Orthopedic Basic 2026 MCQs: Board Review Questions & Answers (Part 4)
Key Takeaway
This topic focuses on Orthopedic Basic 2026 MCQs: Board Review Questions & Answers (Part 4), Top-rated Orthopedic Basic 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Basic 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
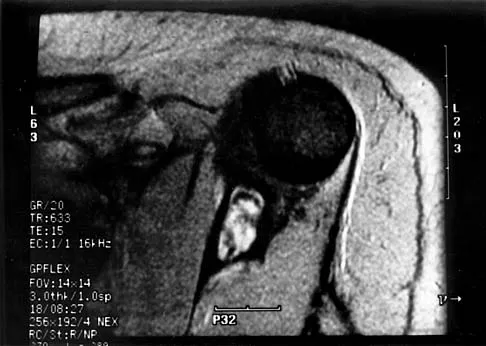
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
Question 2
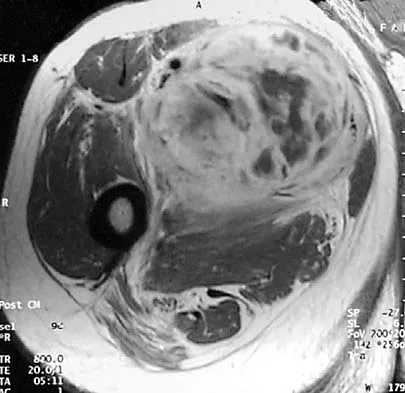
A 13-year-old boy has had a painless mass in the arm for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 46a through 46c. What is the most likely diagnosis?
Explanation
Question 3
A 20-year-old man has a symptomatic lesion of fibrous dysplasia in the femoral neck. Management should consist of
Explanation
Question 4
In addition to radiographs of the primary lesion and chest, MRI of the primary lesion, and CT of the chest, staging studies for Ewing's sarcoma should include which of the following?
Explanation
Question 5
Which of the following conditions is transmitted by an autosomal dominant trait?
Explanation
Question 6
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?
Explanation
Question 7
A 50-year-old man with metastatic renal cell carcinoma has right hip pain. A radiograph and CT scan are shown in Figures 48a and 48b. The first step in management should consist of
Explanation
Question 8
What is the most common benign bone tumor in childhood?
Explanation
Question 9
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?
Explanation
Question 10
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
Question 11
A 23-year-old woman has had vague left knee pain for the past 6 months. A radiograph and CT scan are shown in Figures 50a and 50b. What is the most likely diagnosis?
Explanation
Question 12
What is the preferred treatment of a patient with breast cancer and a pathologic fracture of the clavicle in her dominant arm?
Explanation
Question 13
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include
Explanation
Question 14
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
Question 15
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
Question 16
A 25-year-old woman has had pain and stiffness in her knee following a motor vehicle accident 9 months ago. The radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 53a through 53d. What is the most likely diagnosis?
Explanation
Question 17
Which of the following lesions most closely resembles Ewing's sarcoma histologically?
Explanation
Question 18
Primary chondrosarcoma of bone most commonly occurs in which of the following locations?
Explanation
Question 19
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?
Explanation
Question 20
A 55-year-old man has had a mass in his right thigh for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 55a through 55c. What is the most likely diagnosis?
Explanation
Question 21
Figures 56a through 56c show the radiograph, CT scan, and biopsy specimen of a 44-year-old man who underwent chemotherapy and radiation therapy for lymphoma of the distal femur 20 years ago. His current problem is most likely related to
Explanation
Question 22
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
Question 23
Exostoses in which of the following anatomic locations is the most likely to undergo malignant transformation in a patient with multiple hereditary exostosis (MHE)?
