Volar Osteotomy for Distal Radius Malunion: A Comprehensive Surgical Guide
Key Takeaway
Volar osteotomy is a highly effective surgical intervention for correcting distal radius malunions. By utilizing a volar approach, surgeons can restore anatomic volar tilt, radial inclination, and radioulnar congruity. This procedure involves precise preoperative templating, structural corticocancellous bone grafting, and rigid internal fixation. Successful outcomes depend on meticulous soft tissue handling, accurate restoration of the distal radioulnar joint kinematics, and adherence to structured postoperative rehabilitation protocols.
Comprehensive Introduction and Patho-Epidemiology
Distal radius malunion remains one of the most challenging and complex clinical entities encountered by orthopedic hand and upper extremity surgeons. It is a frequent sequela of the nonoperative management of displaced distal radius fractures, or it arises from the secondary loss of reduction following initial, often inadequate, surgical stabilization. Despite advancements in internal fixation technologies, the sheer volume of distal radius fractures globally ensures that malunion remains a prevalent pathology. The resultant deformity is rarely a simple uniplanar deviation; rather, it is a complex, three-dimensional spatial distortion typically characterized by dorsal tilt in the sagittal plane, loss of radial inclination and radial height in the frontal plane, and a rotational malalignment that manifests as a supination deformity of the radial shaft relative to the pronated distal articular fragment.
The patho-epidemiology of distal radius malunion is deeply intertwined with the initial fracture pattern and the chosen treatment modality. Historically, closed reduction and cast immobilization were the mainstays of treatment for nearly all distal radius fractures. However, predictable patterns of collapse occur in osteopenic bone or highly comminuted fracture patterns, leading to metaphyseal settling. Studies indicate that up to 30% of conservatively managed, initially displaced distal radius fractures will heal with some degree of malunion. Patients typically present with a spectrum of debilitating symptoms, including profound weakness in grip strength, restricted range of motion (particularly in supination and wrist flexion), and chronic, unrelenting ulnar-sided wrist pain. This pain is frequently the primary chief complaint and is driven by secondary ulnocarpal impaction and structural derangement of the distal radioulnar joint (DRUJ).
Historically, dorsal opening wedge osteotomies were utilized to correct these deformities. However, the dorsal approach was fraught with complications, most notably extensor tendon irritation, attritional ruptures, and inadequate soft tissue coverage over bulky hardware. The paradigm has since shifted decisively toward the volar osteotomy, which is now universally recognized as the gold standard surgical intervention. The volar approach exploits the generous soft tissue envelope of the volar wrist, utilizing the pronator quadratus as a dynamic, vascularized buffer between the robust volar locking plates and the flexor tendons.
By executing a meticulously planned volar osteotomy, the surgeon aims to restore the anatomic alignment of the distal radius, thereby re-establishing congruent load transmission across the radiocarpal and midcarpal joints. Furthermore, restoring radial length and volar tilt effectively decompresses the ulnocarpal joint, mitigates the pathological forces acting on the triangular fibrocartilage complex (TFCC), and restores the congruent kinematics of the DRUJ. This comprehensive reconstructive approach not only alleviates pain but predictably restores upper extremity function, allowing patients to return to their pre-injury occupational and recreational activities.
Detailed Surgical Anatomy and Biomechanics
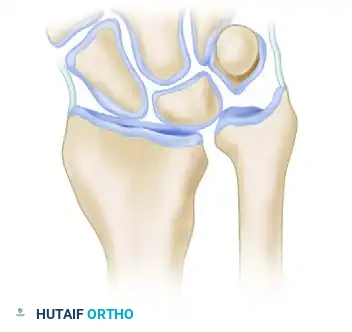
A profound understanding of the surgical anatomy and the intricate biomechanics of the wrist is an absolute prerequisite for executing a successful volar osteotomy. The distal radius is uniquely contoured to facilitate multiplanar wrist motion while simultaneously transmitting immense axial loads from the hand to the forearm. The volar surface of the distal radius is relatively flat and features a thick cortical shell, making it an ideal surface for the application of structural bone grafts and rigid internal fixation. The "watershed line," a critical anatomical landmark, represents the most distal margin of the pronator quadratus fossa. It is a transverse ridge that separates the concave metaphyseal surface from the convex articular surface. Implants placed distal to this line intimately contact the flexor tendons, dramatically increasing the risk of flexor pollicis longus (FPL) and flexor digitorum profundus (FDP) attritional ruptures.
