Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 3)

Key Takeaway
This article provides essential research regarding Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 3). Top-rated Orthopedic Upper Extremity 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 3)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?
Explanation
Question 2
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
Question 3
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?
Explanation
Question 4
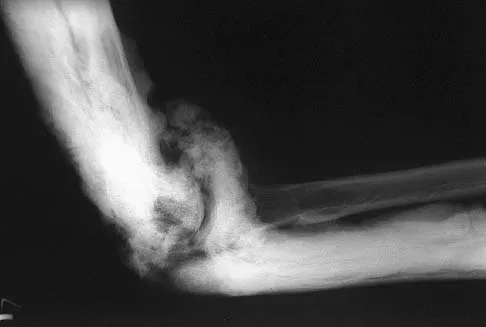
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?
Explanation
Question 5
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O'Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
Explanation
Question 6
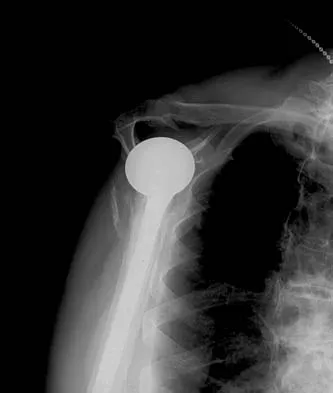
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
Question 7
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended?
Explanation
Question 8
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?
Explanation
Question 9
A 17-year-old high school football player reports wrist pain 5 months after the conclusion of the football season. A radiograph and MRI scan are shown in Figures 29a and 29b. What is the recommended intervention?
Explanation
Question 10
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?
Explanation
Question 11
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Explanation
Question 12
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
Explanation
Question 13
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
Question 14
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
Question 15
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Question 16
A 40-year-old unrestrained passenger reports chest wall pain after a motor vehicle accident. Which of the following structures is most important in preventing the injury shown in Figure 33?
Explanation
Question 17
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?
Explanation
Question 18
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
Question 19
What is the most likely cause of the lesion shown in Figures 35a and 35b?
Explanation
Question 20
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
Question 21
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
Question 22
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
Question 23
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
Question 24
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
Question 25
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
Explanation
Question 26
A 45-year-old competitive weightlifter feels a sudden, painful 'pop' in his anterior elbow while performing heavy bicep curls. Examination reveals a 'Popeye' deformity and significant weakness in forearm supination. He undergoes a distal biceps tendon repair using a traditional two-incision technique. Compared to a single anterior incision approach, which of the following complications is significantly more likely with the two-incision technique?
Explanation
Question 27
A 35-year-old woman falls on an outstretched hand and sustains a complex elbow injury. Radiographs and CT scan demonstrate a posterior elbow dislocation, a comminuted radial head fracture, and a Type II coronoid fracture. Following closed reduction, the elbow remains grossly unstable. During open surgical reconstruction, what is the most widely accepted sequence of fixation to restore elbow stability?
Explanation
Question 28
A 74-year-old woman presents with severe shoulder pain after a mechanical fall. Radiographs demonstrate a displaced 4-part proximal humerus fracture with severe comminution of the tuberosities. Her medical history is significant for chronic pseudoparalysis of the affected shoulder secondary to a known, massive, irreparable rotator cuff tear. What is the most appropriate surgical management?
Explanation
Question 29
A 48-year-old manual laborer complains of a 5-year history of progressive, aching right wrist pain. Radiographs reveal a scaphoid nonunion with advanced collapse (SNAC). There is prominent arthritic change at the radioscaphoid joint and the capitolunate joint, but the radiolunate articulation is completely spared. Which of the following is the most appropriate surgical treatment?
Explanation
Question 30
A 22-year-old collegiate rugby player undergoes a Latarjet procedure for recurrent anterior shoulder instability associated with 28% anterior glenoid bone loss. The procedure involves transferring the coracoid process to the anterior glenoid neck. Which muscular structure is transferred along with the coracoid to provide a dynamic 'sling' effect across the anteroinferior capsule?
