Mastering Volar Plating for Distal Radius Fractures: An Intraoperative Guide
Key Takeaway
This masterclass provides an exhaustive, real-time guide to volar plating distal radius fractures. Fellows will learn intricate surgical anatomy, meticulous patient positioning, and granular intraoperative steps, from initial incision to final hardware placement. We cover critical neurovascular protection, fracture reduction techniques, and essential pearls for avoiding complications and ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The management of distal radius fractures has undergone a profound paradigm shift over the past two decades, pivoting heavily toward open reduction and internal fixation (ORIF) utilizing volar fixed-angle locking plates. As orthopedic surgeons, we encounter this injury with staggering frequency; it represents approximately one-sixth of all fractures treated in emergency departments. The bimodal epidemiological distribution highlights two distinct patient populations: young patients sustaining high-energy trauma (often resulting in complex, intra-articular shear or comminuted patterns) and the elderly population suffering low-energy falls, where osteoporotic bone dictates the mechanical behavior of the fracture. Understanding the nuances of these injury mechanisms is paramount for selecting the appropriate implant and surgical strategy.
Historically, the surgical armamentarium relied heavily on closed reduction with percutaneous pinning, external fixation, or dorsal plating. However, dorsal plating was notoriously plagued by unacceptably high rates of extensor tendon irritation, tenosynovitis, and delayed rupture due to the intimate relationship between the dorsal cortical surface and the extensor compartments. The advent of the volar locking plate revolutionized our approach. By utilizing the relatively protected volar surface of the radius, covered by the substantial muscle belly of the pronator quadratus, we effectively mitigate tendon attrition while capitalizing on the superior biomechanical properties of a fixed-angle construct. This technique provides robust stability, allowing for early mobilization even in osteoporotic bone, and has consequently become the gold standard for most displaced distal radius fractures.
The biomechanical imperative for anatomic restoration cannot be overstated. The distal radius serves as the primary buttress for the proximal carpus, transmitting a substantial 75% to 80% of the axial load from the hand into the forearm. The remaining 20% to 25% is borne by the distal ulna and the triangular fibrocartilage complex (TFCC). Any significant alteration in the distal radius's anatomy—whether through radial shortening, loss of palmar tilt, or articular incongruity—profoundly disrupts wrist kinematics. Even a 2-millimeter articular step-off dramatically alters contact stresses within the radiocarpal joint, predisposing the patient to accelerated post-traumatic osteoarthritis.
Distal radius fractures are defined by their involvement of the metaphysis, specifically the region within a length of the articular surface equivalent to the widest portion of the entire wrist. We assess these fractures based on several key characteristics: location (volar versus dorsal involvement), articular involvement (articular versus nonarticular, and the extent of articular displacement), reducibility, and inherent stability. Irreducible or unstable fractures—characterized by significant initial displacement, dorsal comminution, or intra-articular extension—necessitate surgical reduction and stable fixation to prevent progressive deformity, restore load-bearing mechanics, and optimize long-term functional outcomes.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, a master surgeon must possess an exhaustive, three-dimensional understanding of the regional anatomy. This is not merely an academic exercise; it directly dictates the surgical approach, the safe zones for dissection, and the vigilance required against iatrogenic injury. The distal forearm is a densely packed anatomic corridor, and navigating it requires precision.
Osteology and Articular Configuration
The osteology of the distal radius is uniquely adapted for multi-planar wrist motion and load transfer. Dorsally, the surface forms the floor of the fibro-osseous extensor tendon compartments. Here, we find Lister's tubercle, a crucial bony landmark that acts as a mechanical pulley for the extensor pollicis longus (EPL) tendon. The dorsal radiocarpal ligament originates from this surface. Critically, the dorsal cortical bone is notably thinner, more porous, and less substantial than its volar counterpart. This anatomical predisposition contributes significantly to the characteristic dorsal-bending fracture patterns (Colles-type) we frequently encounter, where the dorsal cortex undergoes tensile failure and comminution.
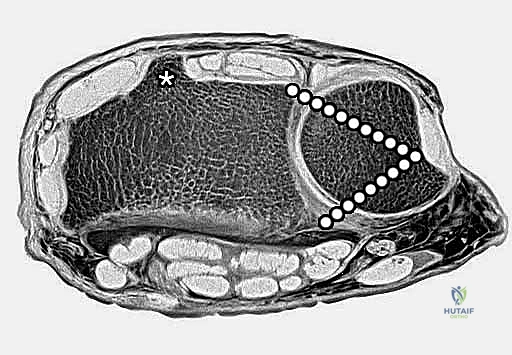
Volarly, the cortical bone is significantly thicker and mechanically stronger, offering a robust platform for plate fixation and buttressing. The volar surface is the origin for critical extrinsic ligaments of the carpus, such as the radioscaphocapitate ligament, which stabilizes the scaphoid and capitate. It also provides the broad origin for the pronator quadratus muscle. Ulnarly, the distal radius gives rise to the radial portion of the triangular fibrocartilage (TFC), a vital component of the TFCC that stabilizes the distal radioulnar joint (DRUJ). The distal radius also contains the sigmoid notch, a shallow concavity that articulates with the head of the distal ulna, facilitating pronation and supination.

