Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4)
Key Takeaway
Learn more about Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4) and how to manage it. Top-rated Orthopedic Sports Medicine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Closure of the rotator cuff interval results in elimination of which direction of shoulder instability?
Explanation
Question 2
In overhead athletic activities, the kinetic chain generates what percentage of force from the leg and trunk segments of the chain?
Explanation
Question 3
A 40-year-old right-handed professional football player reports persistent right wrist pain after falling during a game 5 days ago. A radiograph is shown in Figure 21. Management should consist of
Explanation
Question 4
A 29-year-old ultramarathoner, who is halfway into a 50-mile race, is sweating profusely. He suddenly collapses, is unresponsive, and has violent muscle contractions. Prior to these symptoms, he had been drinking water at every water stop (every 1 mile). What is the most likely diagnosis?
Explanation
Question 5
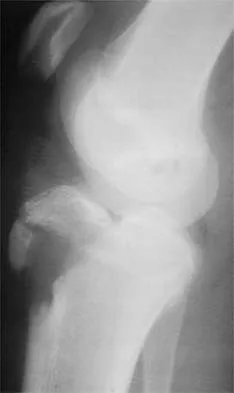
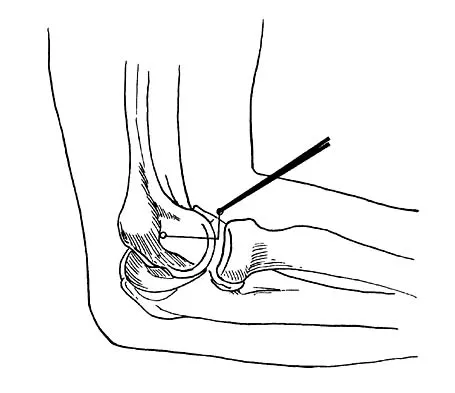
A 12-year-old Little League pitcher reports lateral elbow pain and "catching." Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of
Explanation
Question 6
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a
Explanation
Question 7
Tension force in the anterior cruciate ligament during passive range of motion is highest at
Explanation
Question 8
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
Question 9
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure?
Explanation
Question 10
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Question 11
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted?
Explanation
Question 12
The use of knee arthroscopy following total knee arthroplasty is most effective in treating which of the following conditions?
Explanation
Question 13
Significant anterior tibial translation occurs during which of the following rehabilitation exercises?
Explanation
Question 14
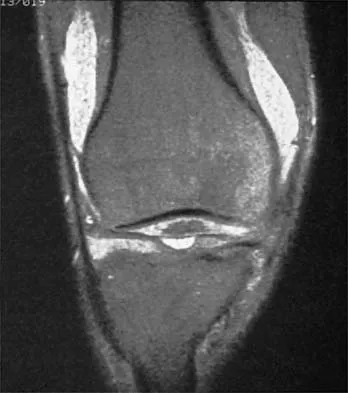
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?
Explanation
Question 15
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
Question 16
A 43-year-old soccer player who had knee pain following a twisting injury underwent an arthroscopic meniscectomy 6 months ago. He continues to report posterior knee pain. Examination reveals soft-tissue fullness and tenderness just above the popliteal fossa, trace knee effusion, full range of knee motion, no instability, and negative meniscal signs. Radiographs show some mild medial joint space narrowing but no other bony changes. What is the next most appropriate step in management?
Explanation
Question 17
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of
Explanation
Question 18
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Explanation
Question 19
Storage of musculoskeletal allografts by cryopreservation is achieved by
Explanation
Question 20
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
Explanation
Question 21
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
Question 22
What procedure can eliminate a sulcus sign?
Explanation
Question 23
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
Question 24
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete?
Explanation
Question 25
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
Question 26
Comparing bone-patellar tendon-bone (BPTB) autograft to hamstring autograft for anterior cruciate ligament (ACL) reconstruction, what is a well-established difference in long-term outcomes based on current evidence?