Explanation
Question 31
Six weeks after nonoperative management of a nondisplaced distal radius fracture, a 62-year-old woman presents with the sudden inability to actively extend the interphalangeal joint of her thumb. An extensor indicis proprius (EIP) to extensor pollicis longus (EPL) tendon transfer is planned. At the level of the metacarpophalangeal joint of the index finger, where is the EIP tendon located relative to the extensor digitorum communis (EDC) tendon?
Explanation
Question 32
A 29-year-old elite volleyball attacker reports vague posterior shoulder pain and progressive weakness. Physical examination reveals isolated weakness in external rotation and profound atrophy of the infraspinatus fossa. Abduction strength and supraspinatus bulk are entirely normal. An MRI confirms a paralabral cyst compressing a peripheral nerve. At what specific anatomic location is the nerve compression occurring?
Explanation
Question 33
A 27-year-old woman complains of progressive dorsal wrist pain. Radiographs demonstrate sclerosis, fragmentation, and flattening of the lunate without carpal collapse. Her ulnar variance is determined to be -3 mm. Based on the most likely diagnosis, what is the preferred initial surgical intervention?
Explanation
Question 34
A 52-year-old man with severe, electromyographically confirmed cubital tunnel syndrome is undergoing an anterior subcutaneous transposition of the ulnar nerve. During the transposition, a specific structural band extending from the medial epicondyle to the medial humerus must be resected to prevent secondary kinking of the nerve as it is moved anteriorly. What is this structure?
Explanation
Question 35
A 38-year-old man falls from a height of 10 feet, sustaining a severely comminuted, unsalvageable radial head fracture. The surgeon performs an isolated radial head excision. Six months later, the patient develops severe, progressive ulnar-sided wrist pain. Radiographs reveal 5 mm of positive ulnar variance. What concurrent injury was missed at the time of the initial trauma?
Explanation
Question 36
A 55-year-old woman sustained a distal radius fracture treated with a volar locking plate. Three months postoperatively, she presents with inability to actively flex the interphalangeal joint of her thumb. Radiographs show plate placement distal to the watershed line. Which tendon is most commonly ruptured in this scenario?
Explanation
Question 37
A 45-year-old manual laborer presents with chronic shoulder pain, profound weakness in external rotation, and a positive hornblower's sign. MRI demonstrates a massive, retracted, and irreparable tear of the supraspinatus and infraspinatus with Goutallier stage 4 fatty infiltration. The subscapularis is intact, and there is no glenohumeral arthritis. Which of the following is the most appropriate tendon transfer to restore active external rotation?
Explanation
Question 38
A 35-year-old man falls from a height and sustains a traumatic elbow dislocation. After closed reduction, radiographs reveal a displaced radial head fracture, a small type 1 coronoid tip fracture, and a lateral collateral ligament (LCL) tear. He is scheduled for operative fixation. What is the standard and most appropriate sequence of surgical repair for this 'terrible triad' injury?
Explanation
Question 39
A 72-year-old woman with a history of osteoporosis sustains a severely comminuted 4-part proximal humerus fracture. A reverse total shoulder arthroplasty (RTSA) is planned. To optimize outcomes and restore appropriate deltoid tension, which of the following landmarks is most critical for determining the correct height of the humeral prosthesis?
Explanation
Question 40
A 24-year-old man presents with chronic wrist pain 8 months after a fall. Radiographs show a scaphoid proximal pole fracture nonunion. MRI demonstrates low T1 and T2 signal intensity throughout the proximal pole, indicating avascular necrosis (AVN). There is no radioscaphoid arthritis. Which of the following is the most appropriate surgical treatment?
Explanation
Question 41
A 50-year-old manual worker presents with dorsal wrist pain and decreased range of motion. Radiographs demonstrate advanced narrowing of the radioscaphoid joint and midcarpal (capitolunate) joint, while the radiolunate joint is perfectly preserved. Which of the following procedures is strictly contraindicated in this patient?
Explanation
Question 42
A 42-year-old bodybuilder feels a 'pop' in his anterior elbow while lifting a heavy object, presenting with an abnormal contour of the biceps muscle belly and weakness in supination. He undergoes a 2-incision surgical repair of the distal biceps tendon. Which of the following complications is most specifically associated with the 2-incision technique compared to a single anterior incision technique?
