Intramedullary Fixation for Extra-Articular Distal Radius Malunions: A Comprehensive Surgical Guide
Key Takeaway
Intramedullary fixation offers a low-profile, biomechanically robust alternative to volar plating for extra-articular distal radius malunions. This technique utilizes a completely intraosseous implant, minimizing soft tissue irritation. Successful execution requires precise preoperative planning, meticulous dorsal approach, corrective osteotomy, and provisional reduction prior to nail insertion. This guide details the indications, step-by-step surgical technique, and postoperative protocols for optimal functional recovery.
Comprehensive Introduction and Patho-Epidemiology
Extra-articular malunions of the distal radius represent a profoundly complex reconstructive challenge for the orthopedic surgeon, often resulting from the nonoperative management of initially displaced fractures, secondary loss of reduction following closed treatment, or failure of initial surgical fixation. The anatomic distortion—classically characterized by a critical loss of radial length, altered radial inclination, and abnormal sagittal alignment (predominantly dorsal tilt)—profoundly disrupts the intricate kinematics of both the radiocarpal and distal radioulnar joints (DRUJ). When the distal radius heals in a malaligned position, the transmission of forces across the wrist is pathologically altered. Normally, the distal radius absorbs approximately 80% of the axial load transmitted through the carpus; however, with increasing dorsal tilt and radial shortening, this load is disproportionately shifted to the triangular fibrocartilage complex (TFCC) and the ulnar head, leading to rapid and debilitating ulnocarpal impaction syndrome.
Patients presenting with symptomatic extra-articular malunions typically describe a constellation of progressive, functionally limiting symptoms. These include chronic midcarpal pain exacerbated by loading, severely restricted range of motion (particularly in supination and wrist extension), diminished grip strength, and focal ulnar-sided wrist pain secondary to ulnocarpal abutment. Furthermore, the dorsal angulation of the distal radial articular surface alters the moment arms of the extrinsic flexor and extensor tendons, significantly decreasing their mechanical advantage and contributing to global weakness of the hand and wrist. The adaptive shortening of the soft tissues, particularly the brachioradialis and the volar radiocarpal ligaments, further tethers the carpus in a pathologically translated position, complicating surgical reconstruction.
Historically, the gold standard for addressing these complex deformities has been the corrective osteotomy stabilized with volar locking plate technology. While volar plates have revolutionized the management of acute distal radius fractures, their application in the setting of corrective osteotomies is not without significant morbidity. The application of a volar plate often requires extensive soft tissue stripping, mobilization of the pronator quadratus, and carries a well-documented risk of flexor tendon irritation or catastrophic rupture due to hardware prominence at the watershed line. Furthermore, the eccentric placement of a volar plate creates a load-bearing construct that is subject to substantial cantilever bending forces, particularly when a large structural bone graft is required to fill the osteotomy void.
In response to these biomechanical and soft-tissue challenges, intramedullary fixation has emerged as a highly effective, low-profile alternative for the stabilization of distal radius osteotomies. Pioneered and rigorously validated by Ilyas et al., modern intramedullary implants (such as the MICRONAIL; Wright Medical, Memphis, TN) are designed to sit entirely within the medullary canal of the distal radius. This intraosseous position theoretically eliminates the risk of hardware-induced flexor and extensor tendon rupture, as there is no extra-cortical hardware prominence. More importantly, an intramedullary device provides a load-sharing biomechanical construct. By residing within the central mechanical axis of the radius, the nail neutralizes bending and torsional forces highly effectively, sharing the physiological loads with the surrounding cortical bone and the interpositional structural bone graft, thereby creating an optimal biological environment for osteotomy consolidation.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the osseous and soft tissue anatomy of the distal radius is the absolute prerequisite for executing a safe and effective intramedullary corrective osteotomy. The distal radius transitions from a dense, diaphyseal cortical tube to a metaphyseal flare composed predominantly of cancellous bone enclosed by a thin cortical shell. The medullary canal of the distal radius is not perfectly cylindrical; rather, it exhibits a distinct "teardrop" or elliptical cross-section, being wider in the coronal plane than in the sagittal plane. This anatomical nuance dictates the design of intramedullary nails, which must be contoured to accommodate the distal metaphyseal flare while achieving an interference fit within the narrower diaphyseal isthmus. The volar cortex of the distal radius is relatively flat and thick, providing a robust buttress, whereas the dorsal cortex is convex, thinner, and highly irregular, featuring Lister’s tubercle which acts as a fulcrum for the extensor pollicis longus (EPL) tendon.