The biomechanical consequences of a distal radius malunion are profound and exponential. In a normal, anatomically aligned wrist, axial load transmission is distributed such that approximately 80% of the force passes through the radiocarpal joint (primarily the scaphoid and lunate fossae) and 20% passes through the ulnocarpal joint via the TFCC. This delicate balance is highly sensitive to changes in sagittal alignment. A dorsal tilt of the distal radius exceeding 20 degrees shifts the center of rotation of the carpus dorsally. This malalignment unloads the volar radiocarpal ligaments and shifts the axial load transmission to an abnormal 50% radius / 50% ulna distribution. This exponential increase in ulnar load is the primary biomechanical driver of ulnar-sided wrist pain, degenerative TFCC tears, and eventual lunotriquetral ligament attenuation.
Furthermore, radial shortening directly compromises the kinematics of the distal radioulnar joint (DRUJ). The sigmoid notch of the radius articulates with the ulnar head, stabilized dynamically by the pronator quadratus and statically by the volar and dorsal radioulnar ligaments of the TFCC. When the radius heals in a shortened and dorsally angulated position, the sigmoid notch translates proximally and dorsally relative to the ulnar head. This creates a severe incongruity, leading to restricted forearm rotation (particularly supination) and painful DRUJ subluxation or dislocation. The interosseous membrane (IOM), specifically the distal oblique bundle (DOB), becomes lax, further destabilizing the longitudinal radioulnar relationship.
The corrective volar osteotomy must therefore address the deformity at its apex—the Center of Rotation of Angulation (CORA). By performing the osteotomy at the CORA (which typically corresponds to the metaphyseal scar of the original fracture), the surgeon can simultaneously correct angular deformity and translational displacement. The insertion of a precisely contoured corticocancellous interpositional graft acts as a structural buttress, resisting the compressive forces acting across the volar cortex while restoring the critical parameters of radial inclination, volar tilt, and radial height. This biomechanical restoration is the definitive mechanism by which normal carpal kinematics and DRUJ stability are salvaged.
Exhaustive Indications and Contraindications
The decision to proceed with a complex reconstructive procedure such as a volar osteotomy must be based on a rigorous assessment of the patient's symptomatology, functional demands, and radiographic parameters. The primary indication for surgical intervention is a symptomatic malunion in a patient who has failed a comprehensive trial of conservative management, including customized orthoses, non-steroidal anti-inflammatory drugs (NSAIDs), and targeted hand therapy. It is critical to differentiate between a purely radiographic malunion and a symptomatic clinical malunion; surgery is rarely indicated for cosmetic deformity alone in the absence of functional deficit or pain.
Symptomatic patients typically present with a combination of ulnar-sided wrist pain secondary to ulnocarpal impaction, restricted range of motion (especially forearm rotation and wrist flexion), and profound weakness in grip strength due to the altered length-tension relationship of the extrinsic flexor and extensor musculature. Radiographic indications generally include a dorsal tilt exceeding 15 to 20 degrees, radial shortening of greater than 3 to 5 millimeters relative to the contralateral side, and a loss of radial inclination exceeding 10 degrees. Furthermore, intra-articular step-offs greater than 2 millimeters in the radiocarpal joint are a strong indication for surgical intervention to mitigate the rapid onset of post-traumatic osteoarthritis.
Conversely, there are strict contraindications to performing a corrective osteotomy. The most absolute contraindication is the presence of advanced, irreversible post-traumatic osteoarthritis of the radiocarpal or midcarpal joints. In such scenarios, realigning the joint surfaces will not alleviate pain, and salvage procedures such as total wrist arthrodesis, proximal row carpectomy (PRC), or total wrist arthroplasty must be considered. Severe osteopenia or osteoporosis is a relative contraindication, as the compromised bone stock may fail to support the rigid internal fixation required to maintain the correction during graft incorporation. Additionally, patients with profound soft tissue contractures, complex regional pain syndrome (CRPS) in the active phase, or those who are medically unfit for prolonged general anesthesia should be managed non-operatively or with less invasive palliative measures.