Explanation
Question 43
A 21-year-old collegiate rugby player is undergoing a Latarjet procedure for recurrent anterior shoulder instability. The coracoid process is osteotomized and transferred to the anterior glenoid neck. Which of the following structures creates the 'sling effect' that provides dynamic stability in this procedure?
Explanation
Question 44
A 32-year-old carpenter presents with insidious onset of dorsal wrist pain. Radiographs demonstrate sclerosis and fragmentation of the lunate, but carpal height is maintained, and there is no fixed scaphoid rotation. The patient has negative ulnar variance. Which of the following surgical interventions is most appropriate?
Explanation
Question 45
A 19-year-old pitcher presents with medial elbow pain during the late cocking phase of throwing. MRI arthrogram shows a partial tear of the ulnar collateral ligament (UCL) anterior bundle. After failing nonoperative management, he undergoes surgical reconstruction. What is the precise anatomical insertion site for the graft on the ulna during a standard UCL reconstruction?
Explanation
Question 46
A 45-year-old heavy laborer undergoes a single-incision anterior approach for the repair of a retracted acute distal biceps tendon rupture. Two weeks postoperatively, he complains of numbness over the lateral aspect of his forearm. His motor function in the hand and wrist is completely intact. Which of the following structures was most likely injured during the procedure?
Explanation
Question 47
A 38-year-old woman falls on an outstretched hand and sustains a 'terrible triad' injury to her right elbow. Which of the following represents the most appropriate sequence of surgical reconstruction to effectively restore joint stability?
Explanation
Question 48
A 28-year-old male falls from a height and sustains a highly comminuted radial head fracture, diffuse forearm tenderness, and distal radioulnar joint (DRUJ) instability, consistent with an Essex-Lopresti injury. He undergoes prompt radial head replacement to restore length. Intraoperatively, following the radial head replacement, the DRUJ remains grossly unstable in neutral rotation. What is the next best step in management?
Explanation
Question 49
A 45-year-old male presents with chronic, progressive wrist pain. Radiographs reveal a scaphoid nonunion with advanced radioscaphoid arthritis and capitolunate arthritis. The radiolunate joint is well-preserved. This is consistent with a Stage III Scaphoid Nonunion Advanced Collapse (SNAC). Which of the following is the most appropriate motion-preserving surgical treatment?
Explanation
Question 50
A 29-year-old elite volleyball player presents with insidious onset of posterior right shoulder pain and weakness. On physical examination, there is noticeable atrophy of the infraspinatus muscle fossa, but the bulk of the supraspinatus is normal. She demonstrates significant weakness in external rotation, while her abduction strength is fully preserved. Which of the following is the most likely anatomic location of the nerve compression?
Explanation
Question 51
A 72-year-old right-hand-dominant woman sustains a 4-part proximal humerus fracture after a ground-level fall. Radiographs show a valgus impacted fracture pattern with disruption of the medial hinge and 1.5 cm of medial translation of the humeral shaft. She has pre-existing advanced glenohumeral osteoarthritis and a documented massive, irreparable rotator cuff tear. What is the most reliable surgical option for pain relief and functional restoration in this patient?
Explanation
Question 52
A 22-year-old collegiate baseball pitcher presents with vague posterior shoulder pain during the late cocking and early acceleration phases of throwing. Examination reveals a 25-degree Glenohumeral Internal Rotation Deficit (GIRD) compared to the non-throwing shoulder, and positive apprehension. MRI arthrography demonstrates a posterosuperior labral tear and a partial articular-sided supraspinatus tendon avulsion (PASTA) lesion. Which of the following pathophysiologic mechanisms is most directly responsible for this specific cascade of pathology?
Explanation
Question 53
A 31-year-old male bodybuilder feels a sudden, painful 'pop' in his anterior chest while performing a heavy bench press. He presents with extensive ecchymosis over the anterior axilla, swelling, and a loss of the normal anterior axillary fold contour. Examination reveals severe weakness in adduction and internal rotation of the humerus. Which of the following anatomical locations is the most common site of rupture for this injury?
