Orthopedic Basic 2026 MCQs: Board Review Questions & Answers (Part 4)

Key Takeaway
Discover the latest medical recommendations for Orthopedic Basic 2026 MCQs: Board Review Questions & Answers (Part 4). Top-rated Orthopedic Basic 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Basic 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Explanation
Question 2
Figures 63a and 63b show the radiographs of an 11-year-old girl who sustained a twisting injury of the knee playing soccer. She is now asymptomatic. What is the appropriate treatment of the lesion?
Explanation
Question 3
A 21-year-old man is referred for evaluation of a lesion in the left proximal femur that was discovered when he was undergoing an upper gastrointestinal series. He reports no hip or thigh pain. Radiographs are shown in Figures 64a and 64b. What is the best course of action?
Explanation
Question 4
A 17-year-old boy has had elbow pain for the past 6 weeks. A radiograph, MRI scans, and biopsy specimens are shown in Figures 65a through 65e. What is the most likely diagnosis?
Explanation
Question 5
What is the most common site of metastases from a soft-tissue sarcoma?
Explanation
Question 6
A 45-year-old woman has had right wrist pain for the past 2 months. A radiograph, bone scan, and MRI scan are shown in Figures 66a through 66c, and a photomicrograph is shown in Figure 66d. What is the most likely diagnosis?
Explanation
Question 7
An otherwise healthy 16-year-old dancer reports a 1-month history of leg pain. AP and lateral radiographs of the distal femur are shown in Figures 67a and 67b. What is the next most appropriate step in management?
Explanation
Question 8
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
Question 9
A 47-year-old woman has had left medial clavicle pain for the past 6 months. History is remarkable for mediastinal non-Hodgkin's lymphoma, treated with mantel radiation 22 years ago. A radiograph, CT scan, MRI scan, and a biopsy specimen are shown in Figures 68a through 68d. What is the most likely diagnosis?
Explanation
Question 10
In 1980, a 32-year-old woman was found to have right breast mass, and a biopsy revealed adenocarcinoma. She underwent a mastectomy at that time, with no other treatment. Five years later, she noticed a lump in the left breast and underwent a left mastectomy. Seven lymph nodes were positive. In 2006, she now reports hip and thigh pain for the past 3 months. Figures 69a and 69b show AP and lateral radiographs of the femur. A bone scan shows a solitary lesion. Following radiographic staging, what is the next most appropriate step in management?
Explanation
Question 11
What is the mechanism of action of bisphosphonates?
Explanation
Question 12
A 16-year-old girl has had hip pain for 1 year. Approximately 2 months ago she noted the development of a hard mass in the right buttock that has steadily increased in size. She now reports severe pain in the right buttock, with radiation down the leg and numbness involving the right foot and toes. A radiograph is shown in Figure 70a and an axial postcontrast T1-weighted MRI scan is shown in Figure 70b. A biopsy specimen is shown in Figure 70c. The chest CT shows multiple lung metastases. Treatment of this lesion should consist of
Explanation
Question 13
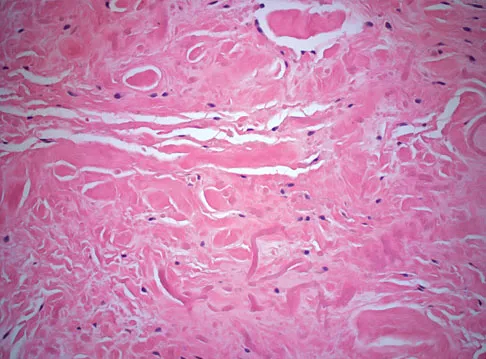
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
Question 14
A 69-year-old woman reports a painful clicking in her right shoulder. A soft-tissue mass is palpated at the lower portion of the scapula. Based on the MRI scan and biopsy specimens shown in Figures 72a through 72c, what is the most likely diagnosis?
Explanation
Question 15
A 40-year-old man has a painless mass around his left ankle. He notes minimal growth over the past year. An MRI scan is shown in Figure 73a, and biopsy specimens are shown in Figures 73b and 73c. What is the most likely diagnosis?
Explanation
Question 16
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?
Explanation
Question 17
Which of the following prognostic indicators is associated with the least favorable outcome for patients newly diagnosed with osteosarcoma?
Explanation
Question 18
A 12-year-old girl has had increasing left knee pain for the past 3 months. A radiograph is shown in Figure 75a, and low- and high-power photomicrographs are shown in Figures 75b and 75c. What is the most appropriate treatment?
