone loss, a completely absent isthmus, and less than 4 cm of intact diaphyseal bone for distal fixation.
According to the Paprosky classification, this is a Type IIIB defect. Which of the following femoral components is the most appropriate workhorse for this reconstruction?
Explanation
Question 49
Performing a total hip arthroplasty in a patient with active Paget's disease of the pelvis and proximal femur is associated with a significantly increased risk of which of the following specific perioperative complications?
Explanation
Question 50
During a mechanically aligned primary TKA using a measured resection and gap balancing technique, the surgeon evaluates the gaps after the distal femoral and proximal tibial cuts. The extension gap measures 12 mm, while the flexion gap measures 18 mm. What is the most appropriate surgical step to balance the knee?
Explanation
Question 51
A 65-year-old female with long-standing rheumatoid arthritis presents with progressive hip pain. Radiographs demonstrate severe protrusio acetabuli with the femoral head migrated medially past the Kohler line. During THA, which of the following is the most appropriate technique to reconstruct the acetabulum and restore biomechanics?
Explanation
Question 52
A 72-year-old male presents with a loose acetabular component. Imaging demonstrates an inferiorly migrated teardrop, a fracture line extending through the posterior column, and complete separation between the superior and inferior halves of the hemipelvis.
What is the preferred contemporary management for this severe defect?
Explanation
Question 53
A patient is evaluated for a painful TKA one year post-operatively. Serum labs show an elevated CRP (15 mg/L) and ESR (45 mm/hr). Joint aspiration yields 2,500 WBC/uL with 75% PMNs. The synovial fluid alpha-defensin immunoassay is positive. Using the 2018 MSIS (ICM) criteria scoring system, what is the correct diagnosis?
Explanation
Question 54
A 60-year-old female presents with a painful 'catch' and an audible popping sensation when extending her knee from 40 degrees of flexion to full extension, occurring one year after a posterior-stabilized (PS) TKA. What is the fundamental pathomechanics of this specific condition?
Explanation
Question 55
Highly cross-linked polyethylene (HXLPE) has become the standard bearing surface in total hip arthroplasty due to its remarkable wear properties. What is the primary mechanical trade-off associated with the increased cross-linking process compared to conventional UHMWPE?
Explanation
Question 56
An asymptomatic 58-year-old female with a large-head metal-on-metal THA placed 8 years ago presents for a routine follow-up. Her serum cobalt level is 8.5 ppb and chromium is 7.2 ppb. According to consensus regulatory guidelines, what is the most appropriate next step in management?
Explanation
Question 57
A patient presents with a feeling of the knee 'giving way' when descending stairs one year following a primary TKA. Varus/valgus stress testing is stable in full extension and at 90 degrees of flexion, but there is marked laxity at 30-45 degrees of flexion. Which of the following technical errors is the most likely cause of this mid-flexion instability?
Explanation
Question 58
During a direct anterior approach for a total hip arthroplasty, the surgeon develops the internervous plane superficially between the tensor fasciae latae and the sartorius. Which nerve is anatomically at greatest risk of iatrogenic injury during this superficial dissection?
Explanation
Question 59
Tantalum and highly porous titanium constructs are extensively used in revision arthroplasty to manage bone loss due to their excellent biologic fixation properties. What is the approximate porosity of these advanced trabecular metals compared to traditional sintered bead porous coatings?
Explanation
Question 60
Early formulations of zirconia ceramic femoral heads in total hip arthroplasty experienced an unacceptably high rate of catastrophic failure in vivo. This mechanical failure was fundamentally attributed to which of the following material properties?
Explanation
Question 61
A 58-year-old male presents with medial compartment knee osteoarthritis. He is being evaluated for a unicompartmental knee arthroplasty (UKA). Which of the following findings is widely considered an absolute contraindication to proceeding with a UKA?
Explanation
Question 62
In the manufacturing of highly cross-linked polyethylene (HXLPE) for total hip arthroplasty, the polymer is often subjected to a thermal treatment of remelting (heating above its melting point of 135°C). What is the primary advantage of remelting compared to annealing (heating below the melting point)?
Explanation
Question 63
The direct anterior (Smith-Petersen) approach to the hip has gained popularity for total hip arthroplasty. During the superficial dissection, the internervous plane is developed between muscles innervated by which of the following pairs of nerves?
Explanation
Question 64
A 68-year-old female experiences her third posterior dislocation following a primary total hip arthroplasty. CT scan evaluation of her component positioning reveals an acetabular cup anteversion of 10 degrees and a femoral stem retroversion of 5 degrees. According to the combined anteversion theory (Ranawat/McKee), what is her combined anteversion, and what is its clinical implication?