Explanation
Question 24
Initial management of a pathologic fracture of the humerus secondary to a unicameral bone cyst should include
Explanation
Question 25
An 11-year-old child has Ewing's sarcoma of the femoral diaphysis with a small soft-tissue mass. Staging studies show no evidence of metastases. Treatment should consist of
Explanation
Question 26
A 15-year-old boy presents with progressive knee pain and a destructive, bone-forming lesion in the distal femoral metaphysis. A core biopsy confirms the diagnosis of high-grade, conventional osteosarcoma. Which of the following genetic alterations is most consistently associated with the underlying pathogenesis of this tumor?
Explanation
Question 27
A 12-year-old girl is evaluated for thigh pain and a low-grade fever. Radiographs reveal a permeative, diaphyseal lesion in the femur with a prominent 'onion skin' periosteal reaction. A biopsy shows sheets of monotonous small round blue cells. The primary translocation associated with this condition results in a fusion protein that acts as an aberrant transcription factor. Immunohistochemistry is most likely to show strong, diffuse membranous staining for which of the following markers?
Explanation
Question 28
A 14-year-old boy presents with a rapidly expanding, painful lesion in the proximal tibia. Radiographs show an eccentric, expansile, lytic lesion with a thin cortical shell. MRI reveals multiple fluid-fluid levels. Biopsy demonstrates blood-filled spaces lacking endothelial lining, separated by cellular fibrous septa containing multinucleated giant cells. Which of the following molecular abnormalities is considered the primary driver of this lesion?
Explanation
Question 29
A 35-year-old woman is diagnosed with a large, destructive, recurrent giant cell tumor of the sacrum with impending neurologic compromise. Surgical resection would result in significant morbidity, so her multidisciplinary oncology team initiates targeted medical therapy. What is the mechanism of action of the most appropriate pharmacological agent?
Explanation
Question 30
A 28-year-old woman complains of a painless, slow-growing mass at the posterior aspect of her knee. Radiographs reveal a dense, heavily ossified mass arising from the posterior surface of the distal femur. A radiolucent cleft separates part of the tumor from the underlying cortex. Histology shows low-grade malignant spindle cells between well-formed, thick bone trabeculae. What is the typical genetic amplification found in this condition?
Explanation
Question 31
A 55-year-old man presents with dull, aching shoulder pain. Radiographs reveal a large medullary cartilaginous lesion in the proximal humerus with 'rings and arcs' calcification and significant endosteal scalloping. Core needle biopsy shows increased cellularity, binucleate chondrocytes, and myxoid changes in the hyaline stroma. Recent molecular studies show that this malignancy shares a specific genetic mutation with benign solitary enchondromas. Which of the following genes is most likely mutated?
Explanation
Question 32
A 10-year-old boy presents for orthopedic evaluation. He has multiple palpable bony protuberances around his knees, ankles, and shoulders, short stature, and a progressive valgus deformity of his left knee. A skeletal survey confirms multiple osteochondromas. The genetic mutation most likely responsible for his condition leads to a direct defect in which of the following biological processes?
Explanation
Question 33
A 20-year-old woman has an impending pathologic fracture of the proximal femur due to a large, ground-glass, radiolucent lesion. She also has a history of precocious puberty and café-au-lait spots with irregular borders ('coast of Maine'). The underlying cellular defect involves:
Explanation
Question 34
A 24-year-old man presents with a deep, slow-growing soft tissue mass in his thigh. MRI shows a heterogeneous mass adjacent to, but not within, the knee joint capsule. Biopsy reveals a biphasic tumor containing both epithelial and spindle cell components. Which of the following chromosomal translocations is considered diagnostic for this sarcoma?
Explanation
Question 35
A 16-year-old boy experiences severe, throbbing leg pain that is consistently worse at night and dramatically relieved by taking ibuprofen. Radiographs demonstrate a diaphyseal cortical thickening in the anterior tibia with a 5-mm radiolucent nidus. The intense pain associated with this specific bone lesion is primarily mediated by the local overproduction of which of the following substances?
Explanation
Question 36
A 32-year-old woman presents with persistent knee pain. Radiographs show an eccentric, lytic epiphyseal lesion in the distal femur. A biopsy demonstrates mononuclear cells and multinucleated giant cells. Which of the following is the specific molecular target of the monoclonal antibody denosumab, which may be used in the medical management of this condition?