Explanation
Question 19
A 58-year-old woman has had a slowly progressing mass over the distal interphalangeal (DIP) joint of her dominant hand with a worsening deformity of her nail. She has no significant medical history but underwent bilateral knee arthroplasties 1 year ago. Radiographs reveal a small osteophyte at the DIP joint dorsally. A clinical photograph and a biopsy specimen are shown in Figures 76a and 76b. What is the most likely diagnosis?
Explanation
Question 20
A 13-year-old boy has had pain and swelling in his ankle for the past several months. Based on the radiograph, MRI scan, and biopsy specimen shown in Figures 77a through 77c, what is the best course of action?
Explanation
Question 21
A 39-year-old man has had a foot mass for the past several months. MRI scans are shown in Figures 78a through 78c. A core biopsy specimen reveals synovial sarcoma, and a staging chest CT scan is normal. Which of the following treatments offers the best local tumor control and expedites the patient's return to normal function?
Explanation
Question 22
A 10-month-old boy has multiple skeletal lesions and a skin rash that he has had since he was a newborn. Based on the radiographs and biopsy specimens shown in Figures 79a through 79d, what is the most likely diagnosis?
Explanation
Question 23
Which of the following is not a characteristic of synovial sarcomas?
Explanation
Question 24
Mutations of what gene are associated with the subsequent development of osteosarcoma?
Explanation
Question 25
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?
Explanation
Question 26
Bone morphogenetic proteins (BMPs) play a crucial role in osteoinduction and fracture healing. They exert their intracellular effects primarily by binding to which of the following types of cell-surface receptors?
Explanation
Question 27
A 30-year-old woman presents with progressive knee pain. Radiographs reveal an eccentric, purely lytic epiphyseal lesion extending to the subchondral bone in the distal femur. A biopsy is performed, and the diagnosis of a Giant Cell Tumor (GCT) of bone is confirmed. Which of the following best describes the primary neoplastic cell population in this tumor?
Explanation
Question 28
A 14-year-old boy presents with thigh pain and a low-grade fever. Radiographs show a permeative lytic lesion in the diaphysis of the femur with an 'onion-skin' periosteal reaction. A biopsy confirms Ewing sarcoma. Which of the following chromosomal translocations is most commonly associated with this diagnosis?
Explanation
Question 29
Articular cartilage relies on a highly organized extracellular matrix for its biomechanical properties. In which structural zone of articular cartilage are the type II collagen fibers oriented parallel to the joint surface and the highest concentration of water found?
Explanation
Question 30
A 4-year-old boy is evaluated for frequent fractures and progressive hearing loss. Radiographs demonstrate a diffuse, symmetric skeletal sclerosis with a 'bone within bone' appearance. The underlying pathogenesis of his disease most likely involves a defect in the function of which of the following?
Explanation
Question 31
Denosumab is an effective pharmacological agent used in the management of osteoporosis, bone metastases, and unresectable giant cell tumors of bone. It decreases bone resorption by directly targeting and inhibiting which of the following?
Explanation
Question 32
A 55-year-old man presents with an acute, painful, swollen left knee. Joint aspiration yields synovial fluid with a white blood cell count of 45,000 cells/mm³, consisting of 80% polymorphonuclear leukocytes. Under polarized light microscopy, rhomboid-shaped crystals are visualized within the neutrophils. Which of the following is the most likely composition of these crystals?
Explanation
Question 33
Vitamin D homeostasis is critical for normal bone mineralization. Which enzyme is responsible for the conversion of 25-hydroxyvitamin D to its most physiologically active form, 1,25-dihydroxyvitamin D, and where does this primarily occur?
Explanation
Question 34
A 16-year-old girl is treated for a high-grade, intramedullary conventional osteosarcoma of the distal femur. After undergoing a standard regimen of neoadjuvant chemotherapy, she undergoes a wide surgical resection of the tumor. Which of the following parameters determined from the resected specimen is the most important independent prognostic indicator for her long-term survival?
Explanation
Question 35
Vitamin C deficiency (scurvy) profoundly affects bone and connective tissue formation, leading to poor wound healing, capillary fragility, and defective osteoid matrix. This occurs because ascorbic acid is an essential cofactor in which specific step of collagen synthesis?
