Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4)

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4). Top-rated Orthopedic Sports Medicine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
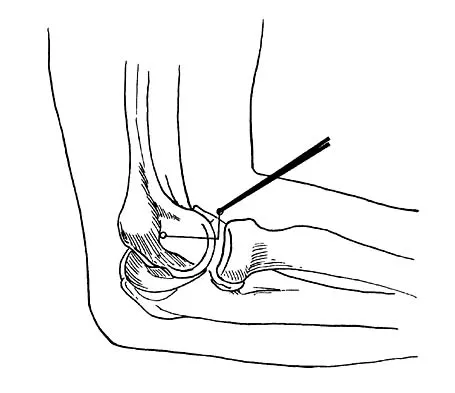
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
Question 2
A 39-year-old man has anterior shoulder pain after landing on his abducted left shoulder while playing softball. Examination reveals a stable glenohumeral joint, pain on passive external rotation of greater than 25 degrees, and pain and weakness on belly press (Napoleon's) test. An MRI scan is shown in Figure 32. To provide maximum pain relief and return of function, management should include
Explanation
Question 3
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Explanation
Question 4
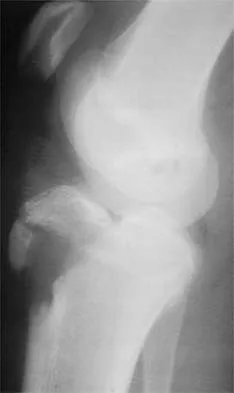
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
Explanation
Question 5
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
Question 6
Which of the following best describes athletic pubalgia?
Explanation
Question 7
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of
Explanation
Question 8
Which of the following activities can improve posterior capsular contractures?
Explanation
Question 9
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
Question 10
Following reconstruction of the anterior cruciate ligament (ACL), which of the following rehabilitation exercises has the greatest potential to harm the graft?
Explanation
Question 11
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
Question 12
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
Question 13
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
Question 14
Figure 36 shows the radiograph of a 28-year-old man who injured his shoulder in a motocross race. Management should consist of
Explanation
Question 15
Figure 37 shows the radiograph of a 21-year-old collegiate basketball player who has had mild midfoot aching for the past 4 months. What is the best course of action?
Explanation
Question 16
A 17-year-old high school gymnast who has peripatellar knee pain has been unable to practice on a consistent basis for the past 3 years. She denies any specific injury events. Physical therapy for modalities, quadriceps strengthening, and hamstring stretching provide temporary relief. A trial of patellar taping significantly reduces her pain. Examination reveals an 15-degree Q angle, moderate lateral facet tenderness, negative patellar apprehension, and the inability to evert the patella. Radiographs show a moderate lateral patellar tilt. Treatment should now consist of
Explanation
Question 17
An active 55-year-old man who felt a sudden pop in the left heel while playing tennis 6 months ago was diagnosed with an ankle sprain around the time of injury. He now reports calf atrophy and severe weakness with running. Examination reveals a palpable defect in the Achilles tendon and only trace passive ankle flexion when the calf is squeezed. At the time of surgery, an Achilles tendon defect of 6 cm cannot be approximated. Surgical management of the Achilles tendon should include
Explanation
Question 18
Figures 38a and 38b show the AP and lateral radiographs of a 12-year-old baseball pitcher who has pain in his right dominant elbow. Management should consist of
Explanation
Question 19
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
Question 20
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
Question 21
A 20-year-old college baseball pitcher reports the insidious onset of medial elbow pain. Examination reveals medial elbow tenderness, a normal neurologic examination, and no obvious valgus laxity. Plain radiographs are normal. MRI scans are shown in Figures 39a and 39b. Management should consist of
Explanation
Question 22
What is the most common arthroscopic finding of internal impingement in an overhead athlete?
Explanation
Question 23
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
Question 24
The essential lesion responsible for posterolateral rotatory instability of the elbow is disruption of the
Explanation
Question 25
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Explanation
Question 26
A 19-year-old female presents with recurrent patellar dislocations. Imaging shows a tibial tubercle-trochlear groove (TT-TG) distance of 14 mm and a normal Insall-Salvati ratio. An isolated medial patellofemoral ligament (MPFL) reconstruction is planned.
