Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 4)

Key Takeaway
This topic focuses on Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 4), Top-rated Orthopedic Upper Extremity 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 52-year-old man has shoulder pain and stiffness after undergoing a "mini-lateral" rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/mm3 (normal 3,500 to 10,500/mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
Question 2
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
Question 3
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
Question 4
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a "pop" in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
Question 5
When comparing the addition of a trough at the greater tuberosity to direct repair of cortical bone, simulated rotator cuff repair in animal models has shown what type of change in the strength of the repair?
Explanation
Question 6
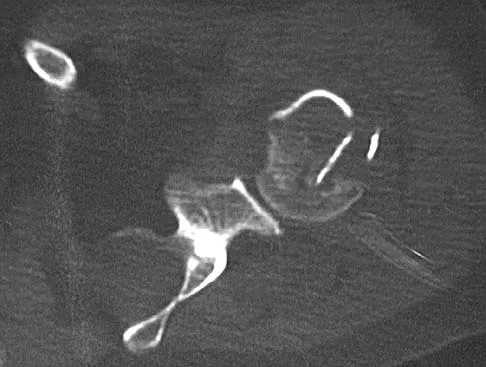
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of
Explanation
Question 7
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?
Explanation
Question 8
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
Question 9
Which of the following best describes the most common anatomic variation seen in the glenoid labrum and the middle glenohumeral ligament in the anterosuperior quadrant of the shoulder??
Explanation
Question 10
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
Explanation
Question 11
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?
Explanation
Question 12
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
Question 13
Which of the following statements best describes the relationship between tissue response to thermal capsulorrhaphy and the type of device used?
Explanation
Question 14
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
Question 15
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Question 16
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
Explanation
Question 17
A 65-year-old woman landed on her nondominant left shoulder in a fall. An AP radiograph is shown in Figure 39. Management should consist of
Explanation
Question 18
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
Question 19
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of
Explanation
Question 20
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of
Explanation
Question 21
After closed reduction of the dislocation shown in Figure 42, it is essential to avoid placing the upper extremity in what position for the first 4 to 6 weeks?
Explanation
Question 22
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
Question 23
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
Question 24
A 38-year-old woman who tripped and fell on her outstretched arm reports pain with movement. Examination reveals swelling. AP and lateral radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
Question 25
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
Question 26
In a reverse total shoulder arthroplasty (RTSA), the center of rotation is altered compared to the native glenohumeral joint. This specific kinematic alteration achieves which of the following biomechanical advantages?
Explanation
Question 27
A 42-year-old woman presents after a fall onto an outstretched hand. She is diagnosed with a 'terrible triad' injury of the elbow. During surgical reconstruction, what is the most widely accepted and appropriate sequence of repair to restore elbow stability?
Explanation
Question 28
A 24-year-old elite volleyball attacker complains of vague posterior shoulder pain and painless weakness over the past 6 months. Physical examination reveals notable atrophy of the infraspinatus fossa but normal bulk of the supraspinatus. She has full strength in shoulder abduction but 3/5 strength in external rotation with the arm at the side. An MRI is obtained, demonstrating a paralabral cyst. Where is the cyst most likely located and which nerve is affected?
Explanation
Question 29
A 65-year-old woman falls and sustains a complex proximal humerus fracture. According to the criteria established by Hertel et al., which combination of radiographic findings is the most reliable predictor of humeral head ischemia?
Explanation
Question 30
A 45-year-old man presents with numbness and tingling in his small and ring fingers, along with subjective weakness in his grip. Electromyography confirms isolated ulnar neuropathy at the elbow. During surgical decompression, which of the following structures is identified as the most common primary site of ulnar nerve compression?
Explanation
Question 31
A 22-year-old man falls on an outstretched hand and sustains a minimally displaced fracture of the proximal pole of the scaphoid. He is counseled regarding the high risk for nonunion and avascular necrosis (AVN). Which of the following accurately describes the primary arterial blood supply to the proximal pole of the scaphoid?
Explanation
Question 32
A 58-year-old woman is evaluated 6 months after open reduction and internal fixation of a distal radius fracture utilizing a volar locking plate. She reports a sudden inability to actively flex the interphalangeal joint of her thumb, which occurred painlessly while wringing out a towel. What is the most likely cause of this complication?