| Parameter | Indications for Volar Osteotomy | Contraindications for Volar Osteotomy |
|---|---|---|
| Clinical Symptoms | Intractable ulnar-sided wrist pain, severe loss of grip strength, restricted ROM (supination/flexion) affecting ADLs. | Asymptomatic deformity (purely cosmetic), active Complex Regional Pain Syndrome (CRPS). |
| Radiographic Alignment | Dorsal tilt > 15-20°, Radial shortening > 3-5 mm, Loss of radial inclination > 10°. | Advanced radiocarpal or midcarpal osteoarthritis (requires salvage procedures). |
| Joint Status | Congruent or reducible DRUJ, preserved radiocarpal cartilage space. | Fixed, irreducible DRUJ dislocation with severe arthrosis; widespread carpal collapse (SLAC/SNAC). |
| Patient Factors | High-demand patient, compliant with complex postoperative rehabilitation protocols. | Elderly, low-demand patients; severe osteoporosis; medically unfit for prolonged surgery. |
| Soft Tissue Envelope | Intact volar soft tissue envelope capable of covering hardware. | Active infection, severe compromised volar skin (e.g., prior radiation, extensive scarring). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous, exhaustive preoperative planning is the absolute cornerstone of a successful volar osteotomy. The complexity of a multiplanar deformity dictates that intraoperative "eyeballing" is entirely insufficient and will predictably lead to under-correction or malalignment. The planning phase begins with obtaining high-quality, standardized bilateral radiographic imaging. Zero-rotation posteroanterior (PA) and true lateral radiographs of both the involved and the contralateral (normal) wrists are mandatory. The contralateral wrist serves as the patient's specific anatomic baseline, providing the exact reconstructive targets for radial inclination, volar tilt, radial height, and ulnar variance.
Advanced cross-sectional imaging is now considered the standard of care for complex malunions. A high-resolution computed tomography (CT) scan with 3-dimensional (3D) reconstructions allows the surgeon to precisely define the apex of the deformity, assess for occult intra-articular step-offs, and evaluate the congruity of the sigmoid notch and the DRUJ. In contemporary academic practice, these 3D CT models are frequently utilized in conjunction with computer-assisted design (CAD) software to perform virtual surgical planning (VSP). VSP allows the surgeon to simulate the osteotomy, calculate the exact dimensions of the required bone graft, and even 3D-print patient-specific osteotomy guides and pre-contoured titanium plates.
Traditional radiographic templating remains a critical skill. The surgeon must plan the osteotomy trajectory so that it is strictly transverse in the frontal plane and oblique in the sagittal plane, tracking parallel to the articular surface of the distal fragment. The geometric planning of the structural corticocancellous autograft is paramount. To correct the complex deformity, the graft must be trapezoidal in the frontal plane (wider on the radial aspect to restore radial length and inclination) and triangular in the sagittal plane (with the apex placed dorsally and the broad base volarly to restore volar tilt). The exact millimeter dimensions of this graft must be calculated and recorded prior to the first incision.
Patient positioning and anesthesia require careful coordination with the surgical team. General endotracheal anesthesia is typically preferred due to the duration of the procedure and the need for concomitant iliac crest bone grafting, though a robust regional brachial plexus block combined with deep sedation is a viable alternative if autograft is harvested from a different site or if allograft is utilized. The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table, allowing unimpeded access for the C-arm fluoroscope. A well-padded pneumatic tourniquet is applied to the proximal arm. Concurrently, the ipsilateral or contralateral anterior iliac crest is prepared and draped to facilitate the harvest of the structural corticocancellous bone graft.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a volar osteotomy demands precision, respect for the soft tissue envelope, and rigid adherence to the preoperative template. The procedure begins with the distal extent of the classic Henry approach. A longitudinal incision is made over the course of the flexor carpi radialis (FCR) tendon, extending approximately 8 to 10 centimeters proximally from the distal wrist crease. The superficial fascia is incised, and the FCR tendon sheath is opened. The FCR tendon is retracted ulnarly, which safely protects the median nerve and the palmar cutaneous branch. The radial artery and its accompanying venae comitantes are identified and carefully retracted radially.
Deepening the dissection exposes the pronator quadratus (PQ) muscle. The PQ is incised along its radial and distal borders, leaving a small cuff of tissue radially for later repair. The PQ is elevated as a continuous, full-thickness subperiosteal flap from radial to ulnar, exposing the volar metaphyseal surface of the malunited distal radius. Small Hohmann retractors are placed subperiosteally to protect the neurovascular bundles and flexor tendons. At this stage, the brachioradialis tendon insertion on the radial styloid must be identified and completely released; failure to release this tendon will result in a persistent deforming force that severely hinders the mobilization and lengthening of the distal fragment.