Explanation
Question 37
A 15-year-old boy is diagnosed with conventional high-grade osteosarcoma of the distal femur. He undergoes neoadjuvant chemotherapy followed by wide surgical resection. Which of the following factors is considered the most significant prognostic indicator for long-term survival in this patient?
Explanation
Question 38
A 12-year-old boy presents with progressive mid-thigh pain and swelling. Radiographs show a permeative diaphyseal lesion with an 'onion-skin' periosteal reaction. Biopsy reveals uniform small round blue cells. Cytogenetic analysis of this tumor is most likely to show which of the following translocations?
Explanation
Question 39
A 65-year-old man presents with generalized bone pain and a recent pathologic fracture of the proximal humerus. Laboratory studies show anemia, hypercalcemia, and renal insufficiency. Serum protein electrophoresis reveals a monoclonal spike. Which of the following is the most appropriate initial diagnostic imaging modality for staging his skeletal disease?
Explanation
Question 40
A 14-year-old girl presents with pain and swelling in her right shoulder. Radiographs demonstrate an expansile, eccentric lytic lesion in the proximal humerus metaphysis with a thin sclerotic rim. MRI shows multiple fluid-fluid levels. The pathogenesis of this lesion is most strongly associated with a rearrangement involving which of the following genes?
Explanation
Question 41
A 55-year-old man presents with a constant, dull ache in his right hip that worsens at night. Radiographs reveal a radiolucent lesion in the right ilium with intralesional stippled calcifications and endosteal scalloping. Biopsy confirms a grade II (intermediate-grade) conventional chondrosarcoma. What is the most appropriate management?
Explanation
Question 42
A 19-year-old man complains of severe right thigh pain that is worse at night and dramatically relieved by NSAIDs. Radiographs show a small radiolucent nidus surrounded by dense reactive sclerosis in the femoral diaphysis. If a biopsy of the nidus were performed, what would be the expected histologic finding?
Explanation
Question 43
A 9-year-old girl is evaluated for a limp and a discrepancy in leg length. Radiographs reveal a 'shepherd's crook' deformity of the proximal femur with a 'ground-glass' appearance. She also has irregularly bordered hyperpigmented skin macules and a history of precocious puberty. This condition is caused by a somatic activating mutation resulting in the overproduction of which intracellular signaling molecule?
Explanation
Question 44
An 8-year-old boy presents to the emergency department with arm pain after throwing a baseball. Radiographs show a minimally displaced pathologic fracture through a centrally located, completely lytic lesion in the proximal humerus metaphysis. A 'fallen leaf' sign is visible. What is the most appropriate initial management?
Explanation
Question 45
A 24-year-old woman presents with a slowly enlarging, painful mass around her left knee. MRI demonstrates a deeply seated, multilobulated soft-tissue mass in the popliteal fossa. Radiographs reveal focal stippled calcifications. Biopsy reveals a biphasic pattern of spindle cells and epithelial cells. What is the most common site of distant metastasis for this specific type of sarcoma?
Explanation
Question 46
A 14-year-old boy presents with a 3-month history of progressive thigh pain and swelling. Radiographs show a destructive diaphyseal lesion of the femur with a lamellated 'onion skin' periosteal reaction. A core needle biopsy reveals uniform sheets of small round blue cells with scant cytoplasm. Cytogenetic analysis of this tumor is most likely to show which of the following translocations?
Explanation
Question 47
A 45-year-old man presents with a painful mass in his proximal humerus. Radiographs demonstrate a lytic lesion with intralesional 'popcorn' calcifications and endosteal scalloping involving greater than 2/3 of the cortical thickness. Biopsy confirms a grade II chondrosarcoma. Which of the following represents the most appropriate and definitive management?
Explanation
Question 48
A 35-year-old woman is diagnosed with a giant cell tumor of the distal femur. Due to the proximity of the lesion to the articular surface, she is started on a course of denosumab therapy prior to intralesional curettage. Which of the following best describes the specific mechanism of action of this medication?