What is the primary biomechanical consequence of placing the femoral tunnel for the MPFL graft significantly proximal to Schöttle's point?

Explanation
Question 27
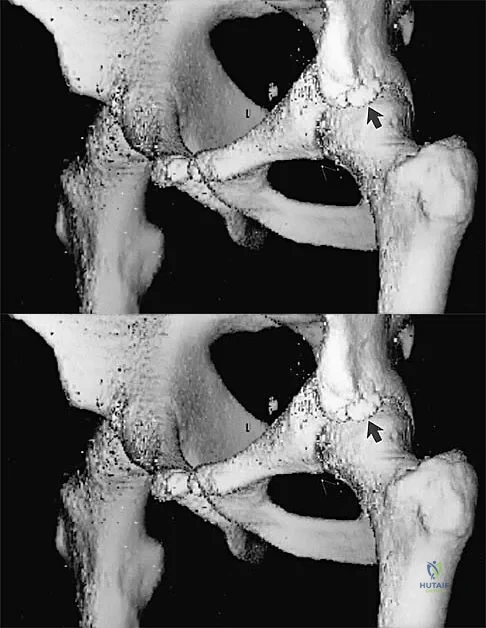
A 28-year-old hockey player undergoes hip arthroscopy for a symptomatic CAM-type femoroacetabular impingement and a focal anterosuperior labral tear. The anterolateral (AL) portal is established first under fluoroscopic guidance. To safely establish the mid-anterior (MAP) portal, the surgeon must remain lateral to the sagittal plane of the anterior superior iliac spine (ASIS). Deviating medial to this plane primarily increases the risk of injury to which of the following structures?
Explanation
Question 28
A 21-year-old male football player undergoes primary ACL reconstruction with a bone-patellar tendon-bone autograft. Two years later, he presents with an atraumatic graft rupture. Standing lateral radiographs demonstrate a posterior tibial slope (PTS) of 16 degrees. If a revision ACL reconstruction is performed without addressing the bony anatomy, what biomechanical alteration is most responsible for an increased risk of early graft failure?
Explanation
Question 29
A 62-year-old laborer presents with chronic, debilitating shoulder pain and pseudoparalysis. MRI reveals a massive, retracted, irreparable tear of the supraspinatus and infraspinatus with Grade 4 fatty infiltration. The subscapularis and teres minor are intact. He undergoes an arthroscopic superior capsular reconstruction (SCR) using a thick dermal allograft.
Biomechanically, how does the SCR primarily restore shoulder kinematics in this specific clinical scenario?

Explanation
Question 30
A 22-year-old collegiate baseball pitcher presents with posteromedial elbow pain and a noticeable decrease in throwing velocity over the last two months. He describes a severe 'catching' and 'locking' sensation specifically in the deceleration phase of throwing. Physical examination reveals a 15-degree flexion contracture and sharp pain in the posteromedial olecranon fossa when forced terminal extension is applied concurrently with a valgus stress. The milking maneuver is negative. What is the most likely diagnosis?
Explanation
Question 31
A 55-year-old female presents with acute medial knee pain following a squatting maneuver. MRI reveals a complete radial tear directly adjacent to the posterior root attachment of the medial meniscus, with associated meniscal extrusion of 4 mm.
Which of the following best describes the biomechanical consequence of leaving this specific root injury unaddressed?

Explanation
Question 32
A 24-year-old rugby player presents for management of recurrent anterior shoulder instability. He has had four dislocations. Computed tomography (CT) with 3D sagittal reconstruction demonstrates an anteroinferior glenoid bone loss of 22% and a large, engaging Hill-Sachs lesion. Based on current literature and evidence-based treatment algorithms, which of the following is the most appropriate surgical management?
Explanation
Question 33
A 14-year-old male gymnast with open physes presents with chronic right knee pain. MRI reveals a 2 x 2 cm osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle.