Explanation
Question 27
In a throwing athlete with a type II superior labrum anterior and posterior (SLAP) lesion, the 'peel-back' mechanism exerts maximal torsional force on the biceps anchor. This mechanism is primarily observed during which specific phase of throwing?
Explanation
Question 28
During medial patellofemoral ligament (MPFL) reconstruction, accurate femoral tunnel positioning is crucial to avoid non-physiologic graft tension and altered patellofemoral kinematics. According to Schöttle's method, what is the correct radiographic location of the MPFL femoral insertion on a strict lateral radiograph?
Explanation
Question 29
A 22-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability with 25% glenoid bone loss. Postoperatively, he presents with profound weakness with shoulder abduction and absent sensation over the lateral aspect of the shoulder. Which nerve was most likely injured, and what is its pertinent anatomic relationship during the procedure?
Explanation
Question 30
A 25-year-old male hockey player presents with chronic groin pain exacerbated by flexion and internal rotation. Imaging reveals a significant Cam-type morphology. In femoroacetabular impingement (FAI), where does the primary cartilage damage classically initiate in the setting of an isolated Cam lesion?
Explanation
Question 31
Following a posterolateral corner (PLC) and ACL injury, a patient is undergoing surgical reconstruction. When drilling the fibular collateral ligament (FCL) femoral tunnel, understanding the anatomy is essential. What is the anatomic relationship of the FCL femoral footprint to the popliteus sulcus/attachment?
Explanation
Question 32
A 30-year-old cyclist sustains a direct blow to his superior shoulder during a fall. Radiographs demonstrate a type III acromioclavicular (AC) joint separation. While deciding between surgical and non-operative management, which of the following is considered an absolute indication for acute surgical intervention?
Explanation
Question 33
During the late cocking and early acceleration phases of throwing, which specific component of the ulnar collateral ligament (UCL) complex of the elbow serves as the primary restraint to valgus stress?
Explanation
Question 34
A 45-year-old woman experiences a painful pop in the posterior aspect of her knee while descending stairs. MRI demonstrates a complete radial tear of the posterior root of the medial meniscus with 3 mm of meniscal extrusion. If this injury is left untreated, the knee joint contact mechanics will most closely resemble which of the following conditions?
Explanation
Question 35
When evaluating the non-operative management of acute Achilles tendon ruptures utilizing an early functional rehabilitation protocol compared to surgical repair, current high-level evidence demonstrates:
Explanation
Question 36
A 25-year-old athlete undergoes an isolated posterior cruciate ligament (PCL) reconstruction. The surgeon debates between a transtibial and a tibial inlay technique. Which of the following is the primary biomechanical advantage of the tibial inlay technique compared to the transtibial technique?
Explanation
Question 37
A 45-year-old overhead worker presents with shoulder pain. MRI reveals a type II SLAP tear. After failed conservative management, surgical intervention is planned. Compared to SLAP repair, primary biceps tenodesis in this age group is associated with:
Explanation
Question 38
A 21-year-old collegiate baseball pitcher undergoes ulnar collateral ligament (UCL) reconstruction using the docking technique. He is concerned about potential postoperative complications. Which of the following is the most common complication following this procedure?
Explanation
Question 39
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, identifying the correct femoral footprint is critical for proper graft isometry. Radiographically, Schöttle's point representing the femoral origin of the MPFL is located:
Explanation
Question 40
A 19-year-old female soccer player sustains a twisting injury to her knee. Radiographs reveal an avulsion fracture of the lateral tibial plateau.
Which of the following intra-articular structures is most likely to be injured concurrently?
Explanation
Question 41
A 22-year-old rugby player presents with recurrent anterior shoulder instability. A 3D CT scan is obtained to evaluate anterior glenoid bone loss.
The 'glenoid track' concept is utilized to determine the risk of an engaging Hill-Sachs lesion. The glenoid track width is calculated as:

Explanation
Question 42
A 50-year-old female experiences a sudden pop in her posterior knee while squatting. MRI demonstrates a radial tear at the posterior root of the medial meniscus.