Explanation
Question 54
A 25-year-old man complains of persistent dorsal wrist pain and a clicking sensation 3 months after falling on an extended, ulnar-deviated wrist. Physical examination reveals focal tenderness over the dorsal scapholunate interval and a positive Watson scaphoid shift test. Radiographs show a scapholunate gap of 4 mm and a cortical 'ring sign' of the scaphoid. The radiolunate angle measures 20 degrees of dorsal tilt. Based on these radiographic findings, what carpal instability pattern has developed?
Explanation
Question 55
A 40-year-old carpenter presents with 6 months of persistent numbness in his small and ring fingers, and subjective clumsiness in his right hand. Examination shows a positive Tinel's sign at the cubital tunnel, weak pinch strength, and a positive Froment's sign. Electrodiagnostic studies confirm severe ulnar neuropathy at the elbow with active denervation in the first dorsal interosseous muscle. Notably, his right elbow demonstrates a 15-degree cubitus valgus deformity from a malunited pediatric supracondylar fracture. What is the most appropriate surgical intervention?
Explanation
Question 56
A 40-year-old patient undergoes surgical management for a 'terrible triad' injury of the elbow. A lateral approach is utilized. The coronoid fracture (Type 1) is repaired with a capsule suture lasso, the comminuted radial head is replaced, and the lateral ulnar collateral ligament (LUCL) is repaired to the lateral epicondyle. Following these steps, fluoroscopic evaluation reveals that the elbow remains persistently unstable and subluxates symmetrically at 45 degrees of flexion. What is the most appropriate next step in management?
Explanation
Question 57
A 65-year-old woman with a long-standing history of rheumatoid arthritis sustains a severe intra-articular, comminuted distal humerus fracture (AO/OTA 13-C3). Radiographs demonstrate severe osteopenia and preexisting radiocapitellar joint space narrowing. Which of the following is the most appropriate surgical treatment?
Explanation
Question 58
A 25-year-old man presents with chronic wrist pain 1 year after falling on an outstretched hand. Imaging reveals a scaphoid nonunion with a humpback deformity and avascular necrosis (AVN) of the proximal pole. There is no significant radiocarpal arthritis. Which of the following vascularized bone grafts is most appropriate for addressing this specific injury?
Explanation
Question 59
A 30-year-old man sustains a hyperextension wrist injury, resulting in a volar perilunate dislocation. During surgical reconstruction via a combined dorsal and volar approach, which of the following ligaments must be repaired to restore the primary stabilizer of the proximal carpal row and prevent a dorsal intercalated segment instability (DISI) deformity?
Explanation
Question 60
A 19-year-old male is brought to the emergency department after a high-impact rugby tackle. He complains of shortness of breath, dysphagia, and severe pain over his medial clavicle. Physical examination reveals a palpable depression over the medial aspect of the affected clavicle. After ensuring a stable airway, what is the most appropriate next step in management?
Explanation
Question 61
A 72-year-old right-hand-dominant woman sustains a 4-part proximal humerus fracture. Her medical history includes severe rotator cuff arthropathy with a massive, irreparable rotator cuff tear diagnosed prior to the injury. Which of the following is the most appropriate surgical treatment?
Explanation
Question 62
A 6-year-old boy sustains a Bado Type I Monteggia fracture-dislocation. Radiographs show a plastic deformation of the ulna and an anterior dislocation of the radial head. During closed reduction, the radial head reduces when the forearm is supinated and the elbow is flexed, but it repeatedly subluxates upon pronation. What is the most critical step to ensure stable maintenance of the radial head reduction?
Explanation
Question 63
A 45-year-old avid cyclist complains of numbness and tingling in his right ring and small fingers, along with weakness in gripping. Examination reveals clawing of the small and ring fingers, a positive Froment's sign, but normal sensation over the dorso-ulnar aspect of the hand. Where is the most likely site of ulnar nerve compression?