The articular cartilage is intact, and there is no high T2 signal fluid behind the fragment, indicating a stable lesion. He has failed 6 months of strict non-operative management including restricted weight-bearing. What is the most appropriate next step in management?

Explanation
Question 34
During an open subpectoral biceps tenodesis, the surgeon creates a cortical window in the bicipital groove just distal to the transverse humeral ligament. However, due to extensive fraying of the long head of the biceps tendon, the incision and deep dissection are extended further distally along the humeral shaft. If medial retractors are placed too aggressively deep to the conjoined tendon and biceps muscle belly during this distal extension, which neurovascular structure is at greatest risk of iatrogenic injury?
Explanation
Question 35
A 26-year-old man sustains a dashboard injury resulting in an isolated posterior cruciate ligament (PCL) tear. Following failure of non-operative management, a single-bundle PCL reconstruction is planned. To accurately reproduce the biomechanics of the primary restraint to posterior tibial translation at 90 degrees of flexion, the graft should be placed to reconstruct which specific bundle, and where is its native femoral footprint located?
Explanation
Question 36
During an anatomic single-bundle anterior cruciate ligament (ACL) reconstruction, the femoral tunnel is drilled through the accessory anteromedial portal. Compared to traditional drilling through a transtibial portal, what is the primary biomechanical advantage of this technique?
Explanation
Question 37
A 25-year-old male sustains a multiligament knee injury. Examination reveals a grade 3 posterior sag and grade 3 varus opening in full extension and at 30 degrees of flexion. The dial test shows increased external rotation at 30 degrees but is symmetric at 90 degrees. He is planned for PCL and posterolateral corner (PLC) reconstruction.
What anatomic structure of the PLC is the primary restraint to varus gapping at 30 degrees of knee flexion?
Explanation
Question 38
A 65-year-old male presents with pseudoparalysis of the shoulder. An MRI reveals an irreparable, chronically retracted tear of the subscapularis tendon with significant fatty infiltration (Goutallier stage 4). The posterosuperior cuff is intact. He is scheduled to undergo a pectoralis major transfer. Which portion of the pectoralis major is typically transferred to best replicate the force vector of the native subscapularis?
Explanation
Question 39
A 28-year-old professional hockey player presents with chronic anterior groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a pistol-grip deformity of the proximal femur.
Which of the following radiographic parameters is most diagnostic of a Cam-type femoroacetabular impingement (FAI)?
Explanation
Question 40
A 14-year-old female gymnast presents with progressive lateral elbow pain and mechanical catching. Imaging reveals an unstable 1.5 cm osteochondral defect (OCD) of the capitellum with loose bodies in the joint. The lateral radiocapitellar ligament is intact. Which surgical treatment provides the best long-term outcome and highest rate of return to sport for an unstable defect of this size in a high-demand athlete?
Explanation
Question 41
A 50-year-old female experiences a sudden "pop" in the posterior aspect of her knee while descending stairs. She is diagnosed with a complete medial meniscus posterior root tear with 3 mm of extrusion on MRI. Biomechanically, what is the direct consequence of leaving this tear untreated compared to the native knee?
Explanation
Question 42
A 45-year-old recreational weightlifter presents with deep anterior shoulder pain. An MRI arthrogram demonstrates a Type II SLAP tear without rotator cuff pathology. A trial of physical therapy and injections has failed to provide relief. What is the most appropriate surgical management for this patient to minimize postoperative stiffness and maximize return to pre-injury activity?
Explanation
Question 43
A 19-year-old female is undergoing a medial patellofemoral ligament (MPFL) reconstruction for recurrent lateral patellar instability. Correct placement of the femoral tunnel is essential to avoid over-constraining the joint. Which of the following landmarks accurately describes the anatomic femoral footprint of the native MPFL?
Explanation
Question 44
A 25-year-old male cyclist falls directly onto his right shoulder. Clinical examination reveals a prominent clavicle, and radiographs confirm a 120% superior displacement of the distal clavicle relative to the acromion, with an increased coracoclavicular distance. He is diagnosed with a Type III acromioclavicular (AC) joint separation. According to current evidence, what is the recommended initial management for this injury in a non-laboring individual?