Biomechanically, leaving this medial meniscus posterior root tear untreated is most comparable to which of the following?

Explanation
Question 43
A 28-year-old male undergoes hip arthroscopy for femoroacetabular impingement (FAI) with a symptomatic CAM lesion. During the osteochondroplasty of the anterolateral femoral head-neck junction, the surgeon must be cautious to avoid injury to the primary blood supply of the femoral head. Which vessel is at greatest risk if the resection is carried too far posterosuperiorly?
Explanation
Question 44
A 30-year-old cyclist falls directly onto his shoulder. Clinical examination reveals significant superior displacement of the clavicle with a prominent step-off. Radiographs show superior displacement of the clavicle by 150% compared to the contralateral side.
According to the Rockwood classification, what specific anatomical disruption distinguishes this injury from a Type III AC joint separation?

Explanation
Question 45
A 35-year-old recreational basketball player sustains an acute Achilles tendon rupture. He elects to undergo a minimally invasive percutaneous repair to minimize wound complications. During the procedure, the surgeon places sutures through the proximal stump of the tendon. Which of the following structures is at the highest risk of iatrogenic injury during this specific step?
Explanation
Question 46
A 25-year-old professional rugby player sustains a contact injury to his right knee. Physical examination reveals a positive dial test with 20 degrees of increased external rotation compared to the contralateral side at both 30 degrees and 90 degrees of knee flexion. Varus stress testing demonstrates grade III laxity at both 0 degrees and 30 degrees of flexion. Which combination of ligamentous structures is most likely injured?
Explanation
Question 47
A 22-year-old collegiate baseball pitcher complains of posterior shoulder pain that is most severe during the late cocking phase of throwing. He has a loss of 25 degrees of internal rotation compared to his non-throwing shoulder. Which of the following describes the primary pathophysiologic mechanism for his pain?
Explanation
Question 48
A 28-year-old male undergoes right hip arthroscopy for femoroacetabular impingement. Postoperatively in the recovery room, he complains of profound numbness in the perineum and scrotum, and difficulty achieving an erection over the next several days. Which mechanism is the primary cause of this complication?
Explanation
Question 49
A 16-year-old female experiences a first-time lateral patellar dislocation while playing soccer. The patella spontaneously reduces. Initial radiographs reveal no acute fractures. Which of the following is an absolute indication for surgical intervention following this primary dislocation event?
Explanation
Question 50
When comparing the outcomes of acute Achilles tendon ruptures treated with operative repair versus non-operative management utilizing early functional bracing and mobilization, non-operative management is associated with which of the following?
Explanation
Question 51
A 20-year-old collegiate pitcher undergoes ulnar collateral ligament (UCL) reconstruction utilizing a palmaris longus autograft. Which of the following technical factors is most critical for successfully restoring the normal kinematics and stability of the elbow?
Explanation
Question 52
A 45-year-old man falls onto his outstretched arm while skiing and sustains an acute, traumatic isolated full-thickness tear of the subscapularis tendon. Which of the following physical examination findings is most specific for this injury?
Explanation
Question 53
A 24-year-old athlete presents with a failed anterior cruciate ligament (ACL) reconstruction.
Computed tomography evaluation demonstrates significant femoral and tibial tunnel widening, with both tunnels measuring >16 mm in diameter. What is the most appropriate next step in management?

Explanation
Question 54
During the biomechanical evaluation of the acromioclavicular (AC) joint complex, which specific ligamentous structure provides the primary restraint against superior displacement of the distal clavicle?
Explanation
Question 55
A 13-year-old skeletally immature male gymnast complains of ongoing knee pain.
MRI reveals a 1.5 cm x 1.5 cm osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. The overlying cartilage is intact, and there is no fluid behind the lesion. Non-operative management, including restricted weight-bearing and activity modification, has failed after 6 months. What is the most appropriate surgical treatment?