Explanation
Question 33
A 42-year-old tennis player presents with chronic, refractory lateral elbow pain that is exacerbated by wrist extension and gripping. He has failed 8 months of conservative management and is scheduled for surgical debridement. Histologic evaluation of the resected tissue is expected to show angiofibroblastic hyperplasia. The primary pathoanatomic lesion in this condition typically involves the origin of which structure?
Explanation
Question 34
A 26-year-old professional baseball pitcher undergoes shoulder arthroscopy for a Type II SLAP tear. During dynamic intraoperative testing, the surgeon observes a 'peel-back' mechanism of the superior labrum when the arm is placed in the late-cocking position (abduction and external rotation). This biomechanical phenomenon most directly leads to which of the following secondary shoulder pathologies in overhead athletes?
Explanation
Question 35
A 20-year-old collegiate baseball pitcher is undergoing ulnar collateral ligament (UCL) reconstruction utilizing an autograft. To minimize the risk of postoperative ulnar neuropathy, a common and devastating complication, which of the following intraoperative principles is most critical regarding the handling of the ulnar nerve?
Explanation
Question 36
A 45-year-old man presents with chronic, progressive wrist pain 10 years after sustaining an untreated fall on an outstretched hand. Radiographs demonstrate a scaphoid waist nonunion with cystic changes and sclerosis, alongside marked narrowing of the radioscaphoid and capitolunate joint spaces. The radiolunate joint is well-preserved. Which of the following is the most appropriate surgical management?
Explanation
Question 37
Reverse total shoulder arthroplasty (RTSA) is widely utilized to restore function in patients with rotator cuff tear arthropathy. Compared to the native glenohumeral joint, how does RTSA alter the center of rotation to improve active elevation?
Explanation
Question 38
A 35-year-old woman is undergoing surgery for a 'terrible triad' injury of the elbow (elbow dislocation, radial head fracture, and coronoid fracture). Intraoperatively, the coronoid has been securely fixed, the radial head has been replaced, and the lateral collateral ligament (LCL) complex has been repaired to the lateral epicondyle. Upon testing range of motion, the elbow remains unstable and subluxates in terminal extension. What is the next most appropriate step in management?
Explanation
Question 39
A 62-year-old woman presents with the sudden inability to bend the tip of her thumb. Twelve months prior, she underwent open reduction and internal fixation of a distal radius fracture with a volar locking plate. Lateral radiographs show the plate is positioned prominent and distal to the watershed line. Given the likely diagnosis, what is the most appropriate surgical treatment?
Explanation
Question 40
A 42-year-old mechanic complains of clumsiness, weakness in his grip, and numbness in his small and ring fingers. During physical examination, the examiner asks the patient to hold a piece of paper laterally between his thumb and index finger. As the examiner pulls the paper away, the patient strongly flexes the interphalangeal (IP) joint of his thumb. Which muscle is compensating to produce this clinical sign?
Explanation
Question 41
A 74-year-old female sustains a displaced 3-part proximal humerus fracture with varus impaction of the head. Bone density testing indicates significant osteoporosis. If the surgeon decides to proceed with open reduction and internal fixation (ORIF) using a locked plate rather than arthroplasty, what is the most common complication she is at risk for postoperatively?
Explanation
Question 42
A 45-year-old male bodybuilder undergoes a single-incision anterior approach for the repair of a complete distal biceps tendon rupture. Postoperatively, he complains of numbness over the radial aspect of his forearm. Which nerve was most likely injured or stretched during the surgical exposure?
Explanation
Question 43
A 32-year-old male presents with chronic dorsal wrist pain and weakened grip strength. Radiographs reveal sclerosis, cystic changes, and early fragmentation of the lunate, consistent with Kienböck's disease (Lichtman Stage IIIA). Ulnar variance is measured at -3 mm. MRI confirms the articular cartilage of the radiocarpal and midcarpal joints remains intact. What is the most appropriate surgical intervention?
Explanation
Question 44
A 22-year-old motorcyclist sustains a traumatic brachial plexus injury following a high-speed collision. He presents with a completely flail and insensate right upper extremity. Physical examination reveals right-sided ptosis, miosis, and anhidrosis. What does this constellation of signs definitively indicate regarding his nerve injury?
Explanation
Question 45
A 28-year-old professional tennis player presents with posterior shoulder pain and selective weakness in external rotation. An MRI of the shoulder reveals a multi-lobulated paralabral cyst located strictly within the spinoglenoid notch. Based on this isolated compression, which of the following clinical findings would most likely be observed on physical examination?