Explanation
Question 64
A 55-year-old manual laborer presents with progressive wrist pain and stiffness. Radiographs show severe joint space narrowing between the scaphoid and the radial styloid, as well as between the lunate and capitate. The radiolunate joint space is completely preserved. This radiographic appearance is most consistent with which stage of Scapholunate Advanced Collapse (SLAC)?
Explanation
Question 65
A 40-year-old weightlifter feels a 'pop' in his anterior elbow during a heavy deadlift, followed by ecchymosis and weakness in forearm supination. He undergoes surgical repair of a distal biceps tendon rupture using a single-incision anterior approach. Postoperatively, he reports isolated numbness over the lateral aspect of his forearm. Which of the following nerves was most likely injured during the surgical exposure?
Explanation
Question 66
A 65-year-old woman presents to the emergency department after falling on an outstretched hand. Radiographs demonstrate a displaced volar shear fracture of the distal radius (volar Barton's fracture).
Which of the following is the most appropriate surgical approach and fixation strategy to prevent displacement?

Explanation
Question 67
A 40-year-old man sustains a terrible triad injury to his left elbow following a fall from a height. Intraoperatively, through a lateral approach, the radial head is replaced and the coronoid fracture is anatomically fixed. However, during range of motion testing, the elbow tends to subluxate posteriorly when brought into extension. Which of the following structures must be addressed next to restore stability?
Explanation
Question 68
A 45-year-old construction worker presents with chronic wrist pain and limited range of motion. Radiographs demonstrate a long-standing scaphoid nonunion with arthritic changes at the radioscaphoid and capitolunate joints, while the radiolunate articulation remains preserved.
What is the most appropriate definitive surgical management?
Explanation
Question 69
A 68-year-old osteoporotic woman undergoes open reduction and internal fixation with a locking plate for a displaced 3-part proximal humerus fracture.
Postoperatively, what technical error during fixation most significantly increases her risk of varus collapse and subsequent superior screw cutout?

Explanation
Question 70
A 50-year-old man presents with persistent ulnar neuropathy 14 months after undergoing an in situ cubital tunnel release. He reports progressive intrinsic weakness. Dynamic ultrasound reveals the ulnar nerve is encased in thick scar tissue and subluxates over the medial epicondyle during elbow flexion. What is the most appropriate surgical intervention?
Explanation
Question 71
A 42-year-old recreational tennis player has persistent, severe anterior shoulder pain. Nonoperative management, including physical therapy and injections, has failed. MRI arthrogram reveals a Type II SLAP tear. Diagnostic arthroscopy confirms a detached superior labrum and an unstable biceps anchor. Based on current orthopedic literature, what is the best management strategy for this patient?
Explanation
Question 72
A 45-year-old man undergoes repair of an acute distal biceps tendon rupture via a single-incision anterior approach.
Postoperatively, he notes a patch of numbness on the radial aspect of his forearm. Which nerve was most likely injured or stretched during the surgical exposure?
Explanation
Question 73
A 28-year-old carpenter presents with worsening dorsal wrist pain. Radiographs demonstrate sclerosis and early fragmentation of the lunate, without carpal collapse. Ulnar variance is measured at -3 mm. What is the most appropriate surgical treatment to halt disease progression?
Explanation
Question 74
A 24-year-old sustains a clean laceration to the volar index finger in Zone II. Surgical exploration reveals >60% laceration of both the FDS and FDP tendons. Following an optimal 4-strand core suture repair with a continuous epitendinous stitch, what is the best postoperative rehabilitation protocol?
Explanation
Question 75
A 72-year-old woman with advanced cuff tear arthropathy and pseudoparalysis undergoes a reverse total shoulder arthroplasty (RTSA).
To minimize the risk of inferior scapular notching postoperatively, how should the glenoid baseplate and glenosphere be positioned?

Explanation
Question 76
A 45-year-old man sustains a terrible triad injury to his left elbow after falling from a ladder. He undergoes operative management including radial head replacement, lateral collateral ligament (LCL) repair, and coronoid fracture fixation. Postoperatively, he is engaged in a supervised rehabilitation protocol. What is the most common complication this patient is likely to experience following surgical management of this injury?