Explanation
Question 49
A 22-year-old man presents with a 6-month history of left knee pain that is significantly worse at night. The pain is dramatically relieved within 30 minutes of taking ibuprofen. Radiographs reveal a 1-cm radiolucent nidus surrounded by dense, reactive sclerotic bone in the proximal tibial diaphysis. Which of the following inflammatory mediators is most responsible for this classic pain pattern?
Explanation
Question 50
A 65-year-old man presents with new-onset severe lower back pain and generalized fatigue. Laboratory studies reveal a normocytic anemia, elevated serum creatinine, and hypercalcemia. A skeletal survey shows multiple 'punched-out' lytic lesions in the skull and pelvis with no surrounding reactive sclerosis. Which of the following factors is most directly responsible for the uncoupled bone remodeling that leads to these purely lytic lesions?
Explanation
Question 51
A 12-year-old boy is found to have an incidental lesion in the proximal humerus during a workup for shoulder stiffness. Radiographs show a centrally located, well-circumscribed radiolucent lesion in the metaphysis with mild cortical thinning. If a diagnostic aspiration of this intact lesion is performed, which of the following fluid characteristics is most classically expected?
Explanation
Question 52
A 28-year-old woman complains of a slowly enlarging, painful mass in her left foot over the past year. MRI reveals an indeterminate soft tissue mass, and plain radiographs demonstrate stippled calcifications within the substance of the mass. A core biopsy confirms synovial sarcoma. Which of the following represents the characteristic cytogenetic abnormality for this neoplasm?
Explanation
Question 53
A 68-year-old man with a known 15-year history of polyostotic Paget's disease presents with a 2-month history of rapidly worsening pain and swelling in his right thigh, a symptom notably different from his baseline. Radiographs demonstrate a destructive, mixed lytic and sclerotic lesion in the femoral diaphysis with a wide zone of transition, cortical breakthrough, and a soft tissue mass. What is the most likely diagnosis?
Explanation
Question 54
A 9-year-old girl undergoes a biopsy of an expansile, eccentrically located, lytic metaphyseal lesion in her proximal tibia. The MRI demonstrates multiple fluid-fluid levels. Histopathology describes cavernous, blood-filled spaces lacking a true endothelial lining, separated by fibrous septa containing multinucleated giant cells. Which of the following genetic alterations is most specific to the primary pathogenesis of this lesion?
Explanation
Question 55
A 15-year-old boy completes a standard course of neoadjuvant multidrug chemotherapy (MAP: methotrexate, doxorubicin, cisplatin) for high-grade conventional osteosarcoma of the distal femur. He subsequently undergoes a wide surgical resection. The pathology report notes 95% tumor necrosis in the resected specimen. Which of the following best describes the clinical significance of this finding?
Explanation
Question 56
A 55-year-old man presents with an enlarging, painful mass in his proximal humerus. Radiographs show a lytic lesion with 'ring and arc' calcifications in the metadiaphysis. Biopsy demonstrates a hypercellular cartilaginous matrix with plump, binucleated chondrocytes and permeation into the surrounding lamellar bone. Which of the following gene mutations is most commonly associated with this primary bone tumor?
Explanation
Question 57
A 14-year-old boy presents with progressive knee pain and swelling for 3 months, accompanied by low-grade fevers. Radiographs of the distal femur reveal a permeative destructive lesion in the metadiaphysis with a prominent 'onion skin' periosteal reaction. Biopsy shows sheets of uniform small round blue cells. Immunohistochemistry is strongly positive for CD99. Which of the following chromosomal translocations is most characteristic of this tumor?
Explanation
Question 58
A 32-year-old woman presents with worsening knee pain. Radiographs reveal an eccentric, purely lytic lesion in the distal femur that extends directly to the subchondral bone without a sclerotic margin. Biopsy demonstrates numerous multinucleated giant cells in a background of mononuclear stromal cells. Due to the proximity of the lesion to the joint surface and its size, she is treated with a targeted monoclonal antibody to downstage the tumor prior to surgery. What is the precise mechanism of action of this medication?