Explanation
Question 46
A 22-year-old male presents with a proximal pole scaphoid fracture after a fall. Operative fixation is planned. Which of the following is true regarding the surgical approach and relevant anatomy for this specific fracture pattern?
Explanation
Question 47
A 60-year-old woman sustained a nondisplaced distal radius fracture treated in a short arm cast. Six weeks later, she develops a sudden inability to actively extend her thumb interphalangeal joint. What is the most likely pathomechanism of this complication?
Explanation
Question 48
A 72-year-old woman undergoes reverse total shoulder arthroplasty for cuff tear arthropathy. At her 2-year follow-up, radiographs show inferior scapular notching. Which of the following component positionings is most strongly associated with this radiographic finding?
Explanation
Question 49
A 45-year-old man undergoes repair of a distal biceps tendon rupture via a dorsal and volar two-incision technique. Postoperatively, he is unable to actively extend his fingers and thumb, but wrist extension is preserved with radial deviation. Which nerve is most likely injured, and what is its anatomic relationship in the forearm?
Explanation
Question 50
A 35-year-old man falls from a ladder and sustains a 'terrible triad' injury of the elbow. Which of the following lists the sequence of structures typically addressed during surgical management, from deep to superficial?
Explanation
Question 51
A 55-year-old manual laborer presents with chronic, progressively worsening radial-sided wrist pain. Radiographs demonstrate advanced narrowing of the radioscaphoid joint and capitulolunate joint, with a preserved radiolunate joint. Which of the following is the most appropriate surgical treatment?
Explanation
Question 52
A 65-year-old woman sustains an intra-articular distal humerus fracture (AO type 13-C3). Open reduction and internal fixation is performed with dual plating. Which of the following statements regarding the biomechanical stability of plating configurations is most accurate?
Explanation
Question 53
A 28-year-old carpenter presents with dorsal wrist pain. MRI confirms osteonecrosis of the lunate. Radiographs demonstrate lunate sclerosis and fragmentation, but the carpal height ratio is preserved and there is no radioscaphoid arthritis. Ulnar variance is -3mm. Which of the following is the most appropriate operative intervention?
Explanation
Question 54
A 45-year-old diabetic man presents with persistent ulnar neuropathy 6 months after an in situ ulnar nerve decompression at the cubital tunnel. EMG shows active denervation in the abductor digiti minimi. During revision surgery, the nerve is embedded in dense scar tissue and subluxates anteriorly with elbow flexion. Which of the following is the most appropriate next step?
Explanation
Question 55
A 22-year-old collegiate baseball pitcher presents with deep shoulder pain and decreased throwing velocity. He has a positive O'Brien test and dynamic labral shear test. MRI arthrogram shows a type II SLAP tear. Following 3 months of failed physical therapy, what is the most appropriate surgical treatment?
Explanation
Question 56
A 68-year-old woman presents with persistent shoulder pain and pseudoparalysis. MRI reveals a massive rotator cuff tear involving the supraspinatus and infraspinatus. Which of the following MRI findings is the strongest contraindication to a primary arthroscopic repair?
Explanation
Question 57
A 32-year-old man sustained a closed midshaft humerus fracture and presents with an inability to extend his wrist or fingers. He is treated nonoperatively with a functional brace. At 3 months, his fracture shows progressive healing, but there is no clinical or electromyographic (EMG) evidence of radial nerve recovery. What is the most appropriate next step in management?
Explanation
Question 58
A 45-year-old woman falls on an outstretched hand and sustains an acute 'terrible triad' injury of the elbow.
During surgical reconstruction, after fixation of the coronoid and radial head fractures and repair of the lateral collateral ligament (LCL) complex, the elbow remains persistently unstable in extension. What is the next most appropriate step in surgical management?

Explanation
Question 59
A 75-year-old right-hand-dominant woman sustains a 4-part proximal humerus fracture. She has a history of severe osteoporosis and advanced osteoarthritis of the glenohumeral joint. Which of the following surgical options will provide the most reliable pain relief and functional improvement?
Explanation
Question 60
A 22-year-old male cyclist falls onto his left shoulder and sustains a completely displaced midshaft clavicle fracture with 2.5 cm of shortening. He undergoes open reduction and internal fixation (ORIF) with a superiorly placed precontoured locking plate. Which of the following nerves is at greatest risk of injury during the surgical approach?