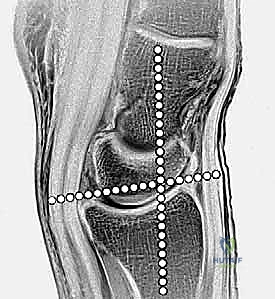
Distally, the articular surface is biconcave and divided by a subtle anteroposterior ridge into two distinct fossae. The lateral, triangularly shaped radioscaphoid fossa articulates with the scaphoid, bearing the brunt of axial loads during radial deviation. The medial, square-shaped radiolunate fossa articulates with the lunate. Accurate restoration of these fossae, particularly the lunate facet which is prone to volar or dorsal die-punch fragmentation, is critical for restoring normal carpal kinematics and preventing midcarpal instability.
Radiographic Parameters and Biomechanics
Restoring the native radiographic angles of the distal radius is the primary metric of surgical success. Radial inclination, measured in the coronal plane, averages 22 degrees (range 21-25 degrees). This inclination represents the angle between a line drawn perpendicular to the longitudinal axis of the radius and a line connecting the tip of the radial styloid to the ulnar corner of the lunate fossa. Loss of radial inclination alters the load-bearing axis, shifting disproportionate stress onto the lunate and the TFCC, which can lead to ulnar-sided wrist pain and restricted radial deviation.

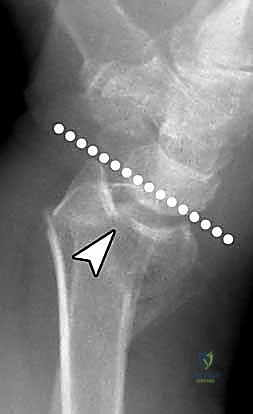
Palmar tilt, or volar tilt, is assessed in the sagittal plane and averages 11 degrees (range 10-12 degrees). It is the angle between a line perpendicular to the radial shaft and a line connecting the dorsal and volar margins of the articular surface. Dorsal angulation, a hallmark of Colles fractures, fundamentally disrupts the congruent articulation between the radius and the carpus. A dorsal tilt exceeding 10 degrees results in a dorsal shift of the carpus, increasing load transmission through the distal ulna and significantly restricting wrist flexion.

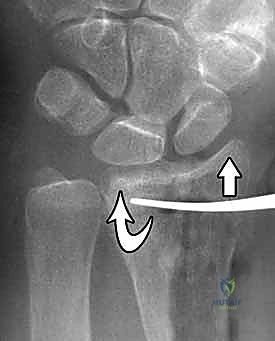
Ulnar variance refers to the relative length of the distal radius compared to the distal ulna. In a healthy wrist, the ulnar aspect of the distal radius (lunate fossa) is usually flush with or slightly distal to the articular surface of the ulnar head, indicating neutral or negative ulnar variance. Fractures often lead to radial shortening, resulting in positive ulnar variance. Even 2 millimeters of radial shortening can increase the axial load transmitted through the ulnocarpal joint from 20% to over 40%, leading to ulnar impaction syndrome and attritional tears of the TFCC.