Explanation
Question 59
A 19-year-old man complains of a dull, aching pain in his right thigh that consistently worsens at night but is profoundly relieved by ibuprofen. CT imaging reveals a 0.8-cm radiolucent nidus surrounded by dense reactive cortical sclerosis in the femoral diaphysis. If a surgical resection is performed, histological analysis of the central nidus would most likely reveal which of the following?
Explanation
Question 60
A 28-year-old woman presents with a slow-growing, painful mass near her right knee that has been present for over two years. Radiographs show a soft-tissue mass with stippled calcifications. An MRI demonstrates a heterogeneous soft-tissue mass adjacent to, but distinct from, the joint space. A biopsy reveals a biphasic pattern consisting of epithelial-like glandular structures and a spindle cell stromal component. Which of the following genetic abnormalities is most specifically associated with this tumor?
Explanation
Question 61
A 60-year-old man presents with chronic low back pain and a recent onset of bowel and bladder dysfunction. MRI of the sacrum reveals a midline destructive lesion with a large pre-sacral soft-tissue component, displaying high signal intensity on T2-weighted images. A core needle biopsy reveals lobules of cells with abundant, bubbly, vacuolated cytoplasm arranged in cords. Immunohistochemistry for which of the following markers is most specific to confirm the diagnosis of this neoplasm?
Explanation
Question 62
During fracture healing, a complex molecular cascade dictates the differentiation of multipotent mesenchymal stem cells into the specific cell lineages necessary for bone repair. Which of the following transcription factors serves as the critical 'master regulator' for committing mesenchymal stem cells to the osteoblastic lineage?
Explanation
Question 63
A 65-year-old woman is being evaluated for generalized bone pain, profound fatigue, and recent onset of hypercalcemia. Laboratory studies confirm a normocytic anemia, elevated serum creatinine, and a monoclonal spike on serum protein electrophoresis. Plain radiographs show multiple sharply marginated 'punched-out' lytic lesions in her skull and pelvis. If a technetium-99m bone scan is performed, which of the following findings is most likely?
Explanation
Question 64
A 70-year-old woman with a history of postmenopausal osteoporosis sustains a fragility fracture of her distal radius. She has been on oral alendronate therapy for the past three years. Nitrogen-containing bisphosphonates, such as alendronate, inhibit osteoclast-mediated bone resorption primarily through which of the following molecular mechanisms?
Explanation
Question 65
A 12-year-old boy presents with multiple palpable, painless, bony prominences around his knees, ankles, and shoulders. Radiographs confirm multiple pedunculated and sessile bony outgrowths projecting away from the adjacent joints in the metaphyses of the long bones, continuous with the medullary cavity of the native bone. He is diagnosed with Multiple Hereditary Exostoses (MHE). What is the primary underlying biochemical defect associated with the genetic mutations in this disorder?
Explanation
Question 66
What is the most significant prognostic factor for overall survival in a patient with localized, high-grade intramedullary osteosarcoma of the distal femur following neoadjuvant chemotherapy and surgical resection?
Explanation
Question 67
A 25-year-old male presents with a slowly growing, painful mass deep in the thigh. MRI shows a well-circumscribed heterogeneous soft tissue mass adjacent to the femur but not invading the bone. Biopsy reveals a biphasic tumor with both epithelial and spindle cell components. Which of the following genetic translocations is most characteristic of this lesion?
Explanation
Question 68
A 30-year-old female presents with knee pain. Radiographs reveal an eccentric, purely lytic lesion in the distal femur extending to the subchondral bone. Biopsy confirms a giant cell tumor of bone. Denosumab is considered for medical management to facilitate surgery. What is the primary cellular target of this medication?
