Distal Radius Fractures: Comprehensive Classification, Stability Assessment, and Operative Management

Key Takeaway
Distal radius fractures demand meticulous assessment of stability and articular congruity. While stable patterns may be managed with closed reduction and casting, unstable fractures—defined by LaFontaine’s criteria—often necessitate operative intervention. Treatment strategies range from percutaneous pinning to rigid internal fixation, tailored to patient demand, bone quality, and fracture morphology to optimize functional recovery and minimize post-traumatic arthrosis.
Comprehensive Introduction and Patho-Epidemiology
Patho-Epidemiology of Distal Radius Fractures
Distal radius fractures represent one of the most ubiquitous injuries encountered in orthopedic traumatology, accounting for approximately one-sixth of all fractures treated in emergency departments. The epidemiological profile of these fractures demonstrates a classic bimodal distribution. In the younger demographic, these injuries are typically the consequence of high-energy trauma, such as motor vehicle collisions or falls from a significant height, frequently resulting in complex, intra-articular shear or highly comminuted fracture patterns. Conversely, in the elderly population, particularly post-menopausal women, these fractures occur via low-energy mechanisms, such as a fall from a standing height onto an outstretched hand (FOOSH), reflecting underlying osteopenia or osteoporosis.
The management of these fractures has evolved significantly, transitioning from historical reliance on closed reduction and cast immobilization to a nuanced, evidence-based approach that heavily incorporates operative intervention for unstable patterns. The primary goal of treatment is the restoration of normal wrist anatomy—specifically radial height, volar tilt, radial inclination, and articular congruity—to maximize functional outcomes and mitigate the risk of post-traumatic osteoarthritis. Achieving this requires a profound understanding of fracture morphology, biomechanical stability, and patient-specific physiological demands. Failure to restore articular congruity to within 2 millimeters is historically correlated with a nearly 100% incidence of radiographic post-traumatic arthrosis, though clinical symptomatology may not always mirror radiographic severity.
Established Classification Systems
More than 20 classification systems have been proposed for distal radial fractures. As with most fracture classifications, the intraobserver and interobserver agreement rates usually are only moderate at best. However, these classifications are indispensable for understanding fracture pathoanatomy, facilitating academic communication, and conceptualizing the biomechanical challenges inherent in treatment.
Gartland and Werley Classification (1951)
This foundational system emphasizes metaphyseal comminution, intra-articular extension, and fragment displacement. It is primarily descriptive and serves as a historical baseline for understanding fracture severity.
* Group 1: Simple Colles fracture (extra-articular, non-comminuted).
* Group 2: Comminuted Colles fracture, undisplaced intra-articular fragment.
* Group 3: Comminuted Colles fracture, displaced intra-articular fragment.
Frykman Classification (1967)
Frykman advanced the assessment by incorporating the involvement of the radioulnar and radiocarpal joints, as well as the presence of an ulnar styloid fracture. A key mnemonic for this system is that even numbers indicate an associated ulnar styloid fracture.
* Group 1 / 2: Extra-articular (without / with ulnar styloid fracture).
* Group 3 / 4: Intra-articular involving the radiocarpal joint (without / with ulnar styloid fracture).
* Group 5 / 6: Intra-articular involving the distal radioulnar joint (DRUJ) (without / with ulnar styloid fracture).
* Group 7 / 8: Intra-articular involving both radiocarpal and DRUJ (without / with ulnar styloid fracture).
Melone Classification (1986)
Melone evaluated the four major fracture components: the radial shaft, the radial styloid, the dorsal medial fragment, and the volar medial fragment. This system is highly relevant for understanding "die-punch" injuries and the critical importance of the lunate facet.
* Type 1: Undisplaced, minimal comminution, stable.
* Type 2: Unstable, displacement of the medial complex, moderate-to-severe comminution.
* Type 3: Displacement of the medial complex as a unit plus an anterior spike.
* Type 4: Wide separation or rotation of the dorsal fragment and palmar fragment rotation.
Fernandez Classification (1987)
Fernandez revolutionized treatment algorithms by basing his classification system on the mechanism of injury. This system directly guides the choice of surgical fixation.
* Type 1 (Bending): One cortex of the metaphysis fails due to tensile stress; opposite cortex with some comminution (e.g., classic Colles or Smith fractures).
* Type 2 (Shearing): Fracture of the joint surface (e.g., Barton or reverse Barton fractures). Requires buttress plate fixation.
* Type 3 (Compression): Fracture of the joint surface with impaction of subchondral and metaphyseal bone, intra-articular comminution (die-punch). Requires bone grafting and support.
* Type 4 (Avulsion): Fracture of the ligament attachments of the ulnar and radial styloid process, radiocarpal fracture-dislocation (e.g., Chauffeur's fracture).
* Type 5 (Combination): High-velocity injuries combining multiple mechanisms.
Cooney Universal Classification (1990)
* Type 1: Extra-articular, undisplaced.
