Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 3)

Key Takeaway
We review everything you need to understand about Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 3). Top-rated Orthopedic Sports Medicine 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Sports Medicine 2026 MCQs: Board Review Questions & Answers (Part 3)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
Question 2
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
Question 3
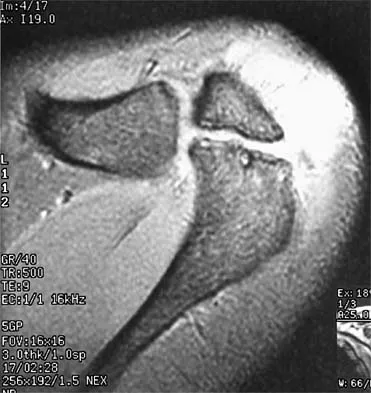
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of
Explanation
Question 4
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
Question 5
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
Question 6
A 37-year-old man has had isolated chronic knee swelling for the past 6 months. He denies any history of specific trauma. Examination reveals a large effusion with a stable knee, but the remainder of the examination is normal. Plain radiographs are unremarkable. An MRI scan reveals a large effusion without meniscal injury. An arthroscopic image of the suprapatellar pouch is shown in Figure 23. What is the most likely diagnosis?
Explanation
Question 7
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Question 8
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
Question 9
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
Question 10
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
Question 11
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
Question 12
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
Explanation
Question 13
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?
Explanation
Question 14
When compared with the normal anterior cruciate ligament (ACL), placement of an anterior cruciate ligament graft in the over-the-top position on the femoral side has what effect on its function?
Explanation
Question 15
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of
Explanation
Question 16
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
Question 17
An 18-year-old football halfback reports that he had immediate right knee pain after being tackled 1 week ago. Examination now reveals moderate tenderness over the proximal medial tibia and lateral joint and normal cruciate stability. In evaluating the integrity of the posterolateral knee structures, what is the most reliable examination finding?
Explanation
Question 18
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
Question 19
A 19-year-old rugby player has severe knee pain after being injured in a game 2 weeks ago. Examination reveals a knee effusion, limited motion, and increased 3+ Lachman's test and anterior drawer. There is also increased external rotation at 30 degrees of knee flexion when the patient is placed in the prone position. Based on these findings, which of the following actions would most likely increase the risk of anterior cruciate ligament (ACL) reconstruction failure?
Explanation
Question 20
The primary function of structure "A" in Figure 29 is to limit
Explanation
Question 21
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in
Explanation
Question 22
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Question 23
Which of the following symptoms are most commonly associated with piriformis syndrome?
Explanation
Question 24
A 19-year-old football player who sustained three traumatic anterior shoulder dislocations underwent surgery to repair a Bankart lesion. Nine months after surgery, examination reveals stability, elevation to 150 degrees, external rotation to 0 degrees with the elbow at his side and to 50 degrees at 90 degrees of abduction, and internal rotation to T12. If his range of motion does not improve, he is at most risk for
Explanation
Question 25
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of
Explanation
Question 26
When performing an anatomic reconstruction of the posterolateral corner (PLC) of the knee, accurate identification of the femoral attachments of the lateral collateral ligament (LCL) and the popliteus tendon is critical for restoring normal kinematics. What is the correct anatomic relationship of the LCL femoral attachment relative to the popliteus tendon attachment?
Explanation
Question 27
A 24-year-old male presents with persistent knee stiffness 7 months following primary anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Physical examination reveals full knee extension, but flexion is limited to 110 degrees (contralateral side flexes to 140 degrees). Sagittal MRI indicates improper femoral tunnel placement. Which of the following tunnel placement errors is the most likely biomechanical cause of this specific range of motion deficit?
Explanation
Question 28
A 19-year-old collegiate baseball pitcher reports medial elbow pain and a noticeable decline in throwing velocity over the past month. Physical examination reveals tenderness just distal to the medial epicondyle and localized pain with valgus stress testing at 30 degrees of elbow flexion. Which structure is the primary restraint to valgus stress during the late cocking and early acceleration phases of throwing, and what is its correct anatomic distal insertion?
Explanation
Question 29
A 26-year-old recreational volleyball player undergoes shoulder arthroscopy for persistent anterior shoulder pain. Diagnostic arthroscopy reveals an absent anterosuperior labrum and a thickened, cord-like structure extending from the superior labrum to the anterior margin of the glenoid. If the surgeon mistakenly identifies this structure as a pathological Bankart lesion and surgically secures it to the anterior glenoid rim, what is the most likely postoperative complication?