Explanation
Question 36
A 45-year-old male smoker is undergoing a single-level anterior lumbar interbody fusion (ALIF). The surgeon decides to use a commercially available recombinant human bone morphogenetic protein (rhBMP) to enhance fusion. Which of the following best describes the intracellular signaling mechanism of the FDA-approved rhBMP used for this indication?
Explanation
Question 37
Highly cross-linked polyethylene (HXLPE) has become the standard bearing surface in total hip arthroplasty to minimize wear and osteolysis. Which of the following is a direct mechanical consequence of the irradiation process used to manufacture HXLPE compared to conventional ultra-high-molecular-weight polyethylene (UHMWPE)?
Explanation
Question 38
A 32-year-old woman presents with a recurrence of an unresectable giant cell tumor (GCT) of the sacrum. The multidisciplinary tumor board recommends treatment with denosumab. What is the specific mechanism of action of this medication in the context of a giant cell tumor?
Explanation
Question 39
A 14-year-old boy presents with a history of multiple fractures and anemia. Radiographs demonstrate diffusely dense bones with a 'bone-in-bone' appearance. Genetic analysis reveals a mutation in the TCIRG1 gene. What is the primary cellular defect responsible for this patient's condition?
Explanation
Question 40
During a single-stage revision total knee arthroplasty for a periprosthetic joint infection, thorough debridement is performed to remove the bacterial biofilm. Which of the following stages of biofilm formation is characterized by the initial secretion of a protective extracellular polymeric substance (EPS) and the beginning of irreversible bacterial adherence?
Explanation
Question 41
In a biomechanical study, an intact anterior cruciate ligament (ACL) specimen is subjected to a constant tensile load over 24 hours. The investigators observe a progressive increase in ligament deformation (length) over time despite the load remaining unchanged. This viscoelastic phenomenon is known as:
Explanation
Question 42
Tranexamic acid (TXA) is widely utilized to minimize blood loss during primary and revision total joint arthroplasty. Which of the following best describes the pharmacological mechanism of TXA?
Explanation
Question 43
A 28-year-old man sustains a closed spiral fracture of the middle third of the humerus. On examination, he is unable to extend his wrist or digits. Based on the Seddon classification, if this injury is an axonotmesis, what is the expected microscopic state of the nerve at the zone of injury?
Explanation
Question 44
During normal human gait on a level surface, sufficient knee flexion during the swing phase is critical for foot clearance. What is the approximate maximum degree of knee flexion achieved during normal level walking?
Explanation
Question 45
A 20-year-old college student complains of deep, aching anterior thigh pain that is notably worse at night. The pain is consistently and completely relieved within 30 minutes of taking ibuprofen.
A radiograph and subsequent CT scan reveal a 0.8 cm radiolucent nidus surrounded by dense reactive sclerosis in the femoral diaphysis. What is the most widely accepted definitive, minimally invasive treatment for this condition if medical management is intolerable?

Explanation
Question 46
A 45-year-old man presents with an increasingly painful shoulder over the past 6 months. Radiographs demonstrate a lytic lesion with rings and arcs of calcification in the proximal humerus, exhibiting endosteal scalloping that exceeds two-thirds of the cortical thickness. Biopsy reveals hypercellular hyaline cartilage with distinct permeation into the surrounding marrow spaces. What is the most appropriate management for this patient?
Explanation
Question 47
A 19-year-old man reports persistent thigh pain that is significantly worse at night and reliably relieved within 30 minutes of taking ibuprofen. Computed tomography (CT) of the femur demonstrates a 1.2 cm radiolucent nidus surrounded by dense reactive sclerotic bone in the femoral diaphysis. What is the primary molecular mechanism responsible for the severe pain and its relief by nonsteroidal anti-inflammatory drugs (NSAIDs) in this condition?
Explanation
Question 48
A 14-year-old girl presents with a rapidly expanding, painful mass in her distal femur. MRI reveals an expansile, multiloculated lytic lesion with prominent fluid-fluid levels. A biopsy confirms blood-filled spaces lacking a true endothelial lining, with giant cells present in the fibrous septa. What genetic translocation is most specific and diagnostic for the primary form of this neoplastic lesion?
Explanation
Question 49
A 16-year-old boy has recently completed a standard course of neoadjuvant chemotherapy for a conventional high-grade osteosarcoma of the distal femur, followed by wide surgical resection. Pathological examination of the resected tumor specimen reveals 95% tumor necrosis. Which of the following statements is true regarding this specific finding?