Explanation
Question 56
A 24-year-old female athlete undergoes an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Postoperatively, she demonstrates a severe loss of terminal knee flexion. During physical examination under anesthesia, the reconstructed graft is noted to be excessively tight in flexion, but relatively lax in extension. What is the most likely technical error that occurred during the reconstruction?
Explanation
Question 57
A 28-year-old soccer player sustains a direct blow to the anteromedial aspect of the proximal tibia while the knee is flexed. On physical examination, the dial test reveals 25 degrees of external rotation of the tibia compared to 10 degrees on the contralateral side at 30 degrees of knee flexion. However, at 90 degrees of knee flexion, the external rotation is symmetric bilaterally. Which of the following structures is most likely injured?
Explanation
Question 58
A 22-year-old collegiate baseball pitcher complains of vague anterior shoulder pain and a 'dead arm' sensation that exclusively occurs during the late cocking phase of throwing. An MRI arthrogram confirms an isolated Type II SLAP (Superior Labrum Anterior and Posterior) tear. What is the primary biomechanical mechanism responsible for generating this specific pathology in an overhead athlete?
Explanation
Question 59
A 50-year-old active female feels a sharp 'pop' in her posterior knee while rising from a deep squat. MRI reveals a complete radial tear immediately adjacent to the posterior horn medial meniscus attachment, with 4 mm of meniscal extrusion seen on coronal sequences. Biomechanically, in terms of tibiofemoral contact pressures, this injury is most equivalent to which of the following?
Explanation
Question 60
A 26-year-old professional hockey player presents with chronic groin pain exacerbated by deep hip flexion and internal rotation. A Dunn lateral radiograph is obtained, and the alpha angle is measured to be 68 degrees. This radiographic finding is most consistent with which of the following pathomorphologies?
Explanation
Question 61
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the surgeon utilizes intraoperative fluoroscopy to identify the anatomic femoral attachment site (Schöttle's point). Which of the following accurately describes the correct radiographic landmarks for this location on a strict lateral radiograph?
Explanation
Question 62
A 28-year-old marathon runner presents with persistent anterior knee pain. MRI and subsequent diagnostic arthroscopy reveal a symptomatic, 4.5 cm² full-thickness unipolar chondral defect on the weight-bearing surface of the medial femoral condyle. He has failed exhaustive nonoperative management. His mechanical alignment is neutral, and both menisci are intact. According to current treatment algorithms, what is the most appropriate primary cartilage restoration procedure?
Explanation
Question 63
A 23-year-old collegiate baseball pitcher requires an ulnar collateral ligament (UCL) reconstruction after suffering a complete rupture of the anterior bundle. During reconstruction using the docking technique, the surgeon aims to anatomically recreate the primary restraint to valgus stress. To which specific anatomic footprints must the graft be secured to accurately recreate the anterior bundle of the UCL?
Explanation
Question 64
A 31-year-old male sustains a knee dislocation (Schenck KD-IIIL) after a high-speed motorcycle accident. On initial presentation, he has an absent dorsalis pedis pulse with an ABI of 0.6, and a profound 'foot drop' with absent sensation in the first web space. Following a successful vascular bypass, orthopedic ligamentous reconstruction is planned. Which of the following statements regarding his neurologic deficit is most accurate?
Explanation
Question 65
A 35-year-old competitive weightlifter presents to the emergency department with acute severe pain, swelling, and ecchymosis over the right anterior axilla and medial arm. He reports feeling a sudden 'tearing' sensation at the bottom phase of a maximal bench press. Physical examination demonstrates a notable loss of the anterior axillary contour. Based on the biomechanics of this injury pattern, which portion of the pectoralis major muscle is placed under the greatest tension during this movement and most commonly ruptures first?
Explanation
Question 66
A 24-year-old professional soccer player presents with recurrent knee instability 2 years after an arthroscopic anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. He reports a 'giving way' episode without a new traumatic event. A sagittal MRI from his recent evaluation is shown in Figure 1.
What is the most common etiology for early clinical failure of this reconstructed ligament?