The extensor retinaculum and the six dorsal extensor compartments intimately overlie the dorsal radius. The surgical approach for intramedullary nailing typically exploits the interval between the third and fourth dorsal compartments. The third compartment, housing the EPL tendon, courses obliquely around Lister’s tubercle. Transposition of the EPL tendon radially is a critical step to protect it from iatrogenic injury during canal preparation and to prevent postoperative attrition against the dorsal cortical window. Deep to the extensor tendons lies the dorsal radiocarpal ligament complex and the highly vascular dorsal periosteum. In the context of a corrective osteotomy, preserving the volar periosteal hinge—when anatomically feasible—is paramount. The volar periosteum not only provides a tension band that aids in restoring palmar tilt during an opening wedge osteotomy but also houses critical vascular contributions from the anterior interosseous artery, which are vital for the incorporation of the structural bone graft.
Biomechanically, the rationale for intramedullary fixation in the distal radius is rooted in the principles of the central mechanical axis and load-sharing. Eccentric fixation devices, such as volar locking plates, act as load-bearing implants. When an opening wedge osteotomy is performed and a bone graft is interposed, a volar plate is subjected to massive cantilever bending forces every time the patient extends the wrist or loads the hand. If the bone graft resorbs or fails to incorporate rapidly, these cyclic bending forces can lead to fatigue failure of the plate or screw pullout. Conversely, an intramedullary nail acts as an internal splint located at the neutral axis of the bone. Bending moments applied to the wrist are converted into compressive forces along the nail and the interpositional bone graft. This load-sharing phenomenon not only protects the implant from fatigue failure but also stimulates osteogenesis within the graft according to Wolff’s Law.
The specific design features of modern distal radius intramedullary nails maximize this biomechanical advantage. Distal fixation is typically achieved via three interlocking threaded pegs or screws placed in a divergent, multi-planar configuration. This divergent pattern captures the dense subchondral bone of the radial styloid, the dorsal rim, and the volar lunate facet, effectively creating a stable foundation within the distal fragment that resists subsidence and loss of inclination. Proximal fixation is achieved through the insertion of bicortical interlocking screws directed from dorsal to volar through the diaphyseal portion of the nail. These proximal screws are critical for neutralizing torsional forces and locking in the restored radial length. The entire construct, once locked, acts as a highly rigid, fixed-angle device that maintains the meticulously restored spatial relationship of the radiocarpal joint and the DRUJ while remaining entirely shielded from the surrounding gliding soft tissues.
Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of success when considering intramedullary fixation for the correction of extra-articular distal radius malunions. The decision to proceed with a complex reconstructive osteotomy must never be based on radiographic appearance alone; it requires a careful synthesis of the patient’s functional demands, clinical symptomatology, and precise radiographic parameters. The ideal candidate is a symptomatic patient with a mature, extra-articular deformity who possesses adequate bone stock to support the rigid internal fixation provided by the intramedullary nail.
Clinical indications for intervention include persistent, activity-limiting wrist pain that has failed nonoperative modalities (such as custom splinting, NSAIDs, and targeted corticosteroid injections). Patients often present with profound weakness in grip strength, which is directly attributable to the loss of the optimal resting length of the extrinsic flexor and extensor musculature. Furthermore, symptomatic ulnocarpal impaction—manifesting as focal pain at the TFCC, exacerbation of pain with forceful pronation and ulnar deviation, and occasionally palpable crepitus at the DRUJ—is a primary driver for surgical intervention. Restoring radial length and correcting dorsal tilt are essential to decompress the ulnar compartment and restore congruent kinematics to the DRUJ.
Radiographic and Clinical Parameters
| Parameter | Threshold for Osteotomy Indication | Biomechanical Consequence of Deformity |
|---|---|---|
| Radial Inclination | Loss of >15 degrees from anatomic normal | Alters radiocarpal load distribution; increases shear stress on the scaphoid and scapholunate ligament. |
| Radial Length | Shortening of >4 mm compared to contralateral side | Leads to positive ulnar variance, ulnocarpal abutment, TFCC tears, and DRUJ subluxation. |
| Ulnar Variance | Positive variance of ≥4 mm | Direct impaction of the ulnar head against the lunate and triquetrum; chondromalacia. |
| Sagittal Tilt | >15 degrees dorsal OR >20 degrees volar tilt | Shifts >50% of axial load to the ulna; severely limits wrist flexion/extension arc; alters tendon moment arms. |
| DRUJ Congruity | Subluxation or dislocation on true lateral | Loss of forearm rotation; chronic instability; early onset secondary osteoarthritis of the sigmoid notch. |
While intramedullary fixation is a powerful tool, it is subject to strict contraindications that must be respected to prevent catastrophic surgical failures. Absolute contraindications include the presence of active local or systemic infection, which precludes the implantation of any hardware, particularly an intramedullary device that could propagate infection throughout the diaphyseal canal. Intra-articular malunions represent a critical absolute contraindication for isolated intramedullary nailing. The nail is a fixed-angle device designed to control the meta-diaphyseal relationship; it possesses no mechanism to independently reduce, compress, or stabilize articular step-offs or gap deformities within the radiocarpal joint. Patients with skeletal immaturity and open physes are also absolutely contraindicated, as the nail and reaming process will cause iatrogenic physeal arrest.