Explanation
Question 65
According to the 2018 International Consensus Meeting on Periprosthetic Joint Infection (PJI), which of the following serves as a major criterion (providing definitive evidence) for the diagnosis of PJI?
Explanation
Question 66
A 74-year-old female sustains a catastrophic rupture of the patellar tendon 4 years after a primary posterior-stabilized total knee arthroplasty. Physical examination reveals a palpable 5 cm gap, and she is unable to actively extend the knee. Which of the following is the most reliable surgical management for this chronic, massive defect?
Explanation
Question 67
During preoperative planning for a revision total hip arthroplasty, you classify the acetabular defect as a Paprosky Type IIIB. Which of the following radiographic findings characterizes this specific defect?
Explanation
Question 68
A 55-year-old male with a metal-on-metal total hip arthroplasty presents with progressive groin pain 6 years postoperatively. Radiographs show well-fixed components with a cup abduction angle of 55 degrees. Laboratory testing reveals a serum cobalt level of 14 ppb (normal < 1 ppb). A Metal Artifact Reduction Sequence (MARS) MRI demonstrates a 6 cm thick-walled cystic mass communicating with the joint. What is the most appropriate definitive management?
Explanation
Question 69
To optimize patellofemoral tracking and minimize the risk of patellar subluxation during a total knee arthroplasty, the patellar component should ideally be placed in which position on the resected patellar surface?
Explanation
Question 70
In total hip arthroplasty, hard-on-hard bearing surfaces (such as ceramic-on-ceramic) demonstrate exceptionally low wear rates. This is primarily attributed to which of the following lubrication regimes occurring during normal walking?
Explanation
Question 71
In a posterior-stabilized (PS) total knee arthroplasty design, what is the primary biomechanical function of the femoral cam and tibial post mechanism during knee flexion?
Explanation
Question 72
A 45-year-old male is undergoing revision total hip arthroplasty for aseptic loosening. He has a history of severe Brooker class III heterotopic ossification following his index procedure. What is the most effective prophylactic regimen to prevent recurrence of heterotopic ossification in this high-risk patient?
Explanation
Question 73
The Exeter femoral stem is a classic example of a collarless, polished, double-tapered cemented implant. By which biomechanical principle does this specific stem design achieve long-term stability?
Explanation
Question 74
Polymethylmethacrylate (PMMA) bone cement is frequently used for component fixation in arthroplasty. What is the primary mechanism by which PMMA secures a prosthesis to the host bone?
Explanation
Question 75
A 70-year-old female requires a revision total knee arthroplasty. Preoperative radiographs and intraoperative assessment reveal substantial metaphyseal bone loss involving both the medial and lateral femoral condyles, while the collateral ligament attachments and joint line remain reasonably identifiable. An intraoperative scenario resembling
is encountered. According to the Anderson Orthopaedic Research Institute (AORI) classification, what is her femoral bone defect type?
Explanation
Question 76
An anterior dislocation of a total hip arthroplasty is most likely to occur when the operative limb is placed in which combination of positions?
Explanation
Question 77
In the setting of revision total knee arthroplasty, a Constrained Condylar Knee (CCK) prosthesis is best indicated for a patient with which of the following clinical scenarios?
Explanation
Question 78
A 62-year-old female presents with a painful 'catching' and an audible pop in her knee when extending from a flexed position, one year after a primary total knee arthroplasty. This complication, known as patellar clunk syndrome, is primarily associated with which of the following arthroplasty designs?
Explanation
Question 79
During trial reduction of a primary total hip arthroplasty, the surgeon determines that the hip is stable but the patient's operative leg is 5 mm short and the offset is 5 mm less than the contralateral side. The current trial uses a standard (+0) neck length. If the surgeon changes the modular femoral head to a +5 mm neck length (assuming a standard 135-degree neck angle), what will be the effect on leg length and offset?
Explanation
Question 80
A 52-year-old active male who underwent an uncomplicated primary total hip arthroplasty 4 years ago presents with an audible squeaking noise emanating from his hip during deep flexion and normal gait. He denies any pain, and radiographs show well-fixed components in acceptable alignment. Which of the following bearing surface combinations is most commonly associated with this phenomenon?
Explanation
Question 81
A 68-year-old male presents with aseptic loosening of a THA. Radiographs show a Paprosky Type IIIB femoral defect. The femoral isthmus has approximately 1.5 cm of diaphyseal scratch fit available. What is the most appropriate femoral revision strategy?
Explanation
None
