Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 5)
Key Takeaway
Learn more about Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 5) and how to manage it. Top-rated Orthopedic Upper Extremity 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Upper Extremity 2026 MCQs: Board Review Questions & Answers (Part 5)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
Question 2
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
Question 3
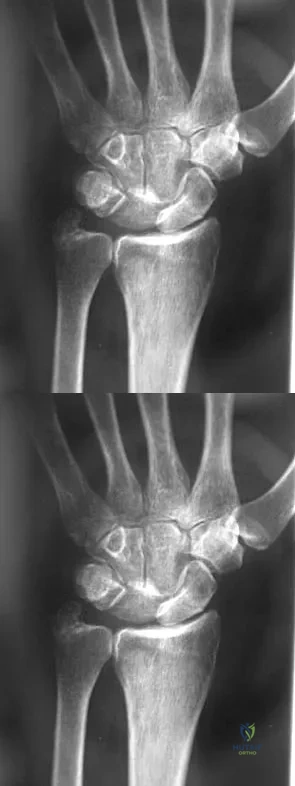
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?
Explanation
Question 4
What is the most common complaint in patients with a developmental radial head dislocation?
Explanation
Question 5
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
Question 6
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Explanation
Question 7
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
Explanation
Question 8
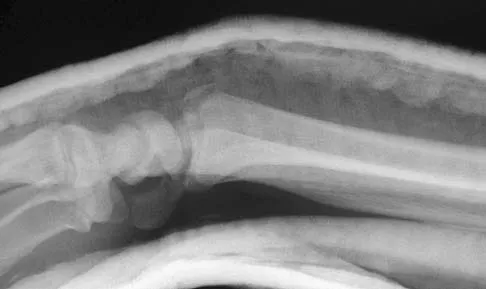
A 35-year-old man sustained the closed injury shown in Figure 52 in his dominant extremity. Neurologic function is normal. Treatment should consist of
Explanation
Question 9
A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?
Explanation
Question 10
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?
Explanation
Question 11
Which of the following antibiotics is contraindicated in children?
Explanation
Question 12
Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
Explanation
Question 13
Figure 55 shows the radiograph of a 30-year-old man who sustained a closed comminuted fracture of the right clavicle. Examination reveals decreased sensation in the radial nerve distribution. Weakness is noted with shoulder abduction, internal rotation, and wrist extension. A displaced bone fragment is most likely pressing on what portion of the brachial plexus?
Explanation
Question 14
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow?
Explanation
Question 15
Which of the following is considered an important component in treating the lesion shown in Figure 56?
Explanation
Question 16
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis?
Explanation
Question 17
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
Question 18
What is the most common complication following interscalene nerve block for shoulder surgery?
Explanation
Question 19
A 61-year-old woman with a long-standing history of rheumatoid arthritis reports progressive elbow pain for the past 12 months. She denies any recent trauma to the elbow; however, she notes increasing pain and decreased joint motion that are now compromising her function. Radiographs are shown in Figures 57a and 57b. What is the most appropriate treatment at this time?
Explanation
Question 20
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal?
Explanation
Question 21
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?
Explanation
Question 22
A 22-year-old college quarterback is tackled and sustains a reducible first carpometacarpal dislocation. What is the recommended treatment?
Explanation
Question 23
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint?
Explanation
Question 24
In a locking plate screw construct, axial forces are borne by which of the following?
Explanation
Question 25
What structure provides the most static stability for valgus restraint in the elbow?
Explanation
Question 26
A 42-year-old man falls on an outstretched hand and sustains a 'terrible triad' injury of the elbow. Surgical fixation is planned. To optimize stability and follow standard surgical principles, what is the most appropriate sequence of repair for the injured structures?
Explanation
Question 27
A 45-year-old male presents with chronic wrist pain. Radiographs demonstrate a scaphoid nonunion advanced collapse (SNAC) pattern with arthritic changes present at the radioscaphoid and capitolunate joints. The radiolunate joint is well preserved. What is the most appropriate definitive surgical treatment?
Explanation
Question 28
A 28-year-old professional volleyball player complains of vague posterior shoulder pain and weakness with overhead serving. Physical examination reveals isolated weakness in external rotation with the arm at the side and noticeable atrophy of the infraspinatus. Supraspinatus strength is normal. An MRI reveals a paralabral cyst. Where is the cyst most likely located?