Relative contraindications require nuanced surgical judgment. Severe osteopenia or advanced osteoporosis poses a significant risk, as the divergent distal interlocking screws rely on the purchase of subchondral bone to prevent hardware migration and loss of reduction. In severely osteoporotic bone, the screws may "cut out" or fail to provide adequate pull-out strength, rendering the construct unstable. Additionally, pre-existing diaphyseal deformities, excessive bowing of the radius, or an unusually narrow medullary canal (less than the diameter of the smallest available nail) may physically preclude the safe passage of the straight intramedullary device, risking iatrogenic fracture during insertion.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous, exhaustive preoperative planning is the absolute cornerstone of a successful corrective osteotomy. The tolerance for error in restoring the complex three-dimensional anatomy of the distal radius is minimal. The planning process begins with obtaining high-quality, standardized imaging. True posteroanterior (PA) and true lateral radiographs of both the affected wrist and the contralateral (normal) wrist are mandatory. The uninjured contralateral wrist serves as the patient’s specific anatomic template, establishing the target parameters for radial length, volar tilt, and radial inclination. It is critical that the PA radiographs are taken with the shoulder abducted to 90 degrees and the elbow flexed to 90 degrees to ensure neutral forearm rotation, as pronation or supination will artificially alter the radiographic measurement of ulnar variance.
Advanced imaging is highly recommended and is considered the standard of care for complex malunions. A fine-cut Computed Tomography (CT) scan (slice thickness of 1 mm or less) with multi-planar formatting and 3D surface-rendered reconstructions provides invaluable data. The CT scan allows the surgeon to precisely map the apex of the deformity, which dictates the exact level of the osteotomy. It also facilitates a detailed evaluation of the DRUJ congruity, identifying any hidden intra-articular step-offs or established osteoarthritis at the sigmoid notch that might necessitate a concomitant DRUJ salvage procedure (e.g., Darrach or Sauvé-Kapandji). Furthermore, CT imaging allows for the assessment of the medullary canal diameter and the subchondral bone stock available for distal screw purchase.
Preoperative templating, whether digital or using traditional acetate overlays, is a non-negotiable step. The surgeon must determine the Center of Rotation of Angulation (CORA). In most extra-articular malunions, the CORA lies at the metaphyseal level. The osteotomy should ideally be placed exactly at the CORA to allow for pure angular correction without introducing secondary translational deformities. Templating dictates the exact site of the osteotomy, the precise dimensions (base and height) of the required structural corticocancellous bone graft, and the appropriate length and diameter of the intramedullary nail. The surgeon must ensure that the chosen nail length will allow the proximal interlocking screws to engage healthy, thick diaphyseal cortical bone well proximal to the osteotomy site.
Patient positioning and operating room setup must be optimized to facilitate unhindered surgical access and flawless fluoroscopic imaging. The patient is placed in the supine position with the affected extremity extended on a fully radiolucent hand table. A well-padded proximal arm tourniquet is applied to provide a bloodless surgical field. The positioning of the image intensifier (C-arm) is critical; it should be brought in parallel to the hand table, entering from the head or the foot of the table, depending on the room configuration. This setup allows the surgeon to obtain seamless AP and lateral fluoroscopic views simply by rotating the patient's forearm, without needing to move the C-arm or compromise the sterile field. The ipsilateral anterior iliac crest must also be prepped and draped in a standard sterile fashion to facilitate the harvesting of the structural corticocancellous bone graft, which is an obligate step in an opening wedge osteotomy.