Explanation
Question 30
A 30-year-old competitive weightlifter feels a sudden 'pop' in his anterior chest while performing a heavy bench press, followed by immediate weakness and ecchymosis over the anterior axillary fold. He is diagnosed with a complete rupture of the pectoralis major tendon. During surgical repair, a thorough understanding of the insertional anatomy is essential. How does the sternocostal head insert relative to the clavicular head on the lateral lip of the bicipital groove?
Explanation
Question 31
A 55-year-old woman experiences a sudden onset of posterior medial knee pain while descending stairs. An MRI confirms a complete posterior root tear of the medial meniscus with 4 mm of medial meniscal extrusion. Biomechanically, what is the direct consequence of this specific tear pattern if left untreated?
Explanation
Question 32
A 22-year-old hockey player presents with chronic, deep groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate an aspherical femoral head with an alpha angle of 68 degrees. If the patient undergoes hip arthroscopy, what is the most typical pattern of associated intra-articular cartilage damage expected?
Explanation
Question 33
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the surgeon utilizes fluoroscopy to verify the anatomic femoral origin point (Schöttle's point). On a strictly lateral radiograph of the knee, where is this point correctly located?
Explanation
Question 34
A 9-year-old male baseball pitcher complains of lateral right elbow pain and stiffness that worsens with throwing. Examination shows a 15-degree flexion contracture. Radiographs reveal diffuse sclerosis and fragmentation involving the entire capitellum, with no loose bodies or localized subchondral bone defects. What is the most appropriate management?

Explanation
Question 35
A 17-year-old female swimmer presents with bilateral shoulder pain and a sensation that her shoulders frequently 'slip out of place.' Examination reveals positive sulcus signs bilaterally, positive apprehension and relocation tests, and a Beighton score of 7/9. There is no history of a distinct traumatic dislocation. She has undergone standard rotator cuff strengthening for 3 months with minimal improvement. What is the most appropriate next step in management?
Explanation
Question 36
A 16-year-old female soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BTB) autograft. Which of the following is the most common postoperative complication specific to this graft choice when compared to hamstring autograft?
Explanation
Question 37
A 19-year-old collegiate swimmer presents with bilateral shoulder pain and a sensation of 'slipping'. Physical examination reveals a sulcus sign of 2 cm bilaterally, positive apprehension and relocation tests, and generalized ligamentous laxity with a Beighton score of 7/9. Initial management should consist of:
Explanation
Question 38
A 45-year-old male feels a pop in the posterior aspect of his right knee while squatting to lift a heavy box. He develops a mild effusion and posterior joint line tenderness.
Coronal T2-weighted MRI of the affected knee reveals a 'ghost sign' and >3 mm extrusion of the medial meniscus. What is the most likely diagnosis?