Explanation
Question 29
A 65-year-old woman sustains a 3-part proximal humerus fracture and is managed non-operatively. At her 6-week follow-up, she demonstrates profound weakness in shoulder abduction and reports decreased sensation over the lateral aspect of her shoulder. Injury to which of the following nerves is most likely responsible for her symptoms?
Explanation
Question 30
A 50-year-old man presents with a 4-month history of numbness in his ring and small fingers, accompanied by weakness in his hand grip. Examination reveals a positive Froment's sign. Which of the following physical examination findings would best differentiate the site of ulnar nerve compression as being at the cubital tunnel rather than Guyon's canal?
Explanation
Question 31
A 40-year-old man undergoes a single-incision anterior approach for a distal biceps tendon repair. Postoperatively, he notes weakness in extending his thumb and fingers. When asked to extend his wrist, his wrist deviates radially. Sensation in the hand and forearm is entirely intact. Which nerve was most likely injured during the procedure?
Explanation
Question 32
A 55-year-old woman is 6 months status post volar locking plate fixation for a comminuted distal radius fracture. She complains of a sudden inability to actively flex the interphalangeal joint of her thumb. Lateral radiographs demonstrate the distal edge of the volar plate is positioned prominently volar to the watershed line. What is the most likely cause of her current presentation?
Explanation
Question 33
A 30-year-old construction worker presents with chronic dorsal wrist pain and stiffness. Radiographs reveal sclerosis and early collapse of the lunate, consistent with Kienböck's disease. Measurement of ulnar variance shows ulnar minus 3 mm. The articular cartilage of the radiocarpal and midcarpal joints appears well-preserved on MRI. Which of the following is the most appropriate initial surgical intervention to decompress the lunate?
Explanation
Question 34
A 22-year-old mountain biker falls over his handlebars and sustains a midshaft clavicle fracture. Which of the following findings is considered an absolute indication for acute open reduction and internal fixation?
Explanation
Question 35
You are discussing the biomechanics of a reverse total shoulder arthroplasty (RTSA) with a resident.
Which of the following best describes the primary biomechanical advantage conferred by the medialized and distalized center of rotation typical of a Grammont-style reverse shoulder implant?
Explanation
Question 36
A 45-year-old manual laborer presents with chronic, progressive radial-sided wrist pain. He has a history of a fall on an outstretched hand 10 years ago. Radiographs demonstrate a scaphoid nonunion with advanced collapse (SNAC). There is significant joint space narrowing and sclerosis at the radioscaphoid and capitolunate joints, but the radiolunate articulation is well preserved. Which of the following is the most appropriate surgical treatment?
Explanation
Question 37
A 38-year-old male weightlifter undergoes repair of a complete distal biceps tendon rupture via a classic two-incision approach. During his postoperative course, what complication is significantly more frequent with this surgical approach compared to a single-incision anterior approach?
Explanation
Question 38
A 22-year-old rugby player with recurrent anterior shoulder instability is scheduled for an open Latarjet procedure (coracoid transfer) after a CT scan demonstrates 28% anterior glenoid bone loss. During the osteotomy of the coracoid and its subsequent transfer through the split in the subscapularis tendon, which of the following nerves is at greatest risk of iatrogenic injury?
Explanation
Question 39
A 65-year-old woman is seen 9 months after undergoing open reduction and internal fixation of a distal radius fracture with a volar locking plate. She reports the sudden onset of an inability to actively flex the interphalangeal joint of her thumb. Passive motion is intact. What is the most likely etiology of this complication?
Explanation
Question 40
A 55-year-old woman falls and sustains a displaced 4-part proximal humerus fracture.
According to Hertel's criteria, which of the following radiographic findings is the most reliable predictor of subsequent avascular necrosis (AVN) of the humeral head?
Explanation
Question 41
A 42-year-old male falls from a height and sustains a 'terrible triad' injury of the elbow, which includes an elbow dislocation, a comminuted radial head fracture, and a Type II coronoid fracture. Operative intervention is planned. To optimize stability, what is the most widely accepted surgical sequence for addressing these lesions?