Explanation
Question 50
A 12-year-old boy presents with intermittent low-grade fevers, mild weight loss, and a painful, swollen mid-thigh. Radiographs demonstrate a permeative, ill-defined destructive lesion in the femoral diaphysis with an 'onion-skin' periosteal reaction. Biopsy reveals sheets of uniform, small, round, blue cells. Which immunohistochemical marker is most consistently and strongly positive in this tumor?
Explanation
Question 51
A 14-year-old boy presents with multiple painless, hard bony protuberances around his knees, ankles, and shoulders that have been present since early childhood. Radiographs demonstrate multiple pedunculated and sessile bone lesions pointing away from the joints, showing continuity of the cortex and medullary cavity with the host bone. Mutations in which of the following genes are most commonly responsible for this condition, and what is their normal cellular function?
Explanation
Question 52
An 8-year-old boy sustains a minor fall and presents with a pathologic fracture of the proximal humerus. Radiographs demonstrate a centrally located, completely radiolucent metaphyseal lesion extending to the physis, with a small cortical fragment resting at the dependent portion of the cyst ('fallen leaf' sign). Once the fracture heals, the cyst remains persistent and active. What is the most appropriate initial management for the cyst?
Explanation
Question 53
A 32-year-old woman presents with persistent knee pain. Radiographs demonstrate an eccentric, lytic, expansile lesion in the distal femur epiphysis extending to the subchondral bone, with no sclerotic margin. Histological examination reveals numerous multinucleated giant cells distributed evenly throughout a background of mononuclear stromal cells. Which cell type in this lesion is the true neoplastic population, and what is the key molecular target for specific medical therapy?
Explanation
Question 54
A 25-year-old woman presents with hip pain and an impending pathological fracture of the proximal femur. Radiographs reveal a classic 'shepherd's crook' deformity with a diaphyseal 'ground-glass' appearance. The patient's medical history includes precocious puberty and hyperthyroidism. Which of the following best describes the underlying cellular pathophysiology of her musculoskeletal and endocrine abnormalities?
Explanation
Question 55
A 28-year-old man presents with a slow-growing, deep, painful mass in his popliteal fossa. MRI shows a well-circumscribed soft tissue mass adjacent to the knee joint but not originating from the joint space itself. Core needle biopsy reveals a biphasic tumor consisting of both spindle cells and epithelial-like gland formations. Which cytogenetic abnormality is diagnostic for this tumor?
Explanation
Question 56
A 14-year-old boy presents with progressive night pain in his proximal tibia that is reliably relieved by oral ibuprofen. Radiographs demonstrate a 1-cm radiolucent nidus surrounded by dense reactive sclerosis. What is the primary mechanism by which the nonsteroidal anti-inflammatory drug (NSAID) relieves his symptoms in this specific condition?
Explanation
Question 57
According to standard orthopedic biomechanical principles, which of the following geometric modifications to a cortical screw will most effectively increase its pull-out strength in bone?
Explanation
Question 58
A 65-year-old woman is scheduled to undergo a total hip arthroplasty. The surgeon plans to use a highly cross-linked polyethylene (HXLPE) liner. Which of the following describes the primary tribological and mechanical trade-off associated with highly cross-linked polyethylene compared to conventional ultra-high-molecular-weight polyethylene (UHMWPE)?
Explanation
Question 59
A 45-year-old man presents with chronic, dull lower back and perineal pain. Advanced imaging reveals a destructive, midline expansile lytic lesion in the sacrum. Histological examination of a biopsy specimen demonstrates large, vacuolated cells with a bubbly cytoplasm arranged in cords within a myxoid background. Which of the following immunohistochemical markers is most likely to be positive in this lesion?
Explanation
Question 60
During a direct anterior approach to the hip for a total hip arthroplasty, the surgeon develops the internervous plane between the sartorius and the tensor fasciae latae. Which of the following nerves is at greatest risk of iatrogenic injury during the superficial dissection of this approach?
Explanation
Question 61
A 62-year-old man presents with progressive anterolateral bowing of his left tibia. He reports his hat size has increased over the last few years. Laboratory evaluation reveals a markedly elevated serum alkaline phosphatase, but normal serum calcium, phosphorus, and parathyroid hormone levels. What is the fundamental cellular abnormality initiating this disease process?