Explanation
Question 39
A 28-year-old male weightlifter presents with a tearing sensation in his anterior chest wall while performing a heavy bench press. Examination reveals ecchymosis over the anterior axillary fold and a palpable defect. If surgical repair is planned, which portion of the pectoralis major tendon is most commonly ruptured and where does it normally insert?
Explanation
Question 40
A 24-year-old baseball pitcher presents with deep shoulder pain and a 'dead arm' sensation. An MRI arthrogram reveals a SLAP tear with detachment of the superior labrum and biceps anchor from the glenoid (Type II SLAP tear). Which of the following physical examination tests is designed to evaluate this pathology by utilizing active compression?
Explanation
Question 41
A 26-year-old professional volleyball player presents with insidious onset of posterior shoulder pain and paresthesias over the lateral aspect of the shoulder. She also reports weakness with external rotation. An MRI demonstrates fatty infiltration and atrophy isolated to the teres minor with no rotator cuff tear. What is the most likely cause of her symptoms?
Explanation
Question 42
A 30-year-old male sustains a severe varus blow to his anteromedial tibia. Clinical examination (Dial test) reveals a 15-degree increase in external rotation of the affected tibia at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of knee flexion, the external rotation is symmetric bilaterally. This finding indicates an isolated injury to which of the following structures?
Explanation
Question 43
A 20-year-old collegiate baseball pitcher complains of medial elbow pain and diminished pitching velocity for 6 weeks. A moving valgus stress test reproduces his pain.
An MR arthrogram confirms a partial tear of the anterior bundle of the ulnar collateral ligament (UCL). What is the most appropriate initial management?

Explanation
Question 44
A 25-year-old cyclist falls directly onto his shoulder. Radiographs demonstrate 150% superior displacement of the distal clavicle relative to the acromion. Physical examination notes a severe clinical deformity and the MRI shows disruption of the deltotrapezial fascia along with torn acromioclavicular and coracoclavicular ligaments. According to the Rockwood classification, what type of injury is this and what is the generally recommended treatment?
Explanation
Question 45
A 15-year-old female gymnast complains of persistent, insidious low back pain that is exacerbated by spinal extension maneuvers. Her neurological examination is completely normal. Plain AP and lateral radiographs of the lumbar spine are unremarkable. Which of the following imaging modalities is the most appropriate next step to diagnose an early, radiographically occult active pars interarticularis stress reaction?
Explanation
Question 46
A 25-year-old female undergoes an uncomplicated anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Postoperatively, she reports a well-demarcated area of numbness over the anterolateral aspect of her proximal leg. Motor function is intact. Which of the following nerves was most likely injured during the surgical approach or graft harvest?
Explanation
Question 47
A 19-year-old female collegiate swimmer presents with bilateral shoulder pain and a sensation of 'slipping' with overhead activities. Examination demonstrates a positive sulcus sign, generalized ligamentous laxity with a Beighton score of 6/9, and scapular dyskinesia. Radiographs and an MRI arthrogram (Figure 25) reveal a voluminous capsule but no frank labral tear. What is the most appropriate initial management for this patient?

Explanation
Question 48
A 28-year-old male sustains a bucket-handle tear of the medial meniscus. During arthroscopy, the tear is localized to the peripheral 3 mm of the meniscal body. To optimize healing after a planned inside-out meniscal repair, the surgeon relies on the primary source of vascularity to this region. Which of the following arterial structures is primarily responsible for the blood supply to this area?
Explanation
Question 49
A 30-year-old male presents with knee pain following a dashboard injury during a motor vehicle collision. On examination, a posterior sag sign is present. To confirm a posterior cruciate ligament (PCL) injury, the examiner performs a quadriceps active test. Which of the following correctly describes a positive finding for this test in a PCL-deficient knee?
Explanation
Question 50
A 27-year-old elite volleyball player complains of vague posterior shoulder pain and progressive weakness in external rotation. Examination reveals isolated atrophy of the infraspinatus muscle with normal supraspinatus bulk and strength. An MRI (Figure 12) demonstrates a paralabral cyst. At which of the following anatomical locations is the suprascapular nerve compression most likely occurring?
Explanation
Question 51
A 22-year-old collegiate baseball pitcher reports medial elbow pain during the late cocking and early acceleration phases of throwing. On examination, he has localized tenderness slightly distal to the medial epicondyle and a positive moving valgus stress test. An MRI of the elbow (Figure 8) demonstrates a full-thickness tear of the ulnar collateral ligament (UCL). Which of the following components represents the primary restraint to valgus stress at the elbow between 30 and 120 degrees of flexion?