Step-by-Step Surgical Approach and Fixation Technique
1. Surgical Approach and Soft Tissue Dissection
The procedure begins with a 3-to-4-cm longitudinal dorsal incision centered precisely over Lister’s tubercle, extending proximally over the radial shaft. Superficial dissection must be performed with extreme care, utilizing sharp dissection through the dermis and then blunt dissection through the subcutaneous tissues to identify and protect the terminal dorsal sensory branches of the radial nerve radially, and the dorsal cutaneous branch of the ulnar nerve ulnarly. The extensor retinaculum is exposed, and the third dorsal compartment is identified. The retinaculum covering the third compartment is incised longitudinally, and the extensor pollicis longus (EPL) tendon is mobilized, released from its fibro-osseous sheath, and transposed radially into the subcutaneous tissues.
Following EPL transposition, deep dissection proceeds by developing the interval between the second compartment (ECRL/ECRB) and the fourth compartment (EDC/EIP). The EDC tendons are retracted ulnarly, exposing the dorsal radiocarpal ligament and the dorsal periosteum of the distal radius. The hypertrophied periosteum and scar tissue overlying the malunion site are meticulously elevated as full-thickness flaps. It is imperative to expose the bone adequately to visualize the planned osteotomy site while preserving as much soft tissue attachment as possible to maintain vascularity.
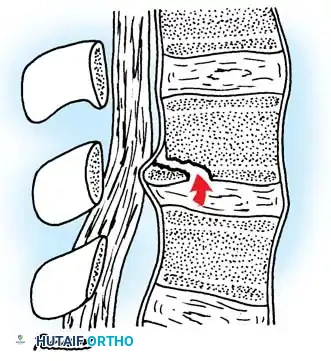
2. Execution of the Corrective Osteotomy
Using the preoperative template and fluoroscopic guidance, the exact site of the osteotomy (at the CORA) is marked on the dorsal cortex. The osteotomy is initiated using a fine-toothed oscillating saw under continuous, copious cold saline irrigation to prevent thermal necrosis of the bone, which would severely compromise graft incorporation. For classic dorsally angulated malunions, the dorsal, radial, and ulnar cortices are cut. The surgeon must exercise extreme caution as the saw blade approaches the volar cortex. Ideally, the volar periosteum and a thin hinge of volar cortical bone are left intact to act as a tension band during the opening of the wedge.
Once the cortices are breached, a sharp osteotome is inserted into the dorsal osteotomy site. A laminar spreader is then carefully introduced and slowly opened to hinge the distal fragment volarly, restoring palmar tilt and radial length. In cases of severe shortening or complex multi-planar deformities where the cortices are overlapped, a simple opening wedge is insufficient; the osteotomy must be completed circumferentially, and the distal fragment fully mobilized.
3. Soft Tissue Release and Deformity Correction
Mobilization of the distal fragment is often the most challenging aspect of the procedure due to chronic soft tissue contractures. A critical, non-negotiable step is the complete release of the brachioradialis tendon from its broad insertion on the radial styloid. The brachioradialis is a massive deforming force; failure to release it will make the restoration of radial length physically impossible and will place catastrophic tension on the hardware and the bone graft. Additionally, the volar radiocarpal ligaments and the pronator quadratus may require partial release or fractional lengthening to allow the distal fragment to be translated and tilted into its anatomic position.
4. Provisional Reduction and K-Wire Fixation
This is the most critical conceptual departure from volar plating. An intramedullary nail is a space-occupying, fixed-angle device; it cannot be used as a lever to reduce the fracture. Therefore, the distal radius must be anatomically reduced and provisionally stabilized before the nail is introduced. Once length, tilt, and inclination are manually restored, the reduction is provisionally held using one or two 0.062-inch Kirschner wires (K-wires). Crucially, these K-wires must be placed peripherally—typically directed from the radial styloid obliquely into the proximal ulnar cortex, or placed entirely along the dorsal or ulnar columns. They must not cross the central medullary canal, as they will block the passage of the reamers and the nail. The provisional reduction is then rigorously verified using multi-planar fluoroscopy to ensure it perfectly matches the preoperative template.
5. Canal Preparation and Nail Insertion
With the provisional reduction secured, a starting portal is created in the dorsal aspect of the distal radial articular block, typically just ulnar to Lister's tubercle, taking immense care to remain extra-articular and not breach the radiocarpal joint. A guide wire is advanced down the medullary canal, and the canal is sequentially prepared using system-specific flexible reamers or broaches. The selected intramedullary nail is then introduced over the guide wire. The nail must be advanced until its proximal end is completely countersunk beneath the dorsal cortical surface to prevent any impingement on the overlying extensor tendons.