Explanation
Question 45
A 32-year-old male suffers an acute Achilles tendon rupture while playing basketball. He elects to pursue nonoperative management. Compared to traditional prolonged cast immobilization, what is the primary advantage of employing an early functional rehabilitation protocol (early weight-bearing in an orthosis with functional ROM)?
Explanation
Question 46
A 50-year-old female presents with acute-onset medial joint line pain and an effusion after squatting deeply. An MRI shows an extrusion of the medial meniscus on coronal views and an 'empty meniscus' or 'ghost sign' on a single sagittal cut. Figure 1
illustrates a similar pathology. Biomechanically, what is the direct consequence of this specific injury pattern if left untreated?
Explanation
Question 47
A 28-year-old professional hockey player undergoes hip arthroscopy for femoroacetabular impingement (FAI). The surgeon establishes an anterolateral portal, followed by an anterior portal. Which of the following describes the typical sensory deficit expected if the nerve most at risk during the placement of the anterior portal is iatrogenically injured?
Explanation
Question 48
A 22-year-old collegiate baseball pitcher reports severe medial elbow pain and a recent drop in his fast pitch velocity. He experiences sharp pain during the late cocking and early acceleration phases of throwing. The moving valgus stress test is markedly positive. An MRI arthrogram demonstrates a high-grade partial tear of the ulnar collateral ligament (UCL). If conservative management fails and surgical reconstruction is planned, which anatomic bundle of the UCL must be targeted as it is the primary restraint to valgus stress at 90 degrees of flexion?
Explanation
Question 49
A 32-year-old competitive weightlifter feels a sudden tearing sensation and 'pop' in his anterior axilla while performing a one-rep max bench press. Physical examination reveals an asymmetrical loss of the anterior axillary fold, significant ecchymosis, and weakness in internal rotation and adduction. An MRI confirms a complete rupture of the pectoralis major tendon. During an open surgical repair, the surgeon must accurately reattach the tendon to its anatomic footprint. Which of the following accurately describes the insertion of the sternal head of the pectoralis major relative to the clavicular head?
Explanation
Question 50
A 24-year-old rugby player sustains a blow to the anteromedial aspect of his fully extended right knee. He complains of posterolateral knee pain, giving way, and difficulty descending stairs. On examination, the dial test reveals 20 degrees of increased external rotation compared to the contralateral normal knee at 30 degrees of flexion, but symmetrical external rotation at 90 degrees of flexion. Based on these physical examination findings, which of the following injury patterns is most likely present?
Explanation
Question 51
A 26-year-old professional baseball pitcher presents with a dull, aching posterior shoulder pain. Examination reveals 20 degrees of internal rotation and 130 degrees of external rotation of the dominant shoulder at 90 degrees of abduction. The contralateral shoulder has 60 degrees of internal rotation and 100 degrees of external rotation. Radiographs are unremarkable. What is the primary underlying anatomic pathology associated with this athlete's Glenohumeral Internal Rotation Deficit (GIRD)?
Explanation
Question 52
A 14-year-old male cross-country runner presents with vague, intermittent anterior knee pain and mechanical catching for the past 3 months. Radiographs demonstrate an osteochondral lesion of the lateral aspect of the medial femoral condyle. He has widely open distal femoral physes. Figure 7
demonstrates the MRI findings, which reveal a 1.5 cm by 1.5 cm lesion with intact overlying cartilage and no high T2 fluid signal behind the fragment. What is the most appropriate initial management?
Explanation
Question 53
A 28-year-old cyclist sustains a severe type V acromioclavicular (AC) joint separation after being thrown over the handlebars. He fails conservative management and undergoes an anatomic coracoclavicular (CC) ligament reconstruction. To accurately recreate the biomechanics of the native ligaments, the surgeon must drill the clavicular tunnels mimicking the anatomic footprints. Which of the following accurately describes the anatomic orientation of the conoid and trapezoid ligaments?