Neurovascular Topography and Muscular Intervals
The volar approach demands meticulous navigation of critical neurovascular structures. The median nerve lies within the subcutaneous tissues along the ulnar portion of the volar wound, separated from the distal radius by the pronator quadratus and the deep flexor tendons. The palmar cutaneous branch of the median nerve (PCBMN) is particularly vulnerable during the superficial dissection. It typically arises 5 to 7 centimeters proximal to the wrist crease and runs subcutaneously, crossing the flexor carpi radialis (FCR) tendon ulnarly. Surgeons must carefully avoid vigorous radial retraction of the ulnar skin flap within 10 centimeters of the wrist flexion crease to prevent painful neuromas.
The radial artery is the primary arterial supply encountered during the modified Henry approach. It lies radially to the FCR tendon, resting on the flexor pollicis longus (FPL) and the radius. While it is usually not necessary to dissect it out circumferentially, the surgeon must be acutely aware of its course. The palmar carpal branch of the radial artery courses transversely across the distal radius to join the deep palmar arch; this branch often requires careful ligation or cauterization during distal exposure to prevent troublesome bleeding.

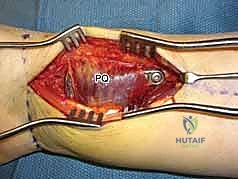
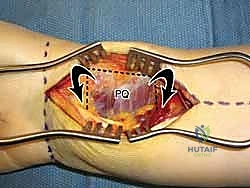
The muscular intervals define our surgical windows. The FCR tendon is the primary landmark for the volar approach. Deep to the FCR, the FPL tendon sits along the radial margin of the deep wound, just ulnar to the FCR interval. The flexor digitorum superficialis (FDS) and profundus (FDP) tendons are deep and ulnar to the FCR, requiring careful ulnar retraction alongside the median nerve. The pronator quadratus (PQ) muscle, a square-shaped muscle covering the volar aspect of the distal radius, represents the final soft-tissue barrier. It must be incised and reflected as an ulnarly based flap to expose the underlying fracture fragments.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention using a volar plate is dictated by a combination of radiographic parameters, fracture morphology, and patient-specific factors. The overarching goal is to prevent post-traumatic arthritis, restore functional range of motion, and return the patient to their pre-injury activity level. While conservative management with closed reduction and casting remains appropriate for truly stable, non-displaced fractures, the threshold for surgery has lowered significantly due to the predictable outcomes of volar plating.
Absolute indications for volar plating include open fractures (requiring concurrent debridement), fractures associated with acute carpal tunnel syndrome or other neurovascular compromise, and irreducible fractures where soft tissue interposition prevents closed alignment. Highly unstable fracture patterns—such as those with marked dorsal comminution, substantial metaphyseal bone loss, or complex intra-articular shear components (Barton's fractures)—are prime candidates. Furthermore, secondary loss of reduction following an initial attempt at conservative casting is a definitive indication for surgical stabilization.
Relative indications encompass a broader spectrum of radiographic criteria that predict poor functional outcomes if left untreated. These include an intra-articular step-off or gap greater than 2 millimeters, radial shortening exceeding 3 millimeters relative to the contralateral wrist, dorsal tilt greater than 10 degrees (or volar tilt >20 degrees), and loss of radial inclination below 15 degrees. Patient factors such as high functional demands, younger age, and the need for early mobilization also heavily influence the decision toward operative fixation.
Contraindications, while relatively few, must be strictly respected. Active local or systemic infection is an absolute contraindication to internal fixation. Relative contraindications include severe, medically unoptimized comorbidities that preclude safe anesthesia, and extremely low-demand, non-ambulatory patients where the surgical risks outweigh the functional benefits. Additionally, pure dorsal shear fractures with small, highly comminuted dorsal articular fragments may sometimes be better served by dorsal fragment-specific fixation or spanning external fixation if a volar plate cannot adequately capture and buttress the dorsal rim.
| Parameter | Operative Indication Threshold | Rationale for Fixation |
|---|---|---|
| Intra-articular Step-off | > 2 mm | Prevents rapid onset of radiocarpal post-traumatic osteoarthritis. |
| Radial Shortening | > 3 mm | Prevents positive ulnar variance, DRUJ incongruity, and ulnar impaction syndrome. |
| Dorsal Angulation | > 10 degrees | Restores normal load transmission and prevents loss of wrist flexion. |
| Radial Inclination | < 15 degrees | Preserves grip strength and normal radiocarpal kinematics. |
| Associated Injuries | Acute CTS, Open Fracture | Requires immediate decompression, debridement, and rigid stabilization. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the foundation of a successful surgical outcome. The process begins with high-quality orthogonal radiographs (posteroanterior, lateral, and oblique views). However, plain films frequently underestimate the degree of intra-articular comminution. For any fracture involving the radiocarpal or distal radioulnar joint, a non-contrast computed tomography (CT) scan with 2D and 3D reconstructions is strongly recommended. CT imaging provides unparalleled visualization of articular step-offs, die-punch fragments, and the precise location of major fracture lines, fundamentally altering the surgical strategy in up to 30% of cases.