Explanation
Question 61
A 40-year-old male weightlifter feels a sudden 'pop' in his anterior elbow while performing a heavy bicep curl. On examination, he has weakness in forearm supination and elbow flexion. He undergoes a single-incision anterior approach for distal biceps tendon repair. Which of the following complications is most specifically associated with this single-incision approach?
Explanation
Question 62
A 24-year-old man falls on an outstretched hand. Initial radiographs are negative, but an MRI obtained 2 weeks later confirms a non-displaced proximal pole scaphoid fracture. Due to the high risk of nonunion, surgical fixation is recommended. The blood supply to the proximal pole of the scaphoid is primarily derived from branches of which of the following arteries?
Explanation
Question 63
A 19-year-old male presents to the emergency department with severe chest pain, shortness of breath, and dysphagia after being tackled during a rugby match. Examination reveals a depression at the right sternoclavicular joint. A CT scan confirms a posterior sternoclavicular dislocation. What is the most appropriate initial management?
Explanation
Question 64
A 55-year-old male manual laborer undergoes an open subpectoral biceps tenodesis for partial tearing of the long head of the biceps tendon. Which of the following represents a known advantage of open subpectoral biceps tenodesis compared to an arthroscopic suprapectoral tenodesis?
Explanation
Question 65
A 50-year-old woman with type 1 diabetes mellitus presents with insidious onset of progressive shoulder pain and stiffness over the last 4 months. She denies any preceding trauma. Examination shows equal limitation in both active and passive range of motion, with significant restriction in external rotation. Radiographs are normal. What is the underlying pathophysiological hallmark of her condition?
Explanation
Question 66
A 72-year-old woman with a massive, irreparable rotator cuff tear and pseudoparalysis undergoes a reverse total shoulder arthroplasty. During glenoid baseplate preparation, which of the following positioning strategies is most effective in minimizing the risk of scapular notching?
Explanation
Question 67
A 45-year-old recreational weightlifter presents with deep, anterior shoulder pain exacerbated by bench pressing. He has a positive O'Brien test and a positive Speed's test. MRI reveals a type II SLAP tear. Nonoperative management has failed. Which of the following surgical interventions provides the most reliable return to his pre-injury activity level?
Explanation
Question 68
A 32-year-old man falls from a ladder and sustains an elbow dislocation associated with a radial head fracture and a coronoid fracture. Following closed reduction of the elbow, he is taken to the operating room. What is the standard recommended sequence of surgical reconstruction for this injury?
Explanation
Question 69
A 24-year-old man falls on an outstretched hand and sustains a fracture of the scaphoid. The fracture line passes through the proximal pole. He is at high risk for avascular necrosis due to the unique blood supply of the scaphoid. The predominant blood supply to the proximal pole is derived from a retrograde flow pattern originating from which of the following vessels?
Explanation
Question 70
A 21-year-old collegiate baseball pitcher presents with medial elbow pain and decreased pitching velocity. Physical examination demonstrates pain and laxity with the moving valgus stress test. An MRI arthrogram confirms a tear of the ulnar collateral ligament (UCL). Which specific bundle of the UCL is the primary restraint to valgus stress from 30 to 120 degrees of elbow flexion?
Explanation
Question 71
A 28-year-old motorcyclist is involved in a high-speed collision and sustains a severe traction injury to his right upper extremity. On examination, he has a flail, insensate right arm. He also exhibits right-sided ptosis, miosis, and anhidrosis. The presence of these ocular and facial symptoms strongly suggests an injury at which of the following levels?
Explanation
Question 72
A 55-year-old woman presents with sudden inability to actively flex the interphalangeal joint of her right thumb. She underwent open reduction and internal fixation of a right distal radius fracture with a volar locking plate 4 years ago. Radiographs show the plate is positioned distally, overriding the watershed line. Which of the following is the most appropriate definitive management for her current condition?
Explanation
Question 73
A 42-year-old carpenter presents with chronic lateral elbow pain that worsens with gripping and resisted wrist extension. Nonoperative management over the past 12 months has failed, and he is scheduled for surgical debridement. The pathologic tissue in lateral epicondylitis most commonly involves the origin of which of the following muscles?
Explanation
Question 74
A 35-year-old man sustains a closed spiral fracture of the distal third of the humeral shaft following an arm-wrestling match. On initial presentation in the emergency department, he is unable to actively extend his wrist or fingers, and he has decreased sensation over the dorsal first web space. Radiographs confirm a Holstein-Lewis fracture. What is the most appropriate initial management?