Explanation
Question 54
A 16-year-old female gymnast presents with a history of recurrent lateral patellar dislocations. She is indicated for a medial patellofemoral ligament (MPFL) reconstruction. To ensure proper isometry of the graft, the femoral tunnel must be placed at 'Schöttle/'s point'. Which of the following best describes the anatomic location of the MPFL origin on the femur?
Explanation
Question 55
A 23-year-old male underwent an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft 6 months ago. He has aggressively participated in physical therapy but continues to complain of a painful mechanical block to terminal extension, lacking 10 degrees compared to the uninjured side. Figure 11
displays a sagittal MRI of his knee. What is the most likely diagnosis?

Explanation
Question 56
A 22-year-old soccer player sustains a twisting knee injury. Radiographs demonstrate a small avulsion fracture of the lateral tibial plateau just distal to the articular surface (Segond fracture). Biomechanical studies demonstrate that the structure avulsed in this injury pattern primarily resists which of the following forces?
Explanation
Question 57
During an open subpectoral biceps tenodesis, the conjoint tendon is retracted medially to optimize exposure of the bicipital groove and pectoralis major tendon. Overzealous medial retraction of the conjoint tendon is most likely to result in injury to which of the following nerves?
Explanation
Question 58
A 26-year-old male with symptomatic cam-type femoroacetabular impingement undergoes hip arthroscopy with osteochondroplasty. During resection of the cam lesion on the femoral neck, aggressive resection of the posterolateral aspect is avoided to prevent injury to the retinacular vessels. These critical vessels are terminal branches of which artery?
Explanation
Question 59
A 52-year-old female undergoes an MRI of the knee for posterior knee pain after a deep squat. The MRI demonstrates a complete radial tear at the posterior root attachment of the medial meniscus. If left untreated, this specific injury pattern alters the joint biomechanics most similarly to which of the following scenarios?
Explanation
Question 60
During a classic Latarjet procedure for anterior shoulder instability with significant glenoid bone loss, the coracoid process is transferred to the anterior glenoid rim. To expose the anterior glenoid, how is the subscapularis muscle typically managed in the traditional Latarjet technique described by Walch?
Explanation
Question 61
A 20-year-old collegiate pitcher undergoes a flexor-pronator splitting approach for ulnar collateral ligament (UCL) reconstruction. During the initial subcutaneous dissection over the medial epicondyle, a nerve is encountered and carefully protected. Injury to this nerve would result in a sensory deficit to which of the following areas?
Explanation
Question 62
A 16-year-old gymnast requires medial patellofemoral ligament (MPFL) reconstruction for recurrent instability. Intraoperative fluoroscopy is used to identify Schöttle's point for the femoral tunnel.
Which of the following describes the correct fluoroscopic location of this point on a strictly lateral radiograph?
Explanation
Question 63
A 62-year-old man presents with a chronic, massive, irreparable posterosuperior rotator cuff tear. He has active forward elevation to 130 degrees but severe pain. He is considered for an arthroscopic Superior Capsular Reconstruction (SCR). Which of the following is considered an absolute contraindication for this procedure?
Explanation
Question 64
A 13-year-old male presents with vague anterior knee pain and occasional catching. Radiographs reveal a lesion consistent with osteochondritis dissecans (OCD) in the most classic location within the knee. Which of the following best describes this anatomical location?
Explanation
Question 65
A 35-year-old male sustains an acute Achilles tendon rupture playing basketball. He elects for non-operative management. According to recent randomized controlled trials and AAOS clinical practice guidelines, which of the following protocols provides rerupture rates most comparable to operative repair?
Explanation
Question 66
A 22-year-old collegiate soccer player sustains a twisting knee injury. MRI demonstrates a complete anterior cruciate ligament (ACL) tear and a medial meniscus posterior root tear.
Biomechanically, an unrepaired medial meniscus posterior root tear alters knee joint kinematics in a manner most similar to which of the following?