Digital templating is an essential step that should not be bypassed. Utilizing the contralateral, uninjured wrist as a template (when available), the surgeon can accurately estimate the required plate length, the optimal positioning of the plate relative to the watershed line, and the expected trajectory of the subchondral locking screws. Templating also aids in anticipating the need for supplemental bone grafting or bone void fillers in cases of severe metaphyseal comminution where structural support is compromised.

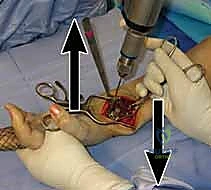
Patient positioning and operating room setup must be optimized for seamless fluoroscopic access and surgical ergonomics. The patient is placed supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The C-arm fluoroscope is typically brought in parallel to the hand table or from the head of the bed, allowing for rapid transition between AP and lateral views without compromising the sterile field.

Prior to incision, the limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated (typically to 250 mmHg or 100 mmHg above systolic pressure). Prophylactic intravenous antibiotics are administered within one hour of incision. The surgeon must ensure that all necessary equipment, including a variety of volar plate designs (variable angle, fixed angle, narrow, standard, and wide), reduction forceps, K-wires, and appropriate screw sets, are readily available on the back table.
Step-by-Step Surgical Approach and Fixation Technique
The execution of volar plating requires a systematic, stepwise approach, balancing adequate exposure for anatomic reduction with the preservation of critical soft tissue envelopes.
The Modified Henry Approach
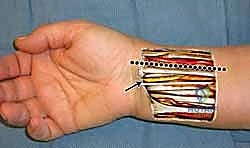
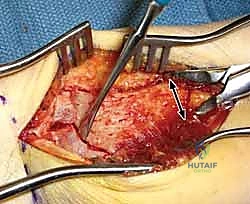
The procedure begins with a longitudinal incision, approximately 8 to 10 centimeters in length, centered over the course of the flexor carpi radialis (FCR) tendon. The incision extends from the wrist flexion crease proximally. Careful subcutaneous dissection is performed to identify and protect the superficial veins and the palmar cutaneous branch of the median nerve, which lies ulnar to the FCR.
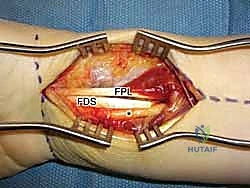
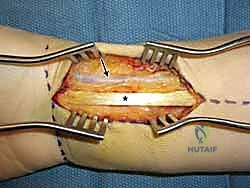
The superficial fascia over the FCR is incised, and the tendon is retracted ulnarly. This exposes the deep fascial floor of the FCR sheath. Incising this deep sheath is the key to entering the intermediate compartment of the forearm safely. Once the deep sheath is opened, the flexor pollicis longus (FPL) tendon is identified radially, and the flexor digitorum superficialis (FDS) tendons and median nerve are identified ulnarly.

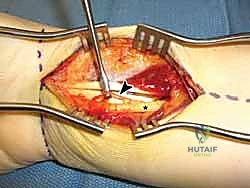
A blunt retractor (such as a Senn or small right-angle retractor) is placed to retract the FPL radially and the FDS/median nerve complex ulnarly. This maneuver directly exposes the pronator quadratus muscle and the volar aspect of the distal radius. The radial artery, situated lateral to the FCR, is protected within the radial soft tissue flap. Care must be taken to identify and cauterize the transverse palmar carpal branch of the radial artery to prevent postoperative hematoma.