Explanation
Question 75
A 28-year-old mechanic complains of an inability to pinch objects using his right thumb and index finger. On examination, when asked to make an 'OK' sign, he compensates by using the pulps of his thumb and index finger rather than the tips, resulting in a flat pinch. Sensation in the hand is completely normal. Which of the following muscles is most likely paralyzed?
Explanation
Question 76
A 65-year-old right-hand-dominant woman presents after a fall onto an outstretched hand. Radiographs demonstrate a displaced intra-articular distal radius fracture with a volar marginal shear fragment.
Which of the following approaches and fixation constructs is most appropriate to prevent carpal subluxation?

Explanation
Question 77
A 45-year-old man falls from a ladder and sustains an elbow dislocation. After closed reduction in the emergency department, radiographs are obtained as shown in the provided figure.
A subsequent CT scan confirms a type II coronoid fracture and a comminuted radial head fracture. During surgical intervention, what is the most appropriate sequence of repair to restore elbow stability?
Explanation
Question 78
A 72-year-old woman sustains a shoulder injury after a mechanical fall.
Assuming this is a severely comminuted 4-part proximal humerus fracture with varus impaction and severe osteoporosis, which of the following is the strongest predictor of postoperative complications if treated with open reduction and internal fixation (ORIF) utilizing a locked plate?
Explanation
Question 79
A 28-year-old laborer presents with progressive dorsal radial wrist pain 3 years after a fall. He did not seek medical attention initially. Radiographs and an MRI confirm a scaphoid waist nonunion with radioscaphoid arthritis and capitolunate arthritis, but the radiolunate joint is preserved.
What is the most appropriate surgical treatment?

Explanation
Question 80
A 55-year-old male complains of numbness and tingling in his small and ring fingers that awakens him at night. Examination shows a positive Tinel's sign at the elbow and a positive Froment's sign. He has clinically palpable snapping over the medial epicondyle during elbow flexion. Electrodiagnostic studies confirm severe ulnar neuropathy at the elbow. He fails a 6-month trial of conservative management.
What is the primary indication for choosing an anterior transposition of the ulnar nerve over an in situ decompression in this patient?

Explanation
Question 81
A 22-year-old elite collegiate baseball pitcher presents with vague posterior shoulder pain during the late cocking and early acceleration phases of throwing.
Physical examination reveals a loss of 25 degrees of internal rotation in the throwing arm compared to the contralateral side. He has a positive apprehension test that is relieved by a relocation maneuver. What is the most likely underlying pathophysiology of his pain?

Explanation
Question 82
A 35-year-old mechanic presents with chronic, progressive dorsal wrist pain and decreased grip strength.
Imaging demonstrates sclerosis and fragmentation of the lunate with negative ulnar variance, but no fixed carpal collapse (Lichtman Stage IIIA). What is the most appropriate initial surgical intervention?

Explanation
Question 83
A 75-year-old woman with long-standing rheumatoid arthritis presents with debilitating right shoulder pain and an inability to lift her arm above 60 degrees.
Radiographs show severe glenohumeral osteoarthritis with massive superior migration of the humeral head, articulating with the acromion. She has an intact deltoid muscle but a massive, irreparable rotator cuff tear. What is the most appropriate definitive management?

Explanation
Question 84
A 29-year-old male cyclist falls directly onto his left shoulder. He presents with severe pain and a prominent distal clavicle.
Radiographs demonstrate a 150% superior displacement of the distal clavicle relative to the acromion, with the clavicle visibly protruding and tenting the trapezius fascia on clinical exam. What is the diagnosis and recommended treatment?

Explanation
Question 85
A 6-year-old boy falls from the monkey bars and presents with a swollen, painful forearm.
Radiographs reveal a plastic deformation and fracture of the proximal ulnar shaft accompanied by an anterior dislocation of the radial head. Which of the following nerves is at greatest risk of injury with this specific fracture pattern?

Explanation
Question 86
A 72-year-old woman presents 3 years after a reverse total shoulder arthroplasty with progressive shoulder pain. Radiographs are shown in Figure 1. What factor most contributes to the complication seen (scapular notching)?
Explanation
Question 87
A 45-year-old man falls onto his outstretched hand and sustains the injury shown in Figure 2. Which of the following is the most appropriate surgical sequence for managing this injury?