Explanation
Question 67
A 24-year-old rugby player presents with recurrent anterior shoulder instability. A CT scan of the shoulder reveals 12% anterior glenoid bone loss and a large Hill-Sachs lesion. Applying the glenoid track concept, the Hill-Sachs lesion is calculated to be 'off-track.' Which of the following is the most appropriate surgical management to minimize the risk of recurrent instability?
Explanation
Question 68
A 20-year-old collegiate baseball pitcher undergoes ulnar collateral ligament (UCL) reconstruction using the modified Jobe (figure-of-8) technique.
Compared to the docking technique, the modified Jobe technique is associated with a higher incidence of which of the following postoperative complications?
Explanation
Question 69
A 28-year-old athlete presents with a hyperextension injury to the knee. On physical examination, the dial test is performed. There is 15 degrees of increased external rotation of the tibia relative to the uninjured contralateral side at 30 degrees of knee flexion. At 90 degrees of knee flexion, the external rotation is symmetric bilaterally. Which structure is most likely injured?
Explanation
Question 70
During hip arthroscopy for femoroacetabular impingement (FAI), standard portals are established. The anterior portal is typically made under direct visualization. Which of the following neurological structures is at greatest risk of iatrogenic injury during the establishment of the anterior portal?
Explanation
Question 71
A 19-year-old female undergoes medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability.
To avoid non-anatomic graft placement that could result in excessive tension during knee flexion, the surgeon identifies the femoral footprint utilizing Schöttle's point. Anatomically, this footprint is located in relation to which of the following osseous landmarks?
Explanation
Question 72
A 21-year-old hockey player sustains a forceful external rotation injury to his right ankle. Examination reveals point tenderness over the anterior inferior tibiofibular ligament (AITFL). Radiographs reveal no fractures. The external rotation stress test elicits pain, but fluoroscopic stress views demonstrate no widening of the medial clear space or tibiofibular overlap. MRI confirms an isolated full-thickness tear of the AITFL; the deltoid and posterior inferior tibiofibular ligaments are intact. What is the most appropriate management?
Explanation
Question 73
A 45-year-old male presents with acute knee pain and inability to actively extend his knee after a fall while playing basketball.
A lateral radiograph of the knee reveals a significantly low-riding patella (patella baja) compared to the contralateral knee. Which of the following is the most likely diagnosis?

Explanation
Question 74
A 42-year-old recreational weightlifter presents with deep shoulder pain exacerbated by overhead activities. Physical therapy has failed after 6 months. An MRI arthrogram reveals an isolated Type II superior labrum anterior-posterior (SLAP) tear. Given the patient's age and activity profile, which surgical intervention is statistically associated with the highest rate of return to sport and the lowest rate of revision surgery?
Explanation
Question 75
An 18-year-old athlete undergoes an isolated arthroscopic all-inside repair of a vertical longitudinal tear located in the red-white zone of the medial meniscus. To maximize the biological healing potential of this isolated meniscal repair, which of the following intraoperative adjuncts is most strongly supported by current literature?
Explanation
Question 76
A 35-year-old male weightlifter presents with chronic anterior shoulder pain that radiates down his arm. He reports pain primarily during the bench press and cross-body adduction. Physical examination reveals point tenderness over the coracoid process, and a positive O'Brien test that is relieved by external rotation. MRI of the shoulder reveals a coracohumeral distance of 4 mm and subscapularis tendinosis without a rotator cuff tear. After failing 6 months of physical therapy and corticosteroid injections, what is the most appropriate surgical management?
Explanation
Question 77
A 22-year-old collegiate football player presents with a recurrent anterior cruciate ligament (ACL) tear after sustaining a contact injury. His primary ACL reconstruction was performed 3 years ago utilizing a bone-patellar tendon-bone (BTB) autograft. Preoperative computed tomography (CT) demonstrates a femoral tunnel diameter of 16 mm and a tibial tunnel diameter of 15 mm. What is the most appropriate next step in surgical management?