Explanation
Question 62
In the ultrastructure of normal adult articular cartilage, which zone is characterized by the highest concentration of proteoglycans, the lowest water content, and collagen fibrils arranged perpendicular to the articular surface?
Explanation
Question 63
A 68-year-old man is prescribed rivaroxaban for venous thromboembolism prophylaxis following an elective total knee arthroplasty. What is the precise mechanism of action of this pharmacological agent?
Explanation
Question 64
Which of the following biological descriptions accurately represents primary (strain-free) bone healing?
Explanation
Question 65
A 16-year-old boy is evaluated for persistent left thigh pain and swelling. Radiographs show a permeative, aggressive diaphyseal lesion in the femur with a prominent 'onion-skin' periosteal reaction. A core needle biopsy is performed. Molecular cytogenetic testing of the biopsy specimen is most likely to reveal which of the following chromosomal translocations?
Explanation
Question 66
A 28-year-old man presents with a slow-growing, painless mass in his foot. MRI shows a well-circumscribed soft tissue mass adjacent to the plantar fascia. Biopsy reveals a biphasic tumor with both epithelial and spindle cell components. What is the most characteristic chromosomal translocation associated with this diagnosis?
Explanation
Question 67
A 35-year-old woman presents with knee pain. Radiographs reveal an eccentric, lytic lesion in the distal femur extending to the subchondral bone without a sclerotic rim. Biopsy confirms a giant cell tumor of bone. She is treated with denosumab preoperatively. What is the mechanism of action of denosumab in this clinical setting?
Explanation
Question 68
A 12-year-old boy presents with thigh pain and low-grade fevers. Radiographs show a permeative diaphyseal lesion in the femur with a classic 'onion-skin' periosteal reaction. Biopsy shows small round blue cells. Immunohistochemistry is strongly positive for CD99. Which of the following gene fusions is most commonly responsible for this tumor?
Explanation
Question 69
A 16-year-old girl is diagnosed with high-grade conventional osteosarcoma of the proximal tibia. She undergoes neoadjuvant chemotherapy followed by wide surgical resection. Which of the following factors has been shown to be the most important prognostic indicator for overall survival in this patient?
Explanation
Question 70
A 9-year-old girl presents with a limp. Radiographs of her proximal femur show a characteristic 'shepherd's crook' deformity with a ground-glass appearance of the medullary canal. She also has irregular café-au-lait spots on her trunk and a history of precocious puberty. This condition is primarily caused by a mutation leading to which of the following cellular abnormalities?
Explanation
Question 71
A 55-year-old man presents with progressive deep thigh pain, worse at night. Radiographs demonstrate a large, predominantly lytic lesion in the proximal femur with endosteal scalloping greater than two-thirds of the cortical thickness and focal cortical breakthrough. MRI shows a lobulated mass with high signal intensity on T2-weighted images. Biopsy is read as a grade 2 chondrosarcoma. What is the most appropriate definitive management for this patient?
Explanation
Question 72
A 14-year-old boy presents with rapid swelling and pain in his left humerus. Radiographs show an expansile, eccentrically located, lytic metaphyseal lesion with 'blown-out' cortices. MRI reveals multiple fluid-fluid levels. Biopsy confirms a primary aneurysmal bone cyst. Primary aneurysmal bone cysts are frequently associated with a recurrent chromosomal translocation resulting in the upregulation of which of the following genes?
Explanation
Question 73
A 19-year-old male presents with right shin pain that is worse at night and dramatically improves with ibuprofen. Radiographs reveal cortical thickening of the anterior tibial diaphysis. CT scan shows a 7-mm radiolucent nidus surrounded by dense reactive sclerosis. What is the primary biochemical mechanism responsible for the classic pain pattern in this condition?
Explanation
Question 74
A 35-year-old woman presents with chronic, progressive swelling and catching of her right knee. Aspiration yields dark, bloody synovial fluid. MRI reveals a large, lobulated intra-articular mass with 'blooming artifact' on gradient-echo sequences. The pathogenesis of this condition is primarily driven by a translocation resulting in the overexpression of which of the following factors?
Explanation
Question 75
A 28-year-old woman presents with a slow-growing, painless mass on the posterior aspect of her distal thigh. Radiographs demonstrate a heavily ossified, lobulated mass attached to the posterior cortex of the distal femur by a broad base, with a radiolucent 'string sign' visible between the tumor and the underlying bone. Which of the following molecular alterations is most characteristic of this tumor?