Explanation
Question 88
A 65-year-old woman sustains a distal radius fracture. The lateral radiograph (Figure 3) demonstrates a volarly displaced fracture fragment of the lunate facet ("volar teardrop"). Failure to adequately stabilize this specific fragment is most likely to result in which of the following complications?
Explanation
Question 89
A 24-year-old man sustains a scaphoid waist fracture. The vascular supply to the proximal pole of the scaphoid relies primarily on retrograde flow from vessels entering which aspect of the bone?
Explanation
Question 90
A 22-year-old collegiate baseball pitcher undergoes ulnar collateral ligament (UCL) reconstruction using a palmaris longus autograft. To minimize the risk of postoperative ulnar neuropathy, which of the following techniques or principles is recommended during the surgical approach?
Explanation
Question 91
A 28-year-old professional volleyball player complains of vague posterior shoulder pain and weakness with external rotation. An MRI (Figure 4) demonstrates a paralabral cyst in the spinoglenoid notch. Which of the following physical examination findings is most likely present?
Explanation
Question 92
A 60-year-old man undergoes arthroscopic rotator cuff repair. A Popeye deformity is a known potential outcome of biceps tenotomy. Compared to arthroscopic biceps tenodesis, which of the following is true regarding biceps tenotomy?
Explanation
Question 93
A 78-year-old woman with severe rheumatoid arthritis presents with a comminuted, intra-articular distal humerus fracture. Due to the severe osteopenia and joint destruction, she undergoes a total elbow arthroplasty (TEA). Which of the following is a recognized absolute contraindication for TEA in the setting of trauma?
Explanation
Question 94
A 13-year-old elite baseball pitcher presents with a 4-week history of gradual-onset shoulder pain during the cocking and early acceleration phases of pitching. Radiographs (Figure 5) reveal widening and irregularity of the proximal humeral physis. What is the most appropriate initial management for this patient?
Explanation
Question 95
A 29-year-old competitive weightlifter feels a 'pop' in his anterior axilla while performing a heavy bench press. Examination reveals bruising over the anterior arm and axilla, and weakness with adduction and internal rotation. He is diagnosed with a pectoralis major rupture. Which portion of the pectoralis major tendon is under the greatest tension during the eccentric phase of the bench press, making it most susceptible to injury?
Explanation
Question 96
A 35-year-old manual laborer presents with chronic radial-sided wrist pain that is exacerbated by heavy lifting. He reports a history of falling onto an outstretched hand 2 years ago, for which he did not seek medical attention. Radiographs reveal a scaphoid nonunion with advanced degenerative changes at both the radioscaphoid and capitolunate joints. The radiolunate joint space is well preserved. What is the most appropriate surgical management for this patient?
Explanation
Question 97
A 42-year-old woman sustains a highly unstable elbow injury after falling from a height. Radiographs demonstrate a posterolateral elbow dislocation associated with a comminuted radial head fracture and a type II coronoid fracture. Operative intervention is undertaken. After securely fixing the coronoid fracture and replacing the radial head with an arthroplasty component, the elbow remains unstable when brought into extension. What is the next most appropriate step in the surgical management?
Explanation
Question 98
A 28-year-old elite volleyball player complains of vague, deep-seated posterior shoulder pain and weakness with overhead activities. Examination demonstrates marked atrophy of the infraspinatus fossa but normal bulk and tone of the supraspinatus. Significant weakness is noted in external rotation with the arm at the side, but abduction strength is symmetrically intact. MRI of the shoulder reveals a paralabral cyst. Based on the physical examination, where is the cyst most likely located?
Explanation
Question 99
A 45-year-old mechanic presents with a 6-month history of numbness and tingling in his ring and small fingers, which worsens when he keeps his elbow flexed during telephone calls. Examination shows a strongly positive Tinel's sign over the posteromedial elbow and a positive Froment's sign. Electromyography confirms severe ulnar neuropathy isolated to the elbow. During a surgical ulnar nerve release, the primary site of compression is identified between the humeral and ulnar heads of the flexor carpi ulnaris (FCU). What anatomical structure forms the roof of this specific compression site?
Explanation
Question 100
A 72-year-old woman undergoes a reverse total shoulder arthroplasty (RTSA) for severe rotator cuff tear arthropathy. The design of the prosthesis fundamentally alters the biomechanics of the glenohumeral joint to compensate for the absent rotator cuff. According to the original Grammont design principles, how is the center of rotation (COR) of the glenohumeral joint altered compared to the native anatomic state?
Explanation
None