Explanation
Question 67
During the arthroscopic repair of a Type II Superior Labrum Anterior to Posterior (SLAP) tear in a 21-year-old collegiate baseball pitcher, anchors are placed to secure the labrum. To avoid altering the complex biomechanics of the superior labrum and to minimize postoperative stiffness, anchor placement should strictly avoid which of the following areas?
Explanation
Question 68
A 20-year-old collegiate baseball pitcher presents with medial elbow pain that occurs predominantly during the late cocking and early acceleration phases of throwing. On physical examination, the moving valgus stress test is markedly positive. Magnetic resonance imaging confirms a high-grade partial tear of the ulnar collateral ligament (UCL), and he elects to undergo UCL reconstruction. Which bundle of the UCL is the primary restraint to valgus stress, and what is its true anatomic footprint?
Explanation
Question 69
A 24-year-old male hockey player presents with chronic, deep groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a pistol-grip deformity. A coronal T2-weighted MRI of his right hip is shown in Figure 11.
During arthroscopic intervention for this condition, where is the most common location of concomitant articular cartilage damage expected to be found?

Explanation
Question 70
A 32-year-old weightlifter presents with right shoulder pain and weakness after feeling a clunk during a heavy bench press exercise. He reports difficulty externally rotating the arm. A modified axillary radiograph is provided in Figure 5.
Imaging reveals a reverse Hill-Sachs lesion that involves approximately 25% of the articular surface. What is the most appropriate surgical management?
Explanation
Question 71
A 26-year-old rugby player sustained a direct blow to the anteromedial aspect of his knee while it was fully extended. On physical examination, he demonstrates 15 degrees of increased external tibial rotation at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of flexion, the external rotation side-to-side difference is only 3 degrees. Which of the following structures is most likely injured?
Explanation
Question 72
A 19-year-old elite collegiate basketball player sustains a fracture at the metaphyseal-diaphyseal junction of the fifth metatarsal. He undergoes intramedullary screw fixation to expedite return to play. The high risk of nonunion in this specific fracture pattern is primarily attributed to a watershed vascular zone. From which aspect does the primary nutrient artery enter the fifth metatarsal to supply this area?
Explanation
Question 73
A 17-year-old gymnast undergoes a medial patellofemoral ligament (MPFL) reconstruction using a semitendinosus autograft for recurrent patellar dislocations. The surgeon uses fluoroscopy to identify Schöttle's point for the femoral anchor placement. Which of the following best describes the radiographic landmarks for the anatomic femoral attachment of the MPFL on a true lateral radiograph?
Explanation
Question 74
A 40-year-old marathon runner feels a sudden pop in the posterior aspect of his knee while decelerating. MRI demonstrates a complete radial tear at the posterior root of the medial meniscus. If left untreated, this specific injury pattern most closely mimics the biomechanical effects of which of the following?
Explanation
Question 75
A 35-year-old recreational tennis player presents with acute posterior ankle pain after lunging for a drop shot. He has a positive Thompson test. An MRI of the ankle is shown in Figure 7.
He elects to undergo minimally invasive surgical repair of the Achilles tendon. During percutaneous suture passage in the proximal stump, which nerve is at the greatest risk of iatrogenic injury?
Explanation
Question 76
A 25-year-old athlete sustains a high-energy knee dislocation during a football game. Magnetic resonance imaging demonstrates complete tears of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), and the posteromedial corner (PMC). The patient undergoes single-stage multi-ligament knee reconstruction 3 weeks post-injury. What is the most common complication following surgical treatment of a multi-ligament knee injury?
Explanation
Question 77
A 30-year-old competitive weightlifter feels a sudden, painful 'pop' in his anterior chest wall while performing a heavy bench press. Physical examination reveals ecchymosis, loss of the anterior axillary fold, and notable weakness in internal rotation and adduction of the humerus. MRI confirms a complete tear of the pectoralis major at its humeral insertion. What is the optimal management for this patient?