Pronator Quadratus Elevation and Fracture Exposure
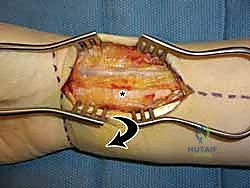
With the pronator quadratus (PQ) completely visualized, an L-shaped incision is made along its radial and distal borders. The radial incision is made just medial to the insertion of the brachioradialis, and the distal incision is made parallel to the joint line, preserving a 2- to 3-millimeter cuff of muscle and fascia distally to facilitate later repair. The PQ is then carefully elevated off the volar radius from radial to ulnar using a periosteal elevator.
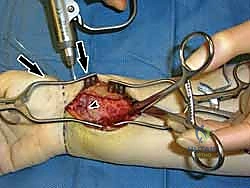
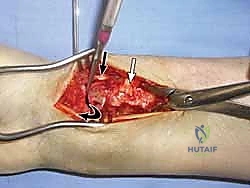
Elevation of the PQ exposes the fracture hematoma and the volar cortical comminution. The fracture site is thoroughly irrigated and debrided of hematoma and interposed soft tissue. At this stage, the brachioradialis tendon, which inserts on the base of the radial styloid, is frequently identified as a major deforming force causing radial shortening and supination of the distal fragment. A step-cut or complete release of the brachioradialis tendon is highly recommended to neutralize these forces and facilitate anatomic reduction.
Fracture Reduction and Provisional Fixation
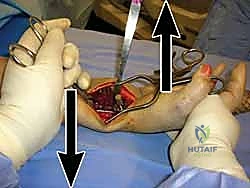
Reduction maneuvers are dictated by the fracture pattern. For typical dorsally displaced fractures, longitudinal traction combined with palmar translation and ulnar deviation of the carpus usually achieves preliminary alignment. Intra-focal pinning (Kapandji technique) can be utilized by inserting a 0.062-inch K-wire into the fracture site dorsally and levering the distal fragment into flexion to restore palmar tilt.

Once satisfactory fluoroscopic reduction is obtained in both AP and lateral planes, provisional fixation is achieved using smooth K-wires. These wires can be placed percutaneously through the radial styloid or directly through the fracture fragments. Alternatively, a volar plate can be applied loosely to the proximal shaft, and the distal fragment can be reduced to the plate using a push-pull screw technique or specialized reduction forceps.

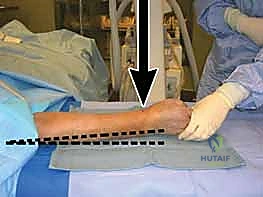
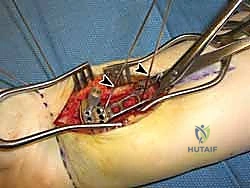
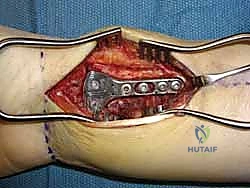
Plate Application and Definitive Fixation
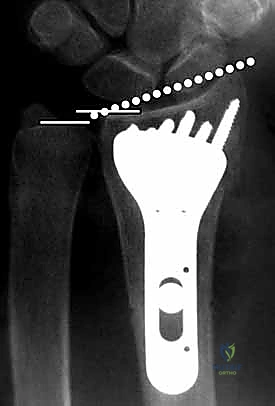
The selection of the volar plate is critical. The plate must be positioned proximal to the "watershed line"—the transverse ridge marking the distal margin of the flat volar surface of the radius. Placing the plate distal to this line significantly increases the risk of flexor tendon irritation and rupture. The plate is initially secured to the intact proximal radial shaft with a single cortical screw in an oblong hole, allowing for proximal-distal micro-adjustments.
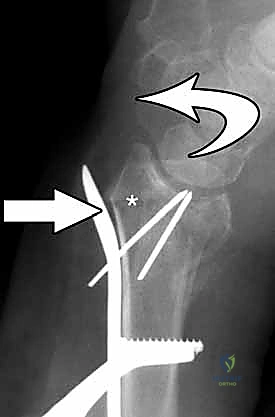
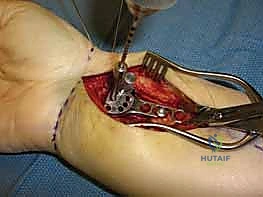
Attention is then turned to the distal articular fragments. Locking drill guides are threaded into the distal holes of the plate. It is imperative that the distal locking screws are placed in a subchondral position (ideally 2-3 millimeters proximal to the articular surface) to provide a structural raft that supports the articular cartilage and prevents late subsidence. Fluoroscopy, particularly the 20-degree elevated lateral view, is utilized to ensure that the screws do not penetrate the radiocarpal joint.

Once the distal locking screws
Clinical & Radiographic Imaging Archive