Explanation
Question 42
A 50-year-old man presents with profound weakness in external rotation and elevation of his right shoulder following a massive, irreparable posterosuperior rotator cuff tear. Examination reveals a positive Hornblower's sign and intact subscapularis function. There is no evidence of glenohumeral arthritis. Which of the following tendon transfers is biomechanically most appropriate to restore external rotation in this patient?
Explanation
Question 43
A 45-year-old carpenter presents with numbness and tingling in the small and ring fingers of his right hand, along with weakness in grip strength. On examination, when asked to hold a piece of paper between his thumb and radial side of his index finger against resistance, the interphalangeal joint of his thumb hyperflexes (positive Froment sign). Which muscle is the patient substituting with to maintain hold of the paper?
Explanation
Question 44
A 32-year-old bodybuilder feels a tearing sensation in his anterior chest wall while bench pressing a heavy weight. Examination reveals loss of the anterior axillary fold and significant ecchymosis. MRI confirms a rupture of the sternocostal head of the pectoralis major muscle. Which of the following describes the anatomic footprint of the sternocostal head at its humeral insertion relative to the clavicular head?
Explanation
Question 45
A 50-year-old woman presents with persistent ulnar-sided wrist pain that worsens with pronation and gripping, 1 year after non-operative management of a distal radius fracture.
Radiographs demonstrate a healed distal radius with 4 mm of radial shortening, resulting in positive ulnar variance. MRI reveals degenerative tearing of the triangular fibrocartilage complex (TFCC) and cystic changes in the lunate. The distal radioulnar joint (DRUJ) is congruous without advanced arthritis. What is the most appropriate definitive surgical management?

Explanation
Question 46
A 45-year-old competitive weightlifter undergoes surgical repair of a distal biceps tendon rupture using a single-incision anterior approach. On his first postoperative visit, he complains of numbness and tingling along the lateral aspect of his forearm. Motor function of the hand and wrist is completely intact. Which of the following anatomical structures was most likely injured or stretched during the surgical exposure?
Explanation
Question 47
A 32-year-old man presents with chronic, progressive wrist pain. Radiographs reveal a scaphoid nonunion advanced collapse (SNAC). Imaging demonstrates moderate degenerative changes at the radioscaphoid joint and the scaphocapitate joint, while the radiolunate articulation is entirely spared. However, there is marked cartilage loss and degenerative cyst formation on the proximal head of the capitate. Which of the following is the most appropriate surgical treatment?
Explanation
Question 48
A 40-year-old man falls from a ladder and sustains a 'terrible triad' injury of the elbow. Intraoperatively, the surgeon fixes the coronoid fracture, replaces the highly comminuted radial head with an arthroplasty, and robustly repairs the lateral collateral ligament (LCL) complex to the lateral epicondyle. Upon testing stability, the elbow remains congruous in flexion but persistently subluxates posteriorly when extended beyond 30 degrees. What is the most appropriate next step in management?
Explanation
Question 49
A 72-year-old woman with pseudoparalysis of the shoulder due to massive rotator cuff tear arthropathy is scheduled for a reverse total shoulder arthroplasty (RTSA). Which of the following best describes the fundamental biomechanical advantage conferred by the implant design of an RTSA compared to an anatomic total shoulder arthroplasty?
Explanation
Question 50
A 6-year-old child sustains a widely displaced, extension-type supracondylar humerus fracture.
On initial presentation in the emergency department, the child's hand is pink and well-perfused, but the radial pulse is non-palpable. The patient is taken to the operating room for closed reduction and percutaneous pinning. Post-reduction, the fracture is anatomically aligned, but the radial pulse remains absent. The hand remains warm and pink, with a capillary refill time of 2 seconds. What is the most appropriate next step?

Explanation
Question 51
An 18-year-old high school football player is driven into the turf directly onto his lateral shoulder. He presents to the emergency department supporting his injured arm across his chest. He reports worsening shortness of breath, mild dysphagia, and a choking sensation.
A CT scan of the chest confirms a posterior sternoclavicular dislocation. What is the most appropriate initial management of this injury?

Explanation
Question 52
A 55-year-old woman sustained a nondisplaced fracture of the distal radius 6 weeks ago, which was managed conservatively in a short-arm cast. Two days after cast removal, she suddenly loses the ability to actively extend the interphalangeal joint of her thumb.
Radiographs show healing of the distal radius fracture with no displacement. What is the gold standard surgical intervention for this complication?