Explanation
Question 78
A 45-year-old female presents with sudden onset posteromedial knee pain and a palpable 'pop' while squatting. MRI demonstrates a medial meniscus posterior root tear with 4 mm of meniscal extrusion. Biomechanically, a medial meniscus posterior root tear alters knee kinematics and contact pressures equivalently to which of the following?
Explanation
Question 79
A 28-year-old offensive lineman complains of recurrent posterior shoulder instability that has failed extensive nonoperative management. Imaging shows a reverse Hill-Sachs lesion involving 25% of the anterior humeral articular surface and an associated posterior labral tear. To prevent engagement and provide the best clinical outcome, what is the most appropriate surgical management?
Explanation
Question 80
During reconstruction of the medial patellofemoral ligament (MPFL) for recurrent patellar instability, the surgeon utilizes the Schöttle point to establish the femoral tunnel. If the femoral tunnel is inadvertently placed too proximal and anterior to this isometric point, what is the most likely biomechanical consequence?
Explanation
Question 81
A 19-year-old collegiate baseball pitcher is undergoing ulnar collateral ligament (UCL) reconstruction utilizing a palmaris longus autograft. Following the procedure, what is the most commonly reported postoperative complication?
Explanation
Question 82
A 25-year-old hockey player is undergoing hip arthroscopy for symptomatic femoroacetabular impingement (FAI) characterized by a prominent cam lesion and an alpha angle of 70 degrees. During the osteochondroplasty, excessive bony resection of the cam lesion at the femoral head-neck junction most significantly increases the risk of which of the following complications?
Explanation
Question 83
A 30-year-old male is evaluated in the clinic following a severe twisting injury to his left knee. Physical examination reveals a positive dial test with 15 degrees of increased external rotation at 30 degrees of flexion compared to the contralateral side. However, at 90 degrees of knee flexion, the external rotation is symmetric bilaterally. Which structure or combination of structures is most likely injured?
Explanation
Question 84
A 62-year-old highly active male presents with chronic pseudoparalysis of his right shoulder. Imaging reveals a massive, retracted, and irreparable supraspinatus and infraspinatus tear. He elects to undergo an arthroscopic superior capsular reconstruction (SCR).
To optimize the biomechanical success of the SCR and effectively centralize the humeral head, the allograft must be securely attached to the superior glenoid and which other structures?
Explanation
Question 85
A 14-year-old male presents with vague knee pain and intermittent mechanical catching. Radiographs reveal a 2 x 2 cm osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI reveals a high T2 signal rim completely surrounding the osteochondral fragment. His physes remain open.
What is the most appropriate management?
Explanation
Question 86
A 25-year-old professional football player sustains a contact injury to his right knee. On physical examination, the dial test reveals 20 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral knee. However, at 90 degrees of knee flexion, the external rotation is symmetric bilaterally. Based on these examination findings, which of the following structures is most likely injured?
Explanation
Question 87
A 30-year-old competitive weightlifter feels a sudden "pop" and tearing sensation in his anterior axilla while performing a heavy bench press. He presents with extensive ecchymosis and loss of the anterior axillary fold. MRI confirms a complete, full-thickness rupture of the pectoralis major tendon at its insertion. Which of the following best describes the anatomic orientation of the pectoralis major tendon at its insertion onto the humerus?
Explanation
Question 88
A 19-year-old collegiate wrestler sustains an anterior shoulder dislocation. After successful closed reduction, he complains of numbness over the lateral deltoid and demonstrates weakness with shoulder abduction. Electromyography (EMG) confirms an isolated neurapraxia. What is the expected anatomic distance of the affected nerve from the inferior border of the glenoid at the 6 o'clock position?
Explanation
Question 89
A 22-year-old hockey player presents with chronic groin pain exacerbated by hip flexion and internal rotation. Examination demonstrates a positive anterior impingement test. An anteroposterior pelvis radiograph is obtained.
The radiograph demonstrates a prominent "crossover sign." Measurement of the alpha angle on a Dunn lateral view is 45 degrees. Which of the following is the most likely diagnosis?