Explanation
Question 69
A 60-year-old man presents with progressive, deep aching pain in his right pelvis. Radiographs show a destructive lytic lesion with 'ring and arc' calcifications in the ilium. Biopsy reveals a grade II chondrosarcoma. What is the most appropriate definitive management?
Explanation
Question 70
A 12-year-old boy presents with pain and swelling in the midshaft of his tibia. Radiographs demonstrate a permeative, diaphyseal lytic lesion with an 'onion skin' periosteal reaction. Histopathology reveals sheets of small round blue cells. Immunohistochemistry is strongly positive for CD99. What is the most appropriate initial treatment sequence?
Explanation
Question 71
A 15-year-old boy reports severe, throbbing right thigh pain that is worse at night and completely relieved by ibuprofen. A CT scan shows a 7-mm radiolucent nidus surrounded by dense sclerotic bone in the femoral diaphysis. What is the primary mediator responsible for the severe pain associated with this lesion?
Explanation
Question 72
A 22-year-old male with known multiple hereditary exostoses (MHE) presents with a rapidly enlarging, painful mass over the posterior aspect of his distal femur. An MRI shows an osteochondroma with a cartilage cap thickness of 2.5 cm. Which of the following gene mutations is most strongly associated with his underlying condition?
Explanation
Question 73
A 16-year-old female presents with mild knee pain. Radiographs reveal an expansile, eccentric lytic lesion in the proximal tibial metaphysis. MRI demonstrates multiple fluid-fluid levels within the lesion. Biopsy shows blood-filled spaces lacking an endothelial lining. Which genetic rearrangement is considered the primary driver of this lesion?
Explanation
Question 74
An 8-year-old boy sustains a pathologic fracture of the proximal humerus after a minor fall. Radiographs show a centrally located, completely lytic lesion in the metadiaphysis with a 'fallen leaf' sign. What is the most appropriate initial management for this presentation?
Explanation
Question 75
Which of the following bone morphogenetic proteins (BMPs) is FDA-approved specifically for use in acute, open tibial shaft fractures treated with an intramedullary nail?
Explanation
Question 76
A 25-year-old man presents with a slowly enlarging, painless mass on the posterior aspect of his distal thigh. Radiographs demonstrate a dense, heavily ossified mass attached to the posterior cortex of the distal femur with a broad base, and a subtle radiolucent line separating a portion of the tumor from the underlying bone (a 'string sign'). Biopsy reveals a spindle cell proliferation with low-grade atypia and well-formed bone trabeculae. Which of the following is the most characteristic genetic alteration associated with this patient's condition?

Explanation
Question 77
A 35-year-old woman presents with persistent knee pain. Radiographs reveal an eccentric, purely lytic lesion in the proximal tibial epiphysis that extends to the subchondral bone. A core needle biopsy demonstrates a proliferation of mononuclear stromal cells interspersed with numerous multinucleated giant cells. For cases of this disease that are deemed unresectable or recurrent, medical therapy is often employed. What is the primary mechanism of action of the most commonly used targeted biologic agent for this condition?
Explanation
Question 78
A 14-year-old boy presents with progressive thigh pain, low-grade fevers, and an elevated erythrocyte sedimentation rate. Radiographs show a permeative diaphyseal lesion in the femur with a multi-layered, 'onion skin' periosteal reaction. Histologic examination of a biopsy specimen reveals sheets of uniform, small, round blue cells that strongly express CD99 on immunohistochemistry. The most common chromosomal translocation associated with this diagnosis results in which of the following fusion genes?

Explanation
Question 79
A 55-year-old man complains of worsening right shoulder pain over several months. Radiographs show a 6-cm radiolucent lesion in the proximal humerus with intralesional stippled 'rings and arcs' calcifications and endosteal scalloping involving 80% of the cortical thickness. Biopsy confirms a conventional Grade II chondrosarcoma. What is the most appropriate definitive management for this patient?