Explanation
Question 53
A 48-year-old male with severe cubital tunnel syndrome is undergoing an anterior transposition of the ulnar nerve. To prevent secondary compression post-transposition, the surgeon must systematically release all potential sites of ulnar nerve entrapment around the elbow. Which of the following structures represents the most proximal potential site of compression for the ulnar nerve in this region?
Explanation
Question 54
A 35-year-old mechanic presents to the emergency department complaining of a severely swollen, throbbing index finger 3 days after sustaining a minor puncture wound with a wire.
You suspect pyogenic flexor tenosynovitis. According to Kanavel's criteria, which of the following is considered the earliest and most sensitive clinical sign of this condition?

Explanation
Question 55
A 30-year-old manual laborer presents with progressive dorsal wrist pain and weakened grip strength over the past 6 months. Radiographs demonstrate increased sclerosis and early collapse of the lunate, without fixed scaphoid rotation or adjacent carpal arthritis. Ulnar variance is measured at -3 mm.
The patient is diagnosed with Lichtman Stage II Kienbock's disease. Which of the following surgical interventions is the most appropriate primary joint leveling procedure to unload the lunate in this patient?

Explanation
Question 56
A 42-year-old male weightlifter feels a sudden pop in his anterior elbow during a heavy deadlift. Clinical examination reveals a positive hook test. He undergoes surgical repair via a single-incision anterior approach. Postoperatively, he complains of numbness and paresthesias over the lateral aspect of his forearm. Which of the following nerves was most likely injured or retracted excessively during the surgical exposure?
Explanation
Question 57
A 28-year-old elite volleyball player complains of vague posterior shoulder pain and weakness in external rotation. Clinical examination reveals isolated atrophy of the infraspinatus muscle, while supraspinatus strength and bulk are normal. An MRI confirms the presence of a paralabral cyst. At which of the following anatomic locations is the nerve compression most likely occurring?
Explanation
Question 58
A 35-year-old man falls from a ladder and sustains an elbow dislocation associated with a radial head fracture and a coronoid fracture. He is taken to the operating room for surgical reconstruction. To optimally restore elbow stability in this 'terrible triad' injury, what is the generally recommended sequence of repair?
Explanation
Question 59
A 72-year-old female with severe, painful rotator cuff arthropathy and pseudoparalysis of the shoulder undergoes a reverse total shoulder arthroplasty (RTSA). Which of the following best describes the fundamental biomechanical alteration provided by this specific prosthesis compared to native shoulder anatomy?
Explanation
Question 60
A 45-year-old manual laborer presents with chronic, progressive wrist pain. He sustained an untreated wrist sprain 10 years ago. Radiographs demonstrate a scaphoid nonunion with advanced arthritic changes at the radioscaphoid and capitolunate joints; however, the radiolunate joint is completely spared.
Which of the following salvage procedures is most appropriate for this patient?

Explanation
Question 61
A 24-year-old female sustains a severe fall onto an outstretched hand. Imaging reveals a coronal shear fracture of the capitellum that extends medially into the lateral trochlear ridge (Type IV capitellar fracture). She is scheduled for open reduction and internal fixation. Which surgical approach provides the most optimal visualization for addressing this specific fracture pattern?
Explanation
Question 62
A 65-year-old woman is 6 weeks status post nonoperative cast management of a minimally displaced distal radius fracture. She suddenly loses the ability to actively extend her thumb interphalangeal joint, though she denies any new trauma. What is the gold standard surgical management for this specific complication?
Explanation
Question 63
A 50-year-old man presents with chronic numbness in his small and ring fingers, accompanied by intrinsic muscle wasting and a positive Froment's sign. Electromyography confirms severe compression of the ulnar nerve at the elbow. During an in situ ulnar nerve decompression, the surgeon must ensure all potential sites of compression are released. Which of the following is the most common anatomical site of ulnar nerve compression in this region?
Explanation
Question 64
A 32-year-old male wrestler sustains a closed, spiral fracture of the distal third of the humeral shaft. On presentation in the emergency department, he is unable to extend his wrist or fingers and has numbness in the first dorsal web space.
According to the American Academy of Orthopaedic Surgeons (AAOS) guidelines, what is the most appropriate initial management for this nerve injury?