6. Distal and Proximal Locking
Once the nail is appropriately seated, the outrigger targeting guide is attached. Distal fixation is achieved first. Three interlocking pegs or screws are inserted through the guide in a divergent pattern, capturing the dense subchondral bone of the radial styloid, the dorsal rim, and the volar lunate facet. Following secure distal fixation, the proximal diaphyseal fixation is addressed. Through separate small stab incisions guided by the targeting jig, two 2.7-mm bicortical interlocking screws are drilled and inserted from dorsal to volar. These screws lock the nail to the proximal diaphysis, effectively neutralizing all rotational forces and permanently securing the restored length and alignment.
7. Structural Bone Grafting and DRUJ Assessment
The opening wedge osteotomy inevitably creates a significant structural void. This defect must be filled to prevent delayed union, nonunion, or fatigue failure of the nail. A precisely measured corticocancellous block is harvested from the ipsilateral anterior iliac crest. The graft is meticulously shaped with a rongeur or burr to match the exact dimensions of the trapezoidal defect and is firmly impacted into place. The intramedullary nail provides the rigid mechanical stability, while the graft provides the essential osteoconductive scaffold and osteoinductive factors required for rapid bony consolidation.
Finally, the DRUJ must be dynamically assessed. With the radius anatomically restored and rigidly fixed, the surgeon evaluates passive pronation and supination. In the majority of cases, restoring the radial anatomy will spontaneously relocate and stabilize the DRUJ. However, if persistent instability or severe crepitus is noted due to chronic articular damage, a concomitant procedure (such as a Darrach resection or a Sauvé-Kapandji arthrodesis) must be performed during the same surgical setting to ensure a pain-free, functional outcome. The wound is then thoroughly irrigated, the extensor retinaculum is closed loosely (leaving the EPL transposed), and a layered closure is performed.
Complications, Incidence Rates, and Salvage Management
While intramedullary fixation of distal radius malunions yields highly predictable and excellent clinical outcomes in appropriately selected patients, the technique is technically demanding. Surgeons must be acutely aware of potential complications, understand their incidence, and possess the requisite knowledge to execute salvage strategies. The intraosseous nature of the implant mitigates many soft-tissue complications associated with plating, but it introduces unique osseous challenges.
Exhaustive Complication Profile and Management
| Complication | Estimated Incidence | Etiology / Pathophysiology | Salvage and Management Strategy |
|---|---|---|---|
| Inadequate Reduction / Malalignment | 2% - 5% | Failure to achieve or maintain perfect provisional K-wire reduction prior to reaming. The nail follows the reamed path, locking the bone in malalignment. | Immediate intraoperative recognition is crucial. Remove the nail, revise the osteotomy, re-reduce, and stabilize with K-wires. If the canal is excessively widened, convert to a volar or dorsal locking plate. |
| Hardware Prominence / Tendon Irritation | 1% - 3% | Proximal interlocking screws are excessively long and protrude through the volar cortex, irritating the Flexor Pollicis Longus (FPL) or deep flexors. | Precise depth measurement using the gauge and fluoroscopy is mandatory. If symptomatic postoperatively, isolated removal of the offending proximal screws after radiographic union is achieved. |
| Nonunion / Delayed Union | 3% - 6% | Inadequate structural bone grafting, thermal necrosis during osteotomy, or patient non-compliance (e.g., smoking). Leads to fatigue failure of the nail. | Revision surgery is required. Removal of the IM nail, aggressive debridement of the nonunion site, massive autologous bone grafting (iliac crest), and conversion to rigid dual-plate fixation. |
| Iatrogenic Radial Shaft Fracture | < 2% | Overzealous reaming, failure to account for diaphyseal bowing, or forceful insertion of the nail into an excessively narrow medullary isthmus. | If non-displaced, it may be bypassed by using a longer IM nail if available. If displaced or unstable, the nail must be removed, and the entire radius (including the osteotomy and the fracture) stabilized with a long, spanning volar locking plate. |
| Loss of Distal Fixation / Subsidence | 2% - 4% | Severe unrecognized osteopenia; distal screws fail to achieve subchondral purchase, leading to collapse of the osteotomy wedge and loss of length. | If detected early with significant loss of alignment, revision to a volar plate with locking pegs and supplementary K-wire fixation is necessary. May require augmentation with bone cement (PMMA) in extreme osteoporotic cases. |
The most critical pitfall unique to intramedullary nailing is the assumption that the nail will aid in reduction. Surgeons transitioning from volar plating must consciously alter their operative sequencing. Furthermore, meticulous attention must be paid to the distal locking screws. The targeting guides for intramedullary systems are precise, but the trajectory of the divergent screws places them in close proximity to the radiocarpal articular surface. Unrecognized intra-articular penetration of a distal screw will result in rapid, catastrophic chondrolysis of the carpus. Multi-planar fluoroscopy, including 20-degree elevated lateral views and individual facet views, must be utilized to definitively confirm that all hardware is extra-articular prior to closure.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following an intramedullary corrective osteotomy must strike a delicate, individualized balance. The surgeon must weigh the absolute necessity of protecting the osteotomy site and the structural bone graft against the paramount need for early mobilization to prevent debilitating stiffness, tendon adhesions, and complex regional pain syndrome (CRPS). Because the intramedullary nail acts as a load-sharing device, it inherently relies on the surrounding bone and graft for ultimate stability. Therefore, the rehabilitation phases are heavily dictated by the magnitude of the deformity correction and the size of the interpositional graft.