Explanation
Question 77
A 42-year-old right-hand-dominant carpenter presents with chronic wrist pain 6 years after an untreated fall on his outstretched hand. Radiographs reveal a scaphoid nonunion with arthritic changes involving the radioscaphoid joint and the capitolunate joint. The radiolunate articulation is entirely spared. Based on this Scaphoid Nonunion Advanced Collapse (SNAC) pattern, which of the following is the most appropriate surgical intervention?
Explanation
Question 78
A 72-year-old woman with a massive, irreparable rotator cuff tear and pseudoparalysis is scheduled to undergo a reverse total shoulder arthroplasty (RTSA). Scapular notching is a well-documented complication of this procedure. Which of the following surgical modifications or implant design choices is most effective in decreasing the incidence of scapular notching?
Explanation
Question 79
A 65-year-old woman sustains a severely displaced 4-part proximal humerus fracture after a motor vehicle collision. A standard AP radiograph
is reviewed. According to the Hertel criteria, which of the following radiographic findings is the most accurate predictor of humeral head ischemia?

Explanation
Question 80
A 48-year-old man presents with severe recurrence of right ulnar neuropathy symptoms 18 months after an in situ ulnar nerve decompression at the cubital tunnel. Electrodiagnostic studies confirm a conduction block at the elbow. Intraoperatively, the ulnar nerve is found to be encased in thick perineural scar tissue within the postcondylar groove. What is the most appropriate management for this revision procedure?
Explanation
Question 81
A 28-year-old male athlete presents with dorsal wrist pain 3 weeks after falling on a hyperextended wrist. Imaging confirms an isolated, complete rupture of the scapholunate interosseous ligament (SLIL). Anatomically, which component of the SLIL is the thickest, strongest, and acts as the primary restraint to palmar flexion of the scaphoid?
Explanation
Question 82
A 14-year-old elite gymnast presents with lateral elbow pain and catching that worsens during weight-bearing activities. Radiographs demonstrate a radiolucent defect in the capitellum. An MRI is obtained. Which of the following MRI findings is an absolute indication for surgical intervention rather than nonoperative management?
Explanation
Question 83
A 55-year-old woman was treated nonoperatively in a short-arm cast for a nondisplaced distal radius fracture. Eight weeks post-injury, she returns to the clinic reporting a sudden inability to actively lift her thumb off a flat table. Physical examination demonstrates intact IP joint flexion but absent active IP joint extension of the thumb. Which of the following is the most appropriate surgical treatment?
Explanation
Question 84
A 30-year-old rock climber presents with acute pain and swelling at the volar base of his right ring finger after hearing a 'pop' while using a crimp grip. Ultrasound confirms bowstringing of the flexor tendons over the proximal phalanx. Which pulley has been ruptured, and what is its precise anatomical origin?
Explanation
Question 85
A 40-year-old avid cyclist presents with intrinsic muscle weakness in his right hand. He reports numbness on the volar aspect of his small finger and the ulnar half of his ring finger. Sensation on the dorsum of his right hand is completely normal. Tinel's sign is positive at the wrist but negative at the cubital tunnel. Compression of the ulnar nerve is most likely occurring at which anatomical location?
Explanation
Question 86
A 28-year-old man presents with chronic radial-sided wrist pain 18 months after a fall onto an outstretched hand. Radiographs reveal a scaphoid proximal pole nonunion with a humpback deformity, but no evidence of radiocarpal arthritis. An MRI confirms avascular necrosis (AVN) of the proximal pole. Which of the following is the most appropriate surgical treatment?
Explanation
Question 87
A 22-year-old collegiate rugby player presents with recurrent anterior shoulder instability. He has had four anterior dislocations over the past season. A 3D-CT scan reveals 25% anterior glenoid bone loss, and MRI shows an engaging Hill-Sachs lesion. What is the most appropriate surgical management?
Explanation
Question 88
Scapular notching is a well-recognized complication following reverse total shoulder arthroplasty (RTSA). Which of the following technical adjustments regarding glenosphere positioning most effectively minimizes the risk of inferior scapular notching?
Explanation
Question 89
A 42-year-old woman sustains a 'terrible triad' injury of the elbow (elbow dislocation, radial head fracture, and coronoid fracture).