Explanation
Question 65
A 28-year-old male powerlifter feels a tearing sensation in his anterior chest wall while performing a heavy bench press. Examination reveals an asymmetric loss of the anterior axillary fold and marked weakness in internal rotation. MRI confirms a complete rupture of the pectoralis major tendon at its humeral insertion. Based on the biomechanics of the bench press exercise, which specific fibers of the pectoralis major are typically under the greatest tension and tear first?
Explanation
Question 66
A 45-year-old man falls from a height and sustains an intra-articular distal radius fracture. CT scan demonstrates a 3-mm displaced, 4-mm wide volar ulnar corner (lunate facet) fragment. He undergoes open reduction and internal fixation with a standard volar locking plate. Two weeks postoperatively, radiographs reveal acute volar subluxation of the carpus. Which of the following is the most likely cause of this complication?
Explanation
Question 67
A 32-year-old woman sustains a 'terrible triad' injury to her right elbow. She is taken to the operating room for surgical stabilization. To optimally restore elbow stability, what is the most widely accepted and biomechanically sound sequence of structural reconstruction?
Explanation
Question 68
A 55-year-old manual laborer presents with chronic wrist pain and weakness. Radiographs reveal a scaphoid nonunion with advanced radioscaphoid arthritis and narrowing of the capitolunate joint space, but the radiolunate joint is preserved. Which of the following is the most appropriate surgical salvage procedure for this patient?
Explanation
Question 69
A 28-year-old carpenter presents with an inability to make an 'OK' sign with his right hand. On examination, his thumb interphalangeal joint and index finger distal interphalangeal joint remain extended when attempting to pinch. He has no sensory deficits. Which of the following anatomical variants is a well-known cause of this specific nerve compression syndrome?
Explanation
Question 70
A 68-year-old woman sustains a 3-part proximal humerus fracture after a fall.
When evaluating the initial trauma radiographs, which of the following findings is the strongest independent predictor for the subsequent development of avascular necrosis (AVN) of the humeral head?
Explanation
Question 71
A 42-year-old recreational weightlifter undergoes a classic two-incision approach (Boyd-Anderson) for a distal biceps tendon rupture repair. Six months postoperatively, he complains of severe stiffness in forearm rotation. Examination reveals a hard block with only 10 degrees of pronation and 15 degrees of supination. Which of the following technical errors during the index procedure is most likely responsible for this complication?
Explanation
Question 72
A 72-year-old man undergoes a reverse total shoulder arthroplasty (rTSA) for massive, irreparable rotator cuff tear arthropathy. Two years later, routine follow-up radiographs reveal grade 3 scapular notching. Which of the following surgical techniques or implant choices would have most likely decreased the incidence of this specific complication?
Explanation
Question 73
A 6-year-old boy presents to the emergency department after falling off playground equipment. Radiographs demonstrate an isolated plastic deformation of the ulnar shaft and an anteriorly dislocated radial head. Which of the following is the most critical step in the initial management to ensure a stable reduction of the radial head?
Explanation
Question 74
A 30-year-old tennis player complains of dorsal, central wrist pain and a subjective 'clunk' 4 weeks after falling on an outstretched hand. Examination reveals tenderness over the dorsal scapholunate interval. Radiographs show a scapholunate gap of 4 mm and a radiolunate angle of 25 degrees. Which of the following is the most appropriate management for this patient?
Explanation
Question 75
A 40-year-old diabetic patient presents with a severely swollen, painful index finger 3 days after sustaining a puncture wound.
Examination reveals the finger is held in slight flexion, uniform volar swelling, exquisite pain on passive extension, and tenderness along the entire flexor tendon sheath. He requires emergent surgical irrigation and debridement. Which of the following annular pulleys MUST be preserved during the surgical approach to prevent postoperative bowstringing of the flexor tendons?

Explanation
Question 76
A 62-year-old man presents to the clinic 4 weeks after an anterior shoulder dislocation that was successfully reduced in the emergency department. He reports persistent weakness in the shoulder, specifically when trying to lift his arm away from his body and externally rotate. Plain radiographs show concentric reduction with no fractures. What is the most appropriate next step in management?