Explanation
Question 76
A 14-year-old boy presents with a 2-month history of worsening thigh pain, worse at night, and intermittent fevers. Radiographs show a permeative, destructive diaphyseal lesion with an 'onion-skin' periosteal reaction in the femur. Biopsy reveals small, round blue cells that strongly express CD99. Which of the following chromosomal translocations is most commonly associated with this patient's diagnosis?
Explanation
Question 77
A 32-year-old woman presents with persistent knee pain. Radiographs demonstrate an eccentric, lytic epiphyseal lesion in the distal femur without sclerotic margins. A core needle biopsy reveals mononuclear cells intermixed with multinucleated giant cells. The patient is prescribed denosumab to downstage the tumor prior to surgery. What is the mechanism of action of this medication in the context of this tumor?
Explanation
Question 78
A 65-year-old man presents with progressive bowing of his right tibia and dull, aching leg pain. Blood tests reveal an isolated, significantly elevated alkaline phosphatase level with normal calcium and phosphorus. Radiographs show cortical thickening, trabecular coarsening, and anterior bowing of the tibia. A biopsy of the bone would most likely demonstrate which of the following histologic features?
Explanation
Question 79
A 19-year-old man presents with aching pain in his left mid-thigh that has been present for 6 months. The pain is characteristically worse at night and is dramatically relieved within 30 minutes of taking ibuprofen. CT scan demonstrates a 0.8 cm radiolucent nidus surrounded by dense reactive cortical sclerosis in the femoral diaphysis. The dramatic pain relief with NSAIDs is due to the inhibition of which of the following substances synthesized in high amounts by this lesion?
Explanation
Question 80
A 12-year-old girl presents with pain and swelling over her left proximal humerus after a minor fall. Radiographs show an expansile, eccentric, radiolucent lesion in the metaphysis. MRI demonstrates multiple internal fluid-fluid levels. Biopsy reveals blood-filled cystic spaces separated by fibrous septa containing osteoclast-like giant cells. Which of the following genetic alterations is most characteristic of the primary form of this lesion?
Explanation
Question 81
A 68-year-old man presents with lower back pain and fatigue. Radiographs of the lumbar spine and pelvis reveal multiple 'punched-out' lytic lesions without reactive sclerosis. Laboratory studies show mild hypercalcemia and a normocytic anemia. Which of the following diagnostic tests would be most appropriate to confirm the underlying diagnosis and evaluate the extent of skeletal involvement?
Explanation
Question 82
A 55-year-old man undergoes radiographs of his shoulder for rotator cuff symptoms, which incidentally reveal a 4 cm calcified lesion in the proximal humeral metaphysis. The calcifications are described as having a 'rings and arcs' appearance. Which of the following MRI findings would most strongly suggest a diagnosis of low-grade chondrosarcoma rather than a benign enchondroma?
Explanation
Question 83
An 8-year-old boy presents with mild arm pain after throwing a baseball. Radiographs of the humerus reveal a central, lytic lesion in the proximal diaphysis with a small piece of cortical bone resting at the dependent portion of the lesion. There is mild expansile remodeling but no other cortical breach. What is the most appropriate initial management for this patient?
Explanation
Question 84
A 10-year-old girl is evaluated for a leg length discrepancy and a limp. Radiographs of the left femur reveal a large medullary lesion with a 'ground-glass' appearance and a characteristic 'shepherd's crook' deformity of the proximal femur. She also has several large, irregular hyperpigmented macules on her back and signs of precocious puberty. Which of the following best describes the pathogenesis of her underlying condition?
Explanation
Question 85
A 15-year-old boy twists his ankle while playing basketball. Radiographs are negative for an acute fracture but incidentally demonstrate an eccentric, cortically based, well-circumscribed radiolucent lesion with a sclerotic margin in the distal tibial metaphysis. The lesion measures 3 cm in length. He has no pain localized to the site of the lesion itself. What is the most appropriate management of this incidental finding?
Explanation
Question 86
A 45-year-old man undergoes a complex revision total hip arthroplasty utilizing a massive structural cortical allograft. Which of the following best describes the expected incorporation process of this allograft compared to a cancellous autograft?
Explanation
Question 87
A 30-year-old woman presents with multiple asymmetric cartilaginous lesions in the short tubular bones of her hands and long bones, consistent with Ollier disease. What is the approximate lifetime risk of malignant transformation of these lesions, and what is the most common gene mutation associated with this condition?