Explanation
Question 52
A 14-year-old female gymnast complains of insidious onset lateral elbow pain, clicking, and a 15-degree extension deficit. Radiographs (Figure 3) demonstrate a radiolucent lesion on the capitellum. MRI confirms an unstable osteochondral defect measuring 14 mm x 12 mm with subchondral fluid and a loose body in the joint space. Six months of nonoperative management has failed. What is the most appropriate surgical management for this athlete?

Explanation
Question 53
A 24-year-old male hockey player presents with gradual onset of groin pain that worsens with deep flexion and internal rotation of the hip. A diagnostic intra-articular injection completely relieves his pain temporarily. Radiographs demonstrate an alpha angle of 75 degrees and normal acetabular version. Which of the following best describes the pathophysiologic mechanism of his condition?
Explanation
Question 54
A 31-year-old male cyclist falls directly onto his right shoulder. Clinical examination reveals a prominent distal clavicle. Radiographs (Figure 19) demonstrate 150% superior displacement of the distal clavicle relative to the acromion, with a significantly increased coracoclavicular distance. Which of the following structures must be completely disrupted to result in this radiographic appearance?

Explanation
Question 55
A 45-year-old recreational tennis player feels a sudden 'pop' in the posterior aspect of his right ankle during a match. Examination reveals a positive Thompson test and a palpable gap 4 cm proximal to the calcaneal insertion. He chooses to undergo non-operative management utilizing a functional rehabilitation protocol. Based on recent high-level evidence, how do the outcomes of functional non-operative management compare to surgical repair for acute Achilles tendon ruptures?
Explanation
Question 56
A 19-year-old collegiate football player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BTB) autograft. What is the most common cause of early graft failure (occurring within 6 months) in this patient population?
Explanation
Question 57
Figure 8 shows the MRI of a 45-year-old female who felt a pop in her posterior knee while squatting.
Imaging confirms a medial meniscus posterior root tear with 4 mm of meniscal extrusion. Which of the following biomechanical scenarios most closely mimics the contact mechanics of the knee resulting from this injury?
Explanation
Question 58
A 24-year-old male rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability associated with 25% glenoid bone loss. During the anterior approach, the conjoined tendon is aggressively retracted medially to obtain adequate exposure of the anterior glenoid neck. Which of the following nerves is at greatest risk of neuropraxia due to this maneuver?
Explanation
Question 59
A 28-year-old hockey player undergoes hip arthroscopy for cam-type femoroacetabular impingement. Postoperatively, he reports isolated burning pain and numbness over the anterolateral aspect of his operative thigh. He denies any motor weakness, groin numbness, or perineal symptoms. Injury to which of the following structures is the most likely cause of his symptoms?
Explanation
Question 60
A 22-year-old collegiate baseball pitcher presents with posterior elbow pain during the deceleration phase of throwing and a progressive loss of terminal extension. Exam shows posteromedial tenderness and pain with forced elbow extension while valgus stress is applied.
Radiographs demonstrate posteromedial olecranon osteophytes. If operative management is chosen, what is a critical technical consideration?
Explanation
Question 61
A 30-year-old male powerlifter feels a tearing sensation in his anterior chest wall while performing a heavy bench press. Clinical examination reveals a palpable defect over the anterior axillary fold and weakness with adduction and internal rotation. During surgical repair, the surgeon isolates the torn sternal head of the pectoralis major. Which of the following accurately describes the native anatomic insertion of the sternal head relative to the clavicular head?
Explanation
Question 62
A 52-year-old recreational tennis player presents with chronic right shoulder pain. MRI shows a massive, retracted, and irreparable tear of the supraspinatus and infraspinatus with Goutallier grade 4 fatty infiltration. The subscapularis and teres minor are completely intact.
Active forward elevation is 150 degrees. The surgeon plans an arthroscopic superior capsular reconstruction (SCR). What are the correct anatomic medial and lateral fixation sites for the graft?