Explanation
Question 77
A 45-year-old woman falls on an outstretched hand and sustains a 'terrible triad' injury of the elbow. She undergoes operative management. During the procedure, the surgeon decides to repair the lateral ulnar collateral ligament (LUCL) to the lateral epicondyle using a suture anchor. Where is the precise isometric origin of the LUCL on the lateral epicondyle?
Explanation
Question 78
A 28-year-old laborer presents with chronic wrist pain and is diagnosed with a scaphoid nonunion with a humpback deformity and early radiocarpal arthrosis limited to the radial styloid (SNAC stage I). He has minimal symptoms at rest but pain with heavy gripping. Which of the following is the most appropriate surgical treatment?
Explanation
Question 79
A 70-year-old woman undergoes reverse total shoulder arthroplasty (RTSA) for massive cuff tear arthropathy. Postoperatively, she has active forward elevation to 135 degrees but reports difficulty eating, drinking, and washing her opposite shoulder. Examination reveals a positive hornblower's sign. Which of the following muscles is most likely deficient and responsible for her functional limitations?
Explanation
Question 80
A 32-year-old woman sustains a coronal shear fracture of the distal humerus extending medially to include the lateral aspect of the trochlea (McKee modification of Bryan and Morrey Type IV). She is scheduled for open reduction and internal fixation. Which of the following structures is most commonly injured with this fracture pattern and must be carefully evaluated for repair during surgery?
Explanation
Question 81
A 24-year-old professional tennis player complains of ulnar-sided wrist pain worsening with forearm rotation and ulnar deviation. MRI reveals a peripheral tear of the triangular fibrocartilage complex (TFCC) at its foveal attachment. Nonoperative management has failed. During arthroscopic repair, which of the following is the most appropriate technique for a Palmer Class 1B tear?
Explanation
Question 82
A 29-year-old female presents with right shoulder pain and weakness after a prolonged backpacking trip. On examination, medial winging of the scapula is prominent when she performs a wall push-up. EMG confirms a severe, isolated long thoracic nerve injury. After 15 months of physical therapy and observation, there is no clinical or electromyographic improvement. Which of the following tendon transfers is the most appropriate surgical option?
Explanation
Question 83
A 42-year-old male heavy laborer feels a 'pop' in his anterior elbow while lifting a 50-lb box. Clinical examination demonstrates a reverse Popeye deformity and weakness in forearm supination. He undergoes an anatomic single-incision repair of the distal biceps tendon using a cortical button. Which of the following nerve complications is most classically associated with the anterior single-incision approach to the distal biceps?
Explanation
Question 84
A 35-year-old assembly line worker reports a 4-month history of aching pain in the proximal volar forearm and numbness in the thumb, index, and middle fingers. Symptoms worsen with resisted forearm pronation and elbow flexion, but not with prolonged wrist flexion. Electrodiagnostic studies of the median nerve at the wrist are normal. Which of the following physical exam findings best differentiates this condition from Carpal Tunnel Syndrome?
Explanation
Question 85
A 55-year-old man falls while skiing, forcibly externally rotating his right arm. He exhibits increased passive external rotation and tests positive on the belly-press test. MRI confirms an isolated, full-thickness tear of the subscapularis tendon with medial retraction. During arthroscopic repair, which anatomic landmark is most reliable for identifying the superior border of the retracted subscapularis tendon?
Explanation
Question 86
A 72-year-old woman with pseudoparalysis of the shoulder secondary to a massive, irreparable rotator cuff tear undergoes a reverse total shoulder arthroplasty. How does this specific implant design alter the biomechanics of the shoulder joint to restore active elevation?
Explanation
Question 87
A 45-year-old man falls on an outstretched hand and sustains a 'terrible triad' injury of the elbow. Imaging confirms a posterior elbow dislocation, a comminuted radial head fracture, and a Regan-Morrey Type 2 coronoid fracture. During surgical reconstruction, after addressing the radial head and repairing the anterior capsule/coronoid, the elbow remains unstable to varus stress and tends to subluxate posterolaterally. Which of the following structures must be repaired next to restore stability?
Explanation
Question 88
A 55-year-old woman undergoes volar locked plating for a displaced intra-articular distal radius fracture. Six months postoperatively, she presents to the clinic with a sudden inability to actively flex the interphalangeal joint of her thumb. She reports no new trauma. Which of the following technical errors during the index procedure is the most likely cause of this complication?