Explanation
Question 88
A 32-year-old woman presents with a lytic, expansile lesion in the distal femur extending to the subchondral bone. Biopsy confirms a giant cell tumor of bone. She is treated preoperatively with denosumab to consolidate the lesion. What is the specific mechanism of action of this medication?
Explanation
Question 89
A 16-year-old boy presents with severe, progressive right thigh pain that is worse at night and dramatically improves with ibuprofen. Radiographs show a thickened cortical diaphyseal area, and a CT scan
reveals a 7-mm radiolucent nidus with central calcification. What inflammatory mediator is found in high concentrations within the nidus of this lesion?

Explanation
Question 90
A 28-year-old man presents with a slow-growing, painful mass in his plantar foot. MRI reveals a soft tissue mass with heterogeneous signal intensity, and a core biopsy is performed. The diagnosis of synovial sarcoma is confirmed. Which of the following cytogenetic abnormalities is most characteristic of this tumor?
Explanation
Question 91
An asymptomatic 9-year-old boy undergoes a radiograph of his tibia after a minor contusion. The radiograph
reveals an eccentrically located, multilobulated, lytic lesion with a sclerotic rim in the distal tibial metaphysis. It measures 2 cm in length and occupies less than 20% of the bone diameter. What is the most appropriate management?

Explanation
Question 92
A 35-year-old woman presents with a painless mass on the posterior aspect of her distal thigh. Radiographs
demonstrate a dense, heavily ossified, broad-based mass attached to the posterior cortex of the distal femur with a 'string sign' radiolucency. Biopsy reveals well-differentiated bone trabeculae within a low-grade fibroblastic stroma. Which of the following is true regarding this diagnosis?
Explanation
Question 93
Which zone of normal articular cartilage contains the largest diameter collagen fibrils oriented strictly perpendicular to the articular surface, providing the primary resistance to compressive forces?
Explanation
Question 94
A 68-year-old woman taking oral alendronate for 10 years presents with a 3-month history of dull right thigh pain. Radiographs reveal focal lateral cortical thickening (beaking) and a transverse radiolucent line in the subtrochanteric femur. What is the fundamental alteration in bone physiology responsible for this condition?
Explanation
Question 95
A 14-year-old boy presents with fever, weight loss, and progressive pain in his left mid-thigh. Radiographs
show a destructive, permeative diaphyseal lesion with a large soft tissue extension and an 'onion-skin' periosteal reaction. Histological examination reveals sheets of uniform, small, round blue cells that strongly express membranous CD99. What is the most important initial step in the systemic staging of this patient?
Explanation
Question 96
A researcher is developing a novel therapeutic agent for osteoporosis that directly inhibits the physiological processes at the ruffled border of osteoclasts. Which of the following best describes the primary mechanism by which osteoclasts create the acidic environment necessary for bone resorption at this ruffled border?
Explanation
Question 97
A 65-year-old man who underwent a primary total hip arthroplasty using a titanium stem and a cobalt-chromium modular head 5 years ago presents with new-onset groin pain. Laboratory tests show elevated serum cobalt levels, while chromium levels are mildly elevated. MRI reveals a solid-cystic pseudotumor around the hip joint. The primary mechanism responsible for the release of these metal ions at the modular head-neck junction is best described as:
Explanation
Question 98
During the process of secondary fracture healing, the differentiation of mesenchymal stem cells is highly dependent on the local mechanical and biological environment. According to Carter's mechanobiology principles and Perren's strain theory, which of the following environments most strongly favors the differentiation of these cells into chondrocytes (cartilage formation)?
Explanation
Question 99
A 22-year-old female athlete tears her anterior cruciate ligament (ACL) and undergoes reconstruction using a bone-patellar tendon-bone (BPTB) autograft. The surgeon discusses the biological remodeling process of the graft, known as 'ligamentization'. At which postoperative time point is the structural graft mechanically at its weakest, owing primarily to the phase of revascularization and cellular repopulation?
Explanation
Question 100
A 14-year-old boy presents with an expanding, painful mass in the diaphysis of his left femur. Radiographs display an aggressive, permeative osteolytic lesion with a 'laminated' (onion-skin) periosteal reaction. Core needle biopsy reveals sheets of uniform, small round blue cells with scant cytoplasm. Immunohistochemical staining is strongly positive for CD99. Which of the following chromosomal translocations is most characteristic of this diagnosis?
Explanation
None