Explanation
Question 80
A 16-year-old girl is evaluated for rapid onset of pain and swelling over the distal fibula. Radiographs show an eccentric, expansile, lytic lesion with cortical thinning. An MRI reveals multiple cysts with fluid-fluid levels. Core biopsy is consistent with an aneurysmal bone cyst (ABC). Primary aneurysmal bone cysts are distinct neoplastic entities frequently characterized by a translocation involving which of the following genes?
Explanation
Question 81
A 65-year-old man presents to the clinic with severe, unrelenting mid-back pain and progressive fatigue. Laboratory studies reveal hypercalcemia and a normocytic anemia. Plain radiographs demonstrate multiple sharply demarcated, 'punched-out' lytic lesions throughout the calvarium and thoracolumbar spine. Which of the following diagnostic findings is most specific for confirming the primary underlying etiology?
Explanation
Question 82
An 8-year-old boy presents with localized severe back pain. Plain radiographs of the thoracic spine reveal complete collapse of the T8 vertebral body (vertebra plana) with relative preservation of the adjacent intervertebral disc spaces. If a biopsy of the lesion were performed, immunohistochemical staining would most likely be positive for which of the following pairs of markers?
Explanation
Question 83
A 25-year-old woman is evaluated for a limp and dull aching pain in her right hip. She has a history of precocious puberty and notes multiple hyperpigmented macules with irregular borders on her torso. Radiographs of the proximal right femur show an expansile, medullary, ground-glass lesion with a 'shepherd's crook' deformity. The underlying genetic mutation responsible for this patient's condition results in which of the following cellular derangements?
Explanation
Question 84
A 30-year-old man notes a slowly growing, deeply seated, painful mass on the plantar aspect of his foot that he first noticed over a year ago. MRI reveals a 4-cm soft-tissue mass with multi-lobular, heterogeneous signal adjacent to the plantar fascia. Biopsy reveals a biphasic tumor consisting of both epithelial-like gland structures and a spindle cell stroma. Which of the following cytogenetic abnormalities is pathognomonic for this tumor?
Explanation
Question 85
An 18-year-old man complains of persistent mid-back pain that is worse at night. He reports that the pain is only partially relieved by ibuprofen. A CT scan of the thoracic spine demonstrates a well-circumscribed, 2.8-cm radiolucent nidus in the posterior elements of T12, surrounded by moderate reactive sclerosis. Based on the size and clinical characteristics of the lesion, what is the most likely diagnosis?
Explanation
Question 86
A 15-year-old boy presents with a painful, enlarging mass about the right knee. Imaging reveals a mixed lytic and sclerotic lesion in the distal femoral metaphysis with an aggressive periosteal reaction. Biopsy confirms high-grade intramedullary osteosarcoma. Which of the following genetic alterations is most frequently associated with the pathogenesis of this disease?
Explanation
Question 87
A 32-year-old woman presents with a lytic, eccentrically located lesion in the distal radius extending into the subchondral bone. Biopsy demonstrates mononuclear cells intermixed with numerous large, multinucleated osteoclast-like giant cells. The patient is prescribed a targeted medical therapy for her condition. Which of the following best describes the mechanism of action of this drug?
Explanation
Question 88
A 12-year-old boy presents with fever, weight loss, and a painful mass in the diaphysis of the left femur. Radiographs show a permeative lytic lesion with an 'onion-skin' periosteal reaction. A biopsy is performed. Which of the following immunohistochemical markers or genetic findings is most specific to confirm the likely diagnosis?
Explanation
Question 89
A 55-year-old man undergoes curettage and bone grafting for an expansile lytic lesion in the proximal phalanx of his ring finger, which has been growing slowly. Histology shows a well-circumscribed cartilaginous tumor with mild cellular atypia. This tumor is most commonly associated with somatic mutations in which of the following genes?