Explanation
Question 63
A 21-year-old female soccer player with a symptomatic 4.5 cm² focal full-thickness chondral defect on the medial femoral condyle has failed prior microfracture. She is scheduled for matrix-induced autologous chondrocyte implantation (MACI). Which of the following describes the correct procedural methodology for MACI compared to first-generation ACI?
Explanation
Question 64
A 27-year-old male is brought to the emergency department following a high-speed motorcycle accident. Clinical and radiographic evaluation confirms a Schenck KD-IV knee dislocation. After closed reduction, the dorsalis pedis and posterior tibial pulses are palpable but slightly weaker compared to the contralateral limb. The ankle-brachial index (ABI) is measured at 0.85. What is the most appropriate next step in management?
Explanation
Question 65
A 26-year-old mountain biker sustains a fall onto his shoulder. Clinical examination reveals a prominent distal clavicle.
Radiographs confirm a Type V acromioclavicular (AC) joint separation. The surgeon plans an anatomic coracoclavicular (CC) ligament reconstruction. To accurately recreate the native anatomy, where should the clavicular tunnel for the conoid ligament be placed?

Explanation
Question 66
A 22-year-old football player undergoes an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft. Which of the following is the most frequently reported complication specific to this graft choice compared to hamstring autografts?
Explanation
Question 67
A 28-year-old female sustains an ultra-low velocity knee dislocation during a gymnastics routine. Her knee spontaneously reduces before arrival at the emergency department. The pedal pulses are palpable and symmetric, but her Ankle-Brachial Index (ABI) is 0.85. What is the most appropriate next step in management?
Explanation
Question 68
A 24-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability with 25% glenoid bone loss. Postoperatively, the patient reports numbness over the lateral forearm and weakness in elbow flexion. Which nerve was most likely injured during the procedure?
Explanation
Question 69
A 21-year-old hockey player presents with chronic groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate a pistol grip deformity and an alpha angle of 75 degrees. Which of the following is the most likely intra-articular finding associated with this specific morphological variant?
Explanation
Question 70
A 20-year-old collegiate baseball pitcher has medial elbow pain during the late cocking and early acceleration phases of throwing. MRI shows a high-grade tear of the ulnar collateral ligament (UCL) anterior bundle. Which of the following best describes the biomechanical property of the anterior bundle of the UCL?
Explanation
Question 71
A 45-year-old recreational weightlifter presents with deep shoulder pain and clicking. Physical examination reveals positive O'Brien and Crank tests. MRI arthrogram demonstrates a Type II SLAP tear. Six months of physical therapy and injections have failed. What is the most appropriate surgical management for this patient?
Explanation
Question 72
A 52-year-old female presents with acute onset medial knee pain after deep squatting. MRI demonstrates a medial meniscus posterior root tear with 4 mm of medial meniscal extrusion. If left completely untreated, the biomechanical consequence of this injury to the knee joint is most equivalent to which of the following?
Explanation
Question 73
A 35-year-old recreational athlete sustains an acute closed Achilles tendon rupture. He is discussing operative versus nonoperative management with his surgeon. Based on current high-level evidence utilizing an accelerated functional rehabilitation protocol, which of the following statements is true?
Explanation
Question 74
A 28-year-old male cyclist falls directly onto his right shoulder. Radiographs show a 150% superior displacement of the distal clavicle relative to the acromion. Physical exam reveals severe soft tissue tenting and pain. According to the Rockwood classification, what is the injury type and most appropriate management?
Explanation
Question 75
A 26-year-old soccer player sustains a twisting injury to his right knee. On examination, the Dial test reveals 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of knee flexion, the external rotation is equal bilaterally. What is the most likely diagnosis?
Explanation
Question 76
A 24-year-old competitive rugby player with recurrent anterior shoulder dislocations undergoes imaging which demonstrates 25% anteroinferior glenoid bone loss and an engaging Hill-Sachs lesion. He is scheduled for a Latarjet procedure.
The conjoint tendon provides a dynamic sling effect. Which nerve is most at risk during the coracoid osteotomy and transfer?
Explanation
Question 77
A 55-year-old active female experiences a sudden 'pop' in her posterior knee while squatting. She presents with posterior knee pain but no mechanical locking. MRI
reveals a medial meniscus posterior root tear with a 3-mm extrusion of the medial meniscus. If left untreated, which of the following biomechanical consequences most closely mimics this injury?