Explanation
Question 90
A 20-year-old collegiate baseball pitcher reports progressive medial elbow pain and decreased pitching velocity. Examination reveals pain with the moving valgus stress test and maximal tenderness slightly distal to the medial epicondyle. MRI shows a high-grade partial tear of the ulnar collateral ligament (UCL). Which of the following bundles of the UCL provides the primary restraint to valgus stress at the elbow between 30 and 120 degrees of flexion?
Explanation
Question 91
A 50-year-old female presents with sudden onset medial-sided knee pain and a "pop" while squatting in her garden. She has no mechanical locking but exhibits an antalgic gait. MRI reveals a 4 mm medial meniscal extrusion and a radial defect directly at the posterior root attachment of the medial meniscus. If left untreated, the biomechanical consequence of this specific injury is most equivalent to which of the following?
Explanation
Question 92
A 45-year-old manual laborer presents with chronic, anterior shoulder pain that has failed 6 months of physical therapy and NSAID management. He describes deep, aching pain and catching when lifting objects away from his body. O'Brien's active compression test is positive. MRI reveals an isolated Type II SLAP (Superior Labrum Anterior to Posterior) tear. Given his age and occupational demands, which of the following is the most appropriate surgical management?
Explanation
Question 93
A 40-year-old water skier sustains a hyperflexion injury to the hip with her knee fully extended. She presents with significant ecchymosis over the posterior thigh, an antalgic gait, and an inability to run. MRI confirms a complete, 3-tendon avulsion of the proximal hamstring complex with 4 cm of retraction. Open surgical repair is planned. Which of the following neurovascular structures is located immediately lateral to the ischial tuberosity and is at highest risk during surgical retrieval and repair?
Explanation
Question 94
A 22-year-old female collegiate soccer player presents with localized anterior knee pain and swelling after matches. She has failed 9 months of conservative management. Knee MRI reveals an isolated, full-thickness chondral defect measuring 3.5 cm² on the weight-bearing surface of the medial femoral condyle. Alignment is normal, and there is no meniscal pathology. Which of the following cartilage restoration procedures is most indicated for this patient?
Explanation
Question 95
During diagnostic elbow arthroscopy, the anteromedial portal is frequently established to view the anterior compartment and radiocapitellar joint. Careful creation of this portal is essential to avoid iatrogenic injury. Which of the following nerves is at greatest risk of injury during the placement of the anteromedial portal?
Explanation
Question 96
A 21-year-old male rugby player presents with recurrent anterior shoulder instability. He has had 5 dislocations in the past year. CT scan reveals 25% anterior glenoid bone loss. He undergoes an open Latarjet procedure. Which of the following describes the "sling effect" provided by the Latarjet procedure?
Explanation
Question 97
A 45-year-old woman presents with acute onset medial knee pain after a deep knee flexion maneuver. She felt a "pop" in her knee. MRI demonstrates a medial meniscus posterior root tear and a 2 mm extrusion of the medial meniscus on coronal sequences. Which of the following biomechanical consequences is most likely if this injury is treated nonoperatively?
Explanation
Question 98
A 55-year-old man presents with anterior shoulder pain and weakness following a fall onto an outstretched hand. On physical examination, he demonstrates a positive bear-hug test and increased passive external rotation compared to the contralateral side. MRI confirms an isolated, full-thickness tear of the subscapularis tendon. During arthroscopic repair, which of the following structures must be carefully evaluated and is most commonly associated with this injury pattern?
Explanation
Question 99
A 24-year-old male hockey player presents with groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate an alpha angle of 70 degrees on the Dunn lateral view and a lateral center edge angle of 35 degrees. He is diagnosed with femoroacetabular impingement (FAI). If left untreated, the pathomechanics of his specific impingement type typically result in which of the following patterns of chondral injury?
Explanation
Question 100
A 28-year-old male suffers a high-energy knee injury resulting in a combined posterior cruciate ligament (PCL) and posterolateral corner (PLC) tear. He undergoes a staged reconstruction. During reconstruction of the posterolateral corner, an anatomic fibular-based technique is planned. Which three primary static stabilizing structures of the PLC are reconstructed in this technique?
Explanation
None