Explanation
Question 89
A 38-year-old weightlifter undergoes an anatomic repair of a distal biceps tendon rupture via a single-incision anterior approach. Postoperatively, he notes numbness and paresthesias along the radial and volar aspect of his forearm. Which of the following nerves was most likely injured or subjected to excessive traction during the surgical approach?
Explanation
Question 90
A 28-year-old manual laborer presents with chronic dorsal wrist pain. Radiographs reveal sclerosis and collapse of the lunate with a fixed flexion deformity of the scaphoid (radioscaphoid angle of 65 degrees) and proximal migration of the capitate. Ulnar variance is neutral. Based on the Lichtman classification, what is the most appropriate definitive surgical intervention?
Explanation
Question 91
A 75-year-old active woman sustains a 4-part proximal humerus fracture. Because of the risk of avascular necrosis and severe comminution, she undergoes a shoulder hemiarthroplasty. What is the most critical prognostic factor determining the long-term functional outcome of active forward elevation in this patient?
Explanation
Question 92
A 32-year-old skier falls and sustains a forced hyperabduction injury to his right thumb. Clinical examination reveals 40 degrees of radial deviation laxity at the metacarpophalangeal (MCP) joint with no distinct endpoint. A discrete, tender mass is palpable just proximal to the MCP joint. Which of the following structures is interposed, preventing anatomic healing of the injured ligament and necessitating surgical repair?
Explanation
Question 93
A 24-year-old male presents with radial-sided wrist pain after a fall. Initial radiographs are negative, but an MRI demonstrates a nondisplaced fracture of the proximal pole of the scaphoid. The patient is at high risk for avascular necrosis due to the unique vascular anatomy of the scaphoid. The predominant blood supply to the proximal pole enters through which of the following regions?
Explanation
Question 94
A 6-year-old boy presents with a completely displaced, extension-type supracondylar humerus fracture (Gartland Type III). On initial examination, the hand is pink but the radial pulse is non-palpable. The patient is taken emergently to the operating room. After closed reduction and percutaneous pinning, the fracture is anatomically aligned. The hand remains pink with brisk capillary refill, but the radial pulse remains absent. What is the most appropriate next step in management?

Explanation
Question 95
A 25-year-old carpenter sustains a volar laceration to his index finger at the level of the proximal phalanx, transecting both the FDS and FDP tendons (Zone II). During the primary surgical repair, optimizing flexor tendon gliding and preventing bowstringing is paramount. Preserving or reconstructing which of the following annular pulley combinations is most critical to ensure maximal biomechanical efficiency of the digit?
Explanation
Question 96
A 55-year-old woman presents with the inability to actively flex the interphalangeal joint of her right thumb. She underwent open reduction and internal fixation of a distal radius fracture with a volar locking plate 8 months ago. Radiographs reveal that the plate is positioned distal to the watershed line of the distal radius. What is the most likely etiology of her current deficit?
Explanation
Question 97
A 40-year-old man falls from a ladder and sustains an elbow injury. Imaging reveals a posterior elbow dislocation, a comminuted radial head fracture, and a type II coronoid fracture. The patient is taken to the operating room for surgical stabilization. What is the generally recommended sequence of reconstruction for this specific pattern of injury?
Explanation
Question 98
A 35-year-old male presents with chronic wrist pain and weakness, noting he sustained a 'sprain' during a football game 5 years ago that was never formally evaluated. Radiographs reveal a scaphoid waist nonunion with advanced degenerative changes at the radioscaphoid and capitolunate joints. The radiolunate articulation is well-preserved. Which of the following is the most appropriate surgical treatment?
Explanation
Question 99
A 78-year-old right-hand-dominant woman sustains a closed right proximal humerus fracture after a mechanical fall. Radiographs demonstrate a 4-part fracture pattern with a head-split component, severe comminution of the tuberosities, and significant osteopenia. She lives independently but leads a sedentary lifestyle. What is the most appropriate surgical management to provide the most predictable pain relief and restoration of forward elevation?
Explanation
Question 100
During surgical decompression and anterior transposition of the ulnar nerve for severe cubital tunnel syndrome, the surgeon meticulously releases all potential sites of compression. From proximal to distal, which of the following structures represents the most proximal potential site of ulnar nerve compression in the arm?
Explanation
None