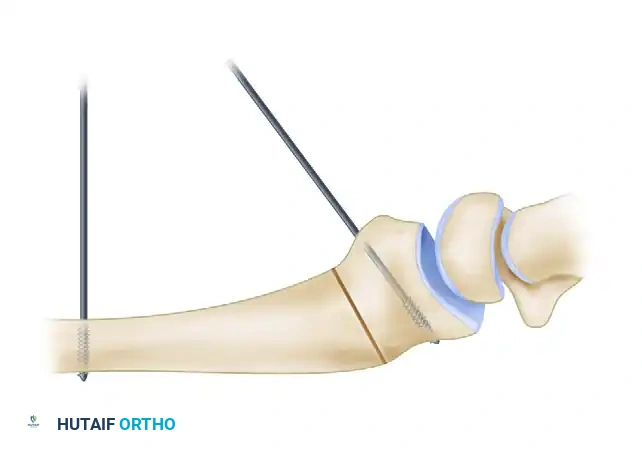
Before the osteotomy is initiated, mechanical references for the planned correction must be established. This is a critical intraoperative validation step. A smooth 0.062-inch Kirschner wire (K-wire) is drilled into the radial diaphysis, proximal to the planned osteotomy site, strictly perpendicular to the long axis of the radius. A second 0.062-inch K-wire is then drilled into the distal articular fragment. This distal wire is inserted at an angle that exactly matches the predetermined sagittal deformity angle calculated during preoperative templating.
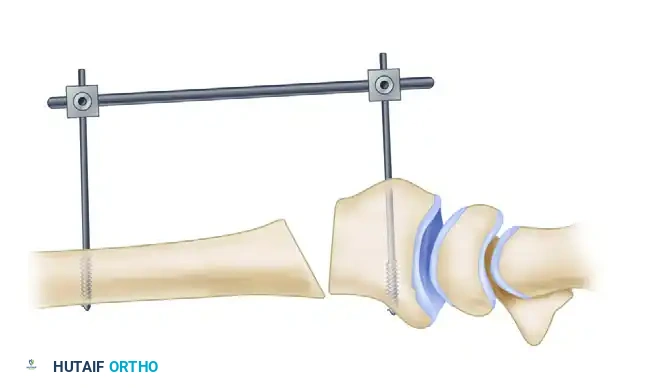
To facilitate controlled distraction and maintain alignment during the procedure, a small external fixator frame or a specialized distraction device is applied. Pins are placed in the radial diaphysis proximally and either the distal radial fragment or the second/third metacarpals distally. With the references in place, the osteotomy is executed using a fine micro-sagittal saw under continuous, copious cold saline irrigation to prevent thermal necrosis of the bone, which is a primary cause of nonunion. The cut is made at the planned site, matching the CORA.

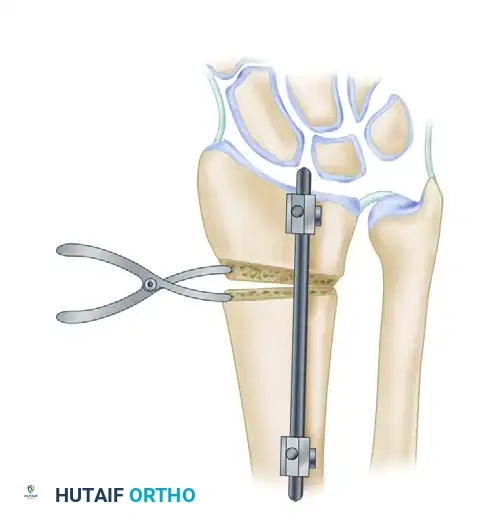
Once the volar and lateral cortices are breached, a small lamina spreader clamp is inserted into the osteotomy gap. The osteotomy is gently and progressively wedged open. It is absolutely crucial to preserve the dorsal periosteum during this maneuver. The intact dorsal periosteal hinge acts as a dynamic tension band, significantly increasing the biomechanical stability of the construct, preventing dorsal translation of the distal fragment, and providing a highly vascularized bed to accelerate bone healing.