Explanation
Question 78
A 17-year-old female presents with recurrent lateral patellar dislocations. Nonoperative management has failed. Imaging demonstrates a Caton-Deschamps index of 1.1, a sulcus angle of 135 degrees, and a tibial tubercle-trochlear groove (TT-TG) distance of 24 mm on MRI. Which of the following surgical interventions is most appropriate?
Explanation
Question 79
A 26-year-old male ice hockey player presents with deep anterior groin pain exacerbated by hip flexion and internal rotation. Radiographs demonstrate an alpha angle of 65 degrees and no crossover sign. Arthroscopy is planned. During hip arthroscopy, establishing the anterior portal places which of the following structures at greatest risk?
Explanation
Question 80
A 30-year-old male fell from a height, sustaining a multiligamentous knee injury. Physical examination
demonstrates an abnormal dial test at 30 degrees of knee flexion but symmetric external rotation at 90 degrees. These findings indicate an isolated injury to which of the following structures?

Explanation
Question 81
A 20-year-old collegiate baseball pitcher reports progressive medial elbow pain and decreased pitching velocity. The moving valgus stress test is positive. MRI shows a high-grade partial tear of the anterior bundle of the ulnar collateral ligament (UCL). During surgical reconstruction, where is the most appropriate anatomical insertion site on the ulna for the graft?
Explanation
Question 82
A 68-year-old male presents with persistent right shoulder pain and pseudoparalysis. Radiographs
show superior migration of the humeral head with an acromiohumeral distance of 4 mm. MRI reveals a massive, retracted tear of the supraspinatus and infraspinatus with Goutallier grade 4 fatty infiltration. He has preserved deltoid function and an intact teres minor. Which of the following is the most appropriate surgical treatment?