Explanation
Question 90
A 20-year-old man presents with deep, aching night pain in his thigh that is dramatically relieved by oral ibuprofen. Radiographs reveal a small radiolucent nidus (<1.5 cm) surrounded by dense reactive sclerosis in the femoral diaphysis. The profound pain relief provided by NSAIDs is primarily due to the lesion's high local production of:
Explanation
Question 91
A 14-year-old girl sustains a minor fall and reports persistent shoulder pain. Radiographs of the proximal humerus show a central, purely lytic lesion with cortical thinning. A 'fallen leaf' sign is noted. A needle is advanced into the lesion for aspiration and injection. What type of fluid is typically aspirated from this cyst?
Explanation
Question 92
A 60-year-old man presents with persistent sacral pain, recent-onset bowel and bladder dysfunction, and a palpable pre-sacral soft-tissue mass. Imaging demonstrates a destructive, midline sacral lesion with a large anterior soft tissue component. Histopathologic examination of the biopsy reveals lobules of vacuolated cells with bubbly cytoplasm set in a myxoid stroma. Which of the following immunohistochemical markers is most highly specific for this tumor?
Explanation
Question 93
A 45-year-old woman is evaluated for a slowly enlarging, painless mass in the deep posterior compartment of her thigh. MRI reveals a well-circumscribed, lobulated mass with heterogeneous high T2 signal and a 'triple signal' pattern. Biopsy shows a biphasic tumor containing both epithelial (glandular) and spindle cell components. Which of the following cytogenetic abnormalities is diagnostic for this tumor?
Explanation
Question 94
A 65-year-old man is incidentally found to have a substantially elevated serum alkaline phosphatase level on routine laboratory work. His serum calcium, phosphorus, and parathyroid hormone levels are strictly normal. Radiographs of his pelvis show thickened trabeculae, cortical thickening, and overall bone enlargement. A defect in which of the following cell types is considered the primary initiating event in the pathogenesis of this condition?
Explanation
Question 95
A 68-year-old man presents with severe generalized lower back pain, persistent fatigue, and recurrent respiratory infections. Laboratory testing reveals normocytic anemia, hypercalcemia, and an elevated serum creatinine. Radiographs of the spine and skull demonstrate multiple 'punched-out' lytic lesions lacking reactive sclerotic margins. A bone marrow aspirate and biopsy are most likely to show an abnormal, clonal proliferation of which of the following cell types?
Explanation
Question 96
A 15-year-old boy presents with knee pain and a mixed lytic/sclerotic lesion in the metaphysis of the distal femur. Biopsy confirms high-grade osteosarcoma. Which of the following genetic alterations is most strongly associated with the pathogenesis of this disease?
Explanation
Question 97
A 32-year-old woman presents with progressive pain and swelling in her left knee. Radiographs reveal an eccentric, completely lytic lesion in the proximal tibia extending to the subchondral bone without a sclerotic margin. Biopsy shows multinucleated giant cells in a background of mononuclear stromal cells. If targeted pharmacological therapy is considered to reduce tumor burden, what is the mechanism of action of the most appropriate agent?
Explanation
Question 98
A 10-year-old boy presents with fever, weight loss, and mid-thigh pain. Imaging shows a permeative, diaphyseal lesion with an 'onion-skin' periosteal reaction. Histology reveals sheets of small, round blue cells that stain strongly positive for CD99. What represents the most significant prognostic factor for overall survival in this patient?
Explanation
Question 99
A 24-year-old man sustains a pathological fracture of the proximal femur. Radiographs prior to the fracture revealed a well-circumscribed, intramedullary lesion with a 'ground-glass' appearance and a 'shepherd's crook' deformity. A biopsy demonstrates irregular trabeculae of woven bone without prominent osteoblastic rimming in a fibrous stroma. Which of the following best describes the underlying molecular pathogenesis of this condition?
Explanation
Question 100
A 19-year-old male complains of severe, right-sided thigh pain that worsens at night and is characteristically relieved by ibuprofen within 30 minutes. Plain radiographs of the femur show a 1-cm radiolucent nidus surrounded by dense reactive sclerosis in the diaphyseal cortex. Which of the following is most accurate regarding the pathophysiology and characteristics of this lesion?
Explanation
None