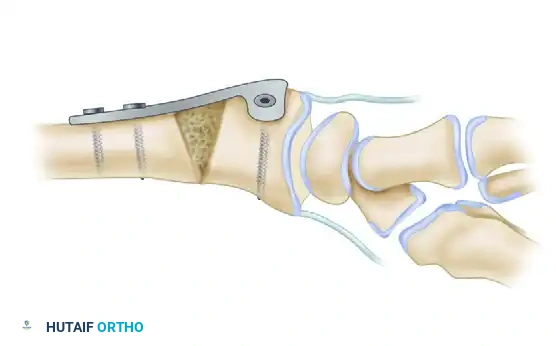
If the preoperative plan dictates a radial lengthening of greater than 10 millimeters, the dorsal periosteum will restrict mobilization and must be transected. This renders the construct highly unstable, demanding perfect graft contouring and exceptionally rigid internal fixation. Based on the defect created by the lamina spreader, a corticocancellous block is harvested from the iliac crest. The graft is meticulously contoured with a rongeur or burr to match the geometric template (trapezoidal and triangular) and is impacted into the defect.

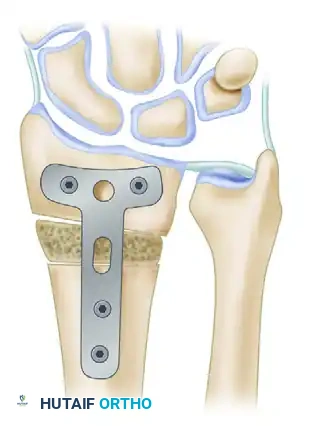
Rigid internal fixation is then achieved using an anatomically contoured volar locking plate. The plate is applied to the volar surface, securing the proximal shaft, the intercalary graft, and the distal articular fragment. When the flat surface of the rigid volar plate is applied and compressed to the volar aspect of the radius, it inherently acts to derotate the distal fragment, effectively correcting the supination/pronation deformity.
Following rigid fixation, the tourniquet is deflated, and the DRUJ is dynamically assessed. If normal ulnar variance is not restored, or if the DRUJ remains tight, a concomitant ulnar shortening osteotomy is performed. While volar plating is the standard, intramedullary (IM) nailing is an alternative for extra-articular deformities, offering a load-sharing construct with minimal soft-tissue disruption, though it requires precise reaming and a sufficient distal fragment.


Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and execution, volar osteotomy for distal radius malunion is a technically demanding procedure associated with a distinct complication profile. The surgeon must be acutely aware of these potential pitfalls and possess the reconstructive armamentarium to manage them effectively. One of the most devastating complications is the attritional rupture of the flexor tendons, particularly the flexor pollicis longus (FPL) and the flexor digitorum profundus (FDP) to the index finger. This occurs when the volar locking plate is positioned too distally, crossing the watershed line and directly abrading the tendons during active flexion. The incidence of tendon irritation or rupture ranges from 2% to 5%. Prevention is paramount: the plate must be seated proximal to the watershed line, and the pronator quadratus must be meticulously repaired over the hardware to serve as a biological barrier.
Nonunion or delayed union at the osteotomy site is another significant complication, occurring in approximately 3% to 5% of cases. This is typically the result of biological or mechanical failure. Biological failures stem from thermal necrosis during the saw cut, inadequate preservation of the soft tissue envelope, or the use of structural allograft instead of highly osteogenic autograft. Mechanical failures arise from insufficient rigid fixation, allowing micromotion at the graft-host interface. If a nonunion occurs and is symptomatic, salvage management requires revision surgery with removal of hardware, aggressive debridement of the nonunion site down to bleeding bone, application of fresh autogenous cancellous bone graft (often supplemented with orthobiologics like BMP-2), and revision rigid internal fixation.
Persistent ulnar-sided wrist pain and DRUJ instability can plague patients even after a radiographically perfect radial osteotomy. This complication, seen in up to 10% of patients, occurs when the chronic malunion has led to irreversible attenuation or tearing of the TFCC, or when the radial osteotomy failed to adequately restore neutral ulnar variance. Intraoperative dynamic assessment of the DRUJ is critical. If instability is noted postoperatively, salvage management may require a delayed ulnar shortening osteotomy to further decompress the ulnocarpal joint, or an arthroscopic/open TFCC repair. In cases of severe, irreversible DRUJ arthrosis, a salvage procedure such as a Darrach procedure or a Sauvé-Kapandji procedure must be considered.