Following an initial closed reduction in the emergency department, the elbow remains persistently unstable in extension. During operative management, what is the generally recommended sequence of reconstruction to restore elbow stability?
Explanation
Question 90
A 38-year-old male weightlifter undergoes surgical repair of a complete distal biceps tendon rupture via a single-incision anterior approach. Postoperatively, he complains of numbness and tingling over the anterolateral aspect of his forearm. Motor function of the hand and wrist is completely intact. Which nerve is most likely injured, and what is its anatomic relationship to the biceps tendon?
Explanation
Question 91
A 27-year-old professional volleyball player presents with an insidious onset of right shoulder pain and weakness. Physical examination reveals isolated atrophy of the infraspinatus with profound weakness in external rotation, while abduction strength is completely normal. MRI of the shoulder is most likely to show a paralabral cyst in which of the following locations, and what labral pathology is typically associated with this finding?
Explanation
Question 92
A 32-year-old male competitive weightlifter felt a sudden 'pop' in his anterior chest wall while performing a heavy bench press. Examination reveals loss of the normal anterior axillary fold contour and weakness with resisted internal rotation and adduction. In a complete rupture of the pectoralis major tendon, which portion of the muscle typically ruptures first, and where does it normally insert anatomically on the humerus?
Explanation
Question 93
An 18-year-old male is brought to the emergency department after a high-speed motor vehicle collision. He complains of severe chest pain, shortness of breath, and difficulty swallowing. Physical examination reveals a palpable depression at the right medial clavicle. A CT scan of the chest confirms a posterior sternoclavicular dislocation. What is the most appropriate next step in management?
Explanation
Question 94
A 62-year-old woman sustained a nondisplaced distal radius fracture treated nonoperatively with a short arm cast for 6 weeks. Two weeks after cast removal, she reports a sudden, painless inability to actively extend her thumb interphalangeal joint. Radiographs confirm a healed distal radius fracture in anatomic alignment. Which of the following is the most appropriate surgical treatment for this specific complication?
Explanation
Question 95
A 21-year-old rugby player sustained an injury to his right ring finger when he grasped an opponent's jersey. Physical examination reveals an inability to actively flex the distal interphalangeal (DIP) joint. A lateral radiograph demonstrates a small bony avulsion fragment located volar to the proximal interphalangeal (PIP) joint. According to the Leddy and Packer classification, what type of injury is this, and what is its blood supply status?
Explanation
Question 96
A 74-year-old right-hand-dominant woman sustains a closed 4-part proximal humerus fracture after a mechanical fall. Her medical history is notable for severe glenohumeral osteoarthritis and a known massive, irreparable rotator cuff tear with preoperative pseudoparalysis. What is the most appropriate surgical management?
Explanation
Question 97
Six months after undergoing volar locking plate fixation for a distal radius fracture, a 58-year-old woman reports the sudden inability to actively flex the interphalangeal joint of her right thumb. Radiographs confirm that the fracture is fully healed, but the plate is noted to be placed prominent and distal to the watershed line. Which of the following is the most likely cause of her current symptoms?
Explanation
Question 98
A 48-year-old manual laborer presents with chronic right wrist pain. Radiographs reveal advanced degenerative changes at the radioscaphoid and capitolunate articulations, while the radiolunate joint is completely spared. Based on these findings, which of the following surgical interventions is most appropriate?
Explanation
Question 99
A 35-year-old man falls from a height and sustains a 'terrible triad' injury of the elbow. During surgical reconstruction, the surgeon successfully fixes the coronoid fracture and replaces the highly comminuted radial head. However, the elbow remains persistently unstable in extension and supination. Which of the following is the most critical next step to restore stability?
Explanation
Question 100
A 42-year-old bodybuilder undergoes a single-incision anterior approach for the repair of a complete acute distal biceps tendon rupture. In the recovery room, he complains of numbness and tingling along the lateral (radial) border of his forearm. Motor function is fully intact. Which nerve was most likely injured or compressed by retractors during the surgical exposure?
Explanation
None