Explanation
Question 78
A 21-year-old rugby player presents with recurrent anterior shoulder instability following an initial dislocation one year ago. A 3D reconstructed CT scan of the glenoid demonstrates an 'inverted pear' appearance with approximately 26% anterior bone loss.
What is the most appropriate surgical intervention to prevent recurrent instability?
Explanation
Question 79
A 22-year-old collegiate baseball pitcher undergoes ulnar collateral ligament (UCL) reconstruction utilizing a palmaris longus autograft (Tommy John surgery). Which of the following is the most frequent postoperative complication associated with this procedure in overhead throwers?
Explanation
Question 80
A 45-year-old woman experiences a sudden 'pop' in the back of her knee while squatting. MRI demonstrates a medial meniscus posterior root tear and localized marrow edema in the medial femoral condyle. What is the primary biomechanical consequence of leaving this root tear untreated?
Explanation
Question 81
During hip arthroscopy for a 28-year-old hockey player with femoroacetabular impingement (FAI), an osteochondroplasty is performed for a large cam lesion at the femoral head-neck junction. Resection of more than what percentage of the femoral neck diameter substantially increases the risk of an iatrogenic postoperative femoral neck fracture?
Explanation
Question 82
A 14-year-old female gymnast presents with lateral elbow pain, clicking, and a 15-degree extension deficit. Radiographs demonstrate a lucency in the capitellum. MRI reveals an osteochondral defect with high T2 signal fluid surrounding the fragment, indicating instability. Her capitellar physis is open. What is the recommended treatment?
Explanation
Question 83
A 24-year-old recreational soccer player sustains an acute anterior cruciate ligament (ACL) rupture. During a subsequent gait analysis assessment, which of the following kinematic adaptations is most characteristic of a classic ACL-deficient 'quadriceps avoidance gait' during the stance phase?
Explanation
Question 84
A 35-year-old woman presents with persistent anterior hip pain. Imaging shows a positive crossover sign, a center-edge angle of 45 degrees, and a labral tear. Which of the following is the defining pathomechanical feature of this specific type of femoroacetabular impingement (FAI)?
Explanation
Question 85
A 28-year-old cyclist falls directly onto his shoulder. Radiographs show superior displacement of the distal clavicle.
Measurements reveal the coracoclavicular distance is increased by 150% compared to the contralateral side. According to the Rockwood classification, what type of acromioclavicular (AC) joint injury is this, and what is the typical recommended management?

Explanation
Question 86
A 25-year-old professional hockey player sustains a high-grade acromioclavicular (AC) joint separation and is scheduled for coracoclavicular (CC) ligament reconstruction. To accurately recreate the native anatomy, the surgeon must be aware of the specific insertion footprints of the CC ligaments. Which of the following describes the anatomical insertion of the conoid ligament relative to the trapezoid ligament on the clavicle?
Explanation
Question 87
A 22-year-old collegiate soccer player is evaluated for posterolateral knee pain and a feeling of instability after a twisting injury. On physical examination, the dial test demonstrates 15 degrees of increased external rotation compared to the contralateral normal knee at 30 degrees of knee flexion, but symmetric external rotation at 90 degrees of knee flexion. This finding is most indicative of an isolated injury to which of the following structures?
Explanation
Question 88
A 24-year-old male presents with deep groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a 'pistol grip' deformity of the proximal femur. Which of the following radiographic parameters is most diagnostic of the Cam-type femoroacetabular impingement (FAI) suspected in this patient?
Explanation
Question 89
A 28-year-old overhead throwing athlete presents with deep shoulder pain and clicking. An MRI is obtained as shown in Figure 4.
After failing conservative management, he undergoes arthroscopic repair for a Type II SLAP lesion. Which of the following portals provides the most optimal trajectory for anchor placement at the posterosuperior glenoid rim to address this pathology?

Explanation
Question 90
A 45-year-old recreational athlete feels a 'pop' in the back of his knee while performing a deep squat. MRI reveals a complete posterior root tear of the medial meniscus. According to biomechanical studies, leaving a complete posterior root tear of the medial meniscus unrepaired is biomechanically equivalent to which of the following?