Explanation
Question 83
A 22-year-old female undergoes an uncomplicated anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft. Postoperatively, she reports a localized area of numbness over the lateral aspect of her proximal leg. Which of the following nerves was most likely injured during the procedure?
Explanation
Question 84
A 28-year-old male overhead athlete presents with deep shoulder pain and clicking. The 'peel-back' mechanism is suspected to be the cause of his symptoms. Which of the following best describes the pathophysiology of this mechanism?
Explanation
Question 85
The anterolateral (AL) and posteromedial (PM) bundles of the posterior cruciate ligament (PCL) exhibit distinct tension patterns during knee motion. Which of the following accurately describes the biomechanical behavior of these bundles?
Explanation
Question 86
A 24-year-old elite baseball pitcher complains of vague, deep right shoulder pain and a recent decrease in throwing velocity. Physical examination demonstrates normal forward elevation, internal rotation of 25 degrees, and external rotation of 130 degrees. The contralateral shoulder has internal rotation of 60 degrees and external rotation of 95 degrees. MRI arthrogram reveals a type II SLAP tear. What is the most appropriate initial management?
Explanation
Question 87
A 16-year-old female presents with recurrent lateral patellar instability. She has failed a 6-month trial of physical therapy. Imaging reveals normal patellar height (Caton-Deschamps index 1.0), normal trochlear morphology, and a tibial tubercle-trochlear groove (TT-TG) distance of 23 mm on MRI. What is the most appropriate surgical intervention?
Explanation
Question 88
A 30-year-old competitive weightlifter feels a sudden 'pop' and tearing sensation in his anterior axilla while performing a heavy bench press. Examination reveals extensive ecchymosis over the medial arm and a loss of the normal anterior axillary fold contour. Weakness is most pronounced with internal rotation and adduction of the arm. Which of the following describes the most common anatomical location of this specific injury?
Explanation
Question 89
A 52-year-old previously active female experiences a sudden pop in the posterior aspect of her knee while descending into a deep squat. Over the next month, she develops significant medial joint line pain and an effusion. MRI demonstrates a medial meniscus posterior root tear. If left untreated, what is the primary biomechanical consequence of this injury?
Explanation
Question 90
A 21-year-old collegiate distance runner complains of bilateral, dull, aching anterolateral leg pain that reliably begins 15 minutes into a run and resolves after 30 minutes of rest. Intracompartmental pressure testing is performed to evaluate for chronic exertional compartment syndrome (CECS). According to the Pedowitz criteria, which of the following compartment pressure measurements confirms the diagnosis?
Explanation
Question 91
A 6-month post-operative anterior cruciate ligament (ACL) reconstruction patient presents with an inability to achieve terminal extension. The patient describes an anterior knee 'clunk' when attempting to fully extend the knee passively. Sagittal MRI shows a nodular soft tissue mass located anterior to the ACL graft in the intercondylar notch. What is the most appropriate management of this condition?
Explanation
Question 92
A 25-year-old rugby player undergoes an MRI arthrogram of the shoulder following a traumatic anterior dislocation. The images demonstrate extravasation of contrast material inferiorly down the humeral shaft, producing a characteristic 'J' sign. Which of the following is the most likely diagnosis?
Explanation
Question 93
A 14-year-old female gymnast complains of lateral elbow pain, clicking, and a 15-degree flexion contracture. Radiographs reveal a radiolucency in the capitellum. MRI demonstrates a 12 mm osteochondral defect of the capitellum. Which of the following MRI findings is the strongest absolute indication for surgical intervention?
Explanation
Question 94
During a physical examination of a football player who sustained a direct blow to the anteromedial aspect of the tibia, you perform the dial test. The patient exhibits 20 degrees of increased external rotation of the tibia compared to the uninjured leg at 30 degrees of knee flexion. However, at 90 degrees of knee flexion, the external rotation is symmetric to the uninjured side. This examination finding is most indicative of an isolated injury to which of the following structures?
Explanation
Question 95
A 28-year-old male is brought to the emergency department after a high-velocity knee dislocation involving disruption of the ACL, PCL, and posterolateral corner (KD-III). On physical examination, he demonstrates a profound foot drop and inability to extend his toes. Vascular exam is normal. What is the most common mechanism of injury for the neurological deficit described in this specific clinical scenario?
Explanation
Question 96
A 22-year-old collegiate football player sustains a recurrent anterior shoulder dislocation. Imaging (Figure 15) shows a significant anteroinferior glenoid bone loss estimated at 27%. Which of the following is the most appropriate surgical management?
Explanation
Question 97
A 28-year-old female recreational skier injured her knee. MRI (Figure 8) demonstrates an acute anterior cruciate ligament (ACL) tear and an extrusion of the medial meniscus on the coronal sequence with a missing meniscal bow tie sign on the sagittal sequence. Which of the following is the most appropriate management for the meniscus during ACL reconstruction?
Explanation
Question 98
A 30-year-old man sustains a direct blow to the anteromedial aspect of his knee. Examination reveals a positive dial test with 15 degrees of increased external rotation at both 30 and 90 degrees of knee flexion compared to the contralateral side. He also has a positive posterior drawer test. What is the most likely combination of injured structures?
Explanation
Question 99
A 21-year-old collegiate baseball pitcher complains of medial elbow pain during the late cocking and early acceleration phases of throwing. He reports feeling a 'pop' during his last outing. The moving valgus stress test is positive. An MRI (Figure 10) confirms a high-grade tear of the anterior bundle of the ulnar collateral ligament (UCL) at its insertion on the sublime tubercle. Which of the following graft choices is most commonly used for UCL reconstruction in this scenario?
Explanation
Question 100
A 19-year-old female gymnast complains of bilateral shoulder pain and a feeling of her shoulders 'slipping out of place' during routines. Physical examination reveals a positive sulcus sign bilaterally that does not obliterate with external rotation, a positive Beighton score of 7/9, and symmetric voluntary posterior subluxation. What is the most appropriate initial management?
Explanation
None