Phase 1: Immediate Postoperative Phase (0-2 Weeks)
Immediately following surgery, the wrist is immobilized in a bulky, well-padded volar and dorsal resting splint in a neutral position. The primary goals during this acute phase are strict edema control and the prevention of digital stiffness. The patient is instructed to keep the extremity elevated above the level of the heart at all times. Active, full-excursion range of motion of the fingers and thumb is initiated in the recovery room and must be performed hourly. Shoulder and elbow mobilization are also heavily emphasized. The patient is strictly non-weight-bearing on the operative extremity.
Phase 2: Early Rehabilitation and Protected Mobilization (2-6 Weeks)
At the two-week postoperative mark, the surgical dressings and sutures are removed. For standard corrections (requiring less than 10 mm of lengthening and a standard graft), the rigid surgical splint is discontinued. The patient is transitioned to a custom-molded, removable thermoplastic wrist splint. Supervised physical therapy is initiated. The focus shifts to active and active-assisted range of motion of the wrist (flexion, extension, radial/ulnar deviation) and the forearm (pronation, supination). The "dart-thrower's motion" is particularly encouraged, as it maximizes midcarpal motion while minimizing stress on the radiocarpal joint and the healing osteotomy. The splint is worn at all times except during therapy sessions and hygiene.
Special Consideration for Massive Corrections: If the corrective osteotomy required a massive lengthening (greater than 10 mm), the tension on the soft tissues, the neurovascular structures, and the graft site is exceptionally high. In these specific, high-risk cases, early mobilization is contraindicated. The patient is transitioned into a well-molded, short-arm fiberglass cast for an additional 4 weeks (total of 6 weeks of rigid immobilization) to prevent graft subsidence or hardware failure.
Phase 3: Consolidation and Strengthening Phase (8-12+ Weeks)
At 8 weeks postoperatively, new orthogonal radiographs are obtained to assess for bridging trabeculae across the osteotomy and graft interfaces. Activities against resistance, heavy lifting, and manual labor remain strictly prohibited until definitive radiographic union is confirmed by the operating surgeon. Once clinical and radiographic union is achieved, the removable splint is permanently discontinued. Progressive strengthening exercises are introduced, focusing on restoring grip strength, eccentric flexor/extensor control, and proprioception. Patients are advised that maximal functional recovery, particularly regarding grip strength and terminal range of motion, may take up to 12 to 18 months. Routine hardware removal is not indicated due to the deeply buried, intraosseous nature of the implant, unless specifically requested by the patient after complete bony consolidation or in the rare event of localized symptomatic hardware irritation.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for distal radius malunions is deeply rooted in biomechanical research and clinical outcomes studies. Historically, the foundation of corrective osteotomies was established by Diego Fernandez in the 1980s, who popularized the dorsal opening wedge osteotomy utilizing iliac crest bone graft and dorsal plate fixation. While anatomically successful, dorsal plating was plagued by unacceptably high rates of extensor tendon tenosynovitis and rupture. The subsequent paradigm shift toward volar locking plates, championed by Orbay and others in the early 2000s, significantly reduced extensor tendon complications but introduced new challenges, specifically flexor tendon ruptures and the biomechanical disadvantages of cantilever bending when bridging large osteotomy gaps.
The advent of intramedullary fixation for the distal radius represents the latest evolutionary step, addressing the shortcomings of eccentric plating. The landmark biomechanical studies by Ilyas et al. provided the foundational justification for this technique. Their cadaveric research demonstrated that intramedullary nails, utilizing a