Explanation
Question 91
A 21-year-old collegiate baseball pitcher reports medial elbow pain and decreased velocity during the late cocking and early acceleration phases of throwing. An MRI is shown in Figure 15.
He undergoes an ulnar collateral ligament (UCL) reconstruction using a docking technique. During the surgical exposure, the surgeon utilizes a muscle-splitting approach through the flexor-pronator mass. Care must be taken to identify and protect which of the following cutaneous nerves to prevent painful neuroma formation?
Explanation
Question 92
A 55-year-old man presents with right shoulder weakness after a fall on an outstretched arm. He specifically complains of difficulty tucking in his shirt behind his back and bringing his hand to his abdomen. Physical examination reveals a positive bear-hug test and increased passive external rotation compared to the contralateral side. Which of the following special tests is also most likely to be positive in this patient?
Explanation
Question 93
A 19-year-old competitive skier sustains a twisting injury to her left knee. A radiograph reveals a small avulsion fracture of the lateral aspect of the proximal tibia, known as a Segond fracture.
This specific radiographic finding is highly associated with an anterior cruciate ligament (ACL) tear and represents a bony avulsion of which of the following structures?
Explanation
Question 94
A 28-year-old physically active female presents with a 3.5 cm² symptomatic, unipolar, full-thickness chondral defect on the medial femoral condyle. She has failed 6 months of non-operative management. Diagnostic arthroscopy reveals normal mechanical alignment, an intact meniscus, and a stable knee. Which of the following surgical interventions is most appropriate to provide hyaline-like cartilage restoration for a defect of this size?
Explanation
Question 95
A 25-year-old professional baseball pitcher presents with vague posterior shoulder pain and a noted decrease in pitching velocity. Physical exam reveals a Glenohumeral Internal Rotation Deficit (GIRD) of 25 degrees compared to the non-throwing shoulder, along with a loss of total arc of motion. What is the most common pathomechanical cause of symptomatic GIRD contributing to internal impingement in the overhead throwing athlete?
Explanation
Question 96
A 17-year-old female high school soccer player tears her ACL during a game. She and her parents are discussing graft options for surgical reconstruction. What is the most accurate information regarding the use of bone-patellar tendon-bone (BPTB) allograft compared to BPTB autograft in this specific patient population?
Explanation
Question 97
A 22-year-old male rugby player presents with recurrent anterior shoulder instability after a primary dislocation 2 years ago. He reports 5 subsequent dislocations requiring closed reduction. A 3D CT scan of the shoulder is shown in Figure 14, demonstrating an 'inverted pear' glenoid with 27% anterior bone loss. What is the most appropriate definitive management?

Explanation
Question 98
A 30-year-old male sustains a severe knee hyperextension injury during American football, resulting in a knee dislocation. After closed reduction, his vascular exam is normal with biphasic pulses, but he exhibits a profound foot drop and absent sensation in the first web space. An MRI shown in Figure 5 demonstrates complete disruption of the ACL, PCL, and posterolateral corner (PLC). Which of the following anatomical structures is most closely associated with the pathway of the injured nerve and serves as a critical surgical landmark?
Explanation
Question 99
A 24-year-old male collegiate hockey player complains of insidious onset, worsening deep right groin pain that is exacerbated by prolonged sitting and deep hip flexion. A radiograph is shown in Figure 19, demonstrating an abnormal alpha angle of 65 degrees. What is the primary pathophysiologic mechanism of chondral injury in this specific morphological variant of femoroacetabular impingement (FAI)?

Explanation
Question 100
A 21-year-old collegiate baseball pitcher underwent a right elbow ulnar collateral ligament (UCL) reconstruction using a palmaris longus autograft 6 weeks ago. He now presents with persistent tingling in his small and ring fingers, as well as subjective weakness when gripping. Which intraoperative factor or surgical step is most commonly associated with this specific postoperative complication?
Explanation
None