Complex Regional Pain Syndrome (CRPS) is a severe, debilitating complication characterized by disproportionate pain, autonomic dysfunction, and trophic changes. The incidence following distal radius surgery can be as high as 5% to 8%. The exact etiology remains elusive, but it is heavily associated with overly aggressive surgical traction, median nerve irritation, and inadequate postoperative pain control. Early recognition is critical. Management requires a multidisciplinary approach involving aggressive hand therapy focused on active range of motion, neuropathic pain modulators (e.g., gabapentin, pregabalin), and early referral to a pain management specialist for stellate ganglion blocks.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Protocol |
|---|---|---|---|
| FPL / Flexor Tendon Rupture | 2% - 5% | Plate positioned distal to the watershed line; failure to repair pronator quadratus. | Hardware removal; tendon transfer (e.g., FDS of ring finger to FPL) or tendon grafting. |
| Nonunion / Delayed Union | 3% - 5% | Thermal necrosis from saw; use of allograft; inadequate rigid fixation; smoking. | Revision ORIF with fresh autogenous bone grafting (iliac crest) and robust locking plate. |
| Persistent DRUJ Instability | 5% - 10% | Unrecognized TFCC tear; failure to restore ulnar variance; chronic ligamentous laxity. | Ulnar shortening osteotomy; TFCC repair; Sauvé-Kapandji procedure for severe arthrosis. |
| Complex Regional Pain Syndrome | 5% - 8% | Median nerve irritation; excessive surgical distraction; poor postoperative pain control. | Multidisciplinary pain management; stellate ganglion blocks; aggressive active hand therapy. |
| Loss of Correction | < 3% | Violation of dorsal periosteal hinge without adequate structural grafting; patient non-compliance. | Revision osteotomy with structural grafting and enhanced rigid internal fixation. |
Phased Post-Operative Rehabilitation Protocols
The surgical execution of a volar osteotomy represents only half of the reconstructive equation; the ultimate functional outcome is heavily dependent on a structured, scientifically grounded, and phased rehabilitation protocol. The rehabilitation must carefully balance the competing demands of protecting the healing osteotomy and structural graft while simultaneously preventing the debilitating stiffness that rapidly develops in the carpal and radioulnar articulations. This requires close, continuous communication between the operating surgeon and a certified hand therapist (CHT).
Phase 1: Immediate Postoperative and Tissue Healing (0-2 Weeks)
The primary goals of the initial phase are the protection of the surgical construct, aggressive management of postoperative edema, and the prevention of extrinsic tendon adhesions. Immediately following surgery, the wrist is immobilized in a well-padded, bulky volar plaster splint, positioning the wrist in neutral to slight extension. Strict elevation of the extremity above the level of the heart is mandatory to minimize interstitial edema, which is a primary driver of postoperative stiffness and CRPS. The patient is instructed to begin immediate, aggressive active range of motion (ROM) exercises of the digits (full composite flexion and extension), elbow, and shoulder. Tendon gliding exercises are initiated to prevent adhesions of the flexor tendons over the surgical site.
Phase 2: Early Mobilization and Neuromuscular Re-education (2-6 Weeks)
At the two-week postoperative mark, the surgical incisions are inspected, and sutures are removed. The bulky plaster splint is discarded and transitioned to a custom-molded, removable thermoplastic volar wrist orthosis. Under the direct, supervised guidance of the CHT, gentle active and active-assisted ROM exercises for the wrist and forearm are initiated. The focus is on restoring the "dart thrower's motion" (coupled radial extension and ulnar flexion), which minimizes stress on the radiocarpal ligaments while maximizing functional recovery. Forearm rotation (pronation and supination) is gently introduced, respecting patient pain limits. It is imperative that passive stretching and forceful manipulation remain strictly contraindicated during this phase to protect the healing osteotomy and prevent hardware failure.
Phase 3: Strengthening, Proprioception, and Return to Function (6+ Weeks)
At six weeks postoperatively, standardized radiographs are obtained to assess the progression of graft incorporation and osteotomy consolidation. Once clinical signs (absence of pain at the osteotomy site) and radiographic signs (bridging trabeculae across the osteotomy gaps) of union are confirmed, the rehabilitation protocol advances significantly. The thermoplastic splint is gradually weaned during the day. Progressive resistance exercises are introduced to rebuild the strength of the extrinsic flexors and extensors. Proprioceptive neuromuscular facilitation (PNF) techniques are utilized to restore the dynamic stability of the wrist. Work restrictions are carefully managed; patients are strictly prohibited from heavy lifting, impact activities, or manual labor until the osteotomy has achieved complete radiographic consolidation, which typically occurs between 10 to 12 weeks postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the volar osteotomy for distal radius malunion is