* Type 2: Extra-articular, displaced.
* Type 3: Intra-articular, undisplaced.
* Type 4: Intra-articular, displaced.
Modified AO/OTA Classification
The AO system remains the gold standard for academic research, categorizing fractures based on articular involvement.
* Type A: Extra-articular.
* Type B: Partial articular (B1: radial styloid, B2: dorsal rim, B3: volar rim, B4: die-punch).
* Type C: Complete articular (metaphyseal dissociation from the diaphysis).
Assessment of Stability and Displacement Risk
Most distal radial fractures are initially treated with immobilization after closed reduction. Unfortunately, many of these fractures lose reduction, or the initial reduction is deemed unacceptable upon critical radiographic review, leading to poor functional outcomes. Identifying fractures at high risk for displacement is paramount.
The LaFontaine Criteria
LaFontaine et al. identified five critical factors indicative of inherent fracture instability. The presence of three or more of these factors strongly predicts the failure of conservative management:
1. Initial dorsal angulation of more than 20 degrees (severe loss of volar tilt).
2. Dorsal metaphyseal comminution.
3. Intra-articular involvement.
4. An associated ulnar fracture (ulnar styloid or neck).
5. Patient age older than 60 years (a surrogate for osteopenia/osteoporosis).
Other suggested indicators of instability include initial radial shortening of greater than 5 mm and significant volar comminution. A fracture that requires excessive molding or extreme wrist flexion (Cotton-Loder position) to maintain reduction is inherently unstable and should be considered for operative fixation. If closed treatment is chosen for a fracture with questionable stability, meticulous and close monitoring is advised. Fractures considered potentially unstable must be evaluated with serial radiographs (typically at 1, 2, and 3 weeks post-injury) until early fracture callus provides mechanical stability.
Detailed Surgical Anatomy and Biomechanics
Osseous Architecture and Radiographic Parameters
The distal radius is structurally complex, transitioning from a dense diaphyseal cortical tube to a metaphyseal flare composed of thin cortical bone surrounding a cancellous core. This transition zone is mechanically vulnerable, explaining the high incidence of metaphyseal fractures. The articular surface features two distinct concavities—the scaphoid and lunate facets—separated by a subtle anteroposterior ridge.
Normal radiographic parameters are critical for both initial assessment and intraoperative evaluation of reduction. The normal radial inclination averages 22 degrees (range 21–25 degrees), measured on an AP radiograph as the angle between a line perpendicular to the long axis of the radius and a line drawn from the radial styloid tip to the ulnar corner of the lunate facet. Normal radial height averages 11 to 12 mm. On the lateral view, the normal volar tilt averages 11 degrees (range 2–20 degrees). Restoration of volar tilt is particularly crucial; dorsal angulation alters carpal kinematics, shifting load-bearing forces dorsally and ulnarly, which significantly increases forces across the DRUJ and the ulnocarpal joint.
Rikli and Regazzoni conceptualized the distal radioulnar articulation as a three-column biomechanical model. The lateral (radial) column comprises the radial styloid and scaphoid facet, acting as an osseous buttress. The intermediate column encompasses the lunate facet and the sigmoid notch, serving as the primary load-bearing axis for the radiocarpal joint. The medial (ulnar) column includes the distal ulna, TFCC, and DRUJ, functioning as the axis of forearm rotation.
Ligamentous Stabilizers and the Triangular Fibrocartilage Complex
The distal radius is heavily invested with stout volar ligaments and relatively thinner dorsal ligaments. The volar radiocarpal ligaments (radioscaphocapitate, long radiolunate, and short radiolunate) are critical stabilizers of the carpus. The short radiolunate ligament firmly tethers the lunate to the volar margin of the lunate facet; thus, in volar marginal shear fractures (volar Barton's), the lunate frequently subluxates with the fracture fragment.
The Triangular Fibrocartilage Complex (TFCC) is the primary stabilizer of the DRUJ and acts as a shock absorber for the ulnocarpal joint. It originates from the sigmoid notch of the radius and inserts broadly onto the base of the ulnar styloid (fovea). Avulsion of the ulnar styloid base frequently compromises the deep radioulnar ligaments of the TFCC, leading to DRUJ instability.

Associated Ulnar Injuries and DRUJ Biomechanics
Distal radius fractures rarely occur in isolation. The distal radioulnar joint (DRUJ) and the ulnar styloid are frequently compromised, significantly altering the stability of the forearm axis.
Galeazzi Fracture-Dislocations
A Galeazzi injury involves a fracture of the distal third of the radial shaft coupled with a dislocation or subluxation of the DRUJ. These are highly unstable injuries that mandate operative intervention in adults. The radius must be anatomically reduced and rigidly fixed, typically utilizing a dynamic compression plate (DCP) or a locking compression plate (LCP). Following radial fixation, the DRUJ must be assessed for stability throughout the forearm arc of motion. If the DRUJ remains unstable, it is often pinned in supination using parallel Kirschner wires.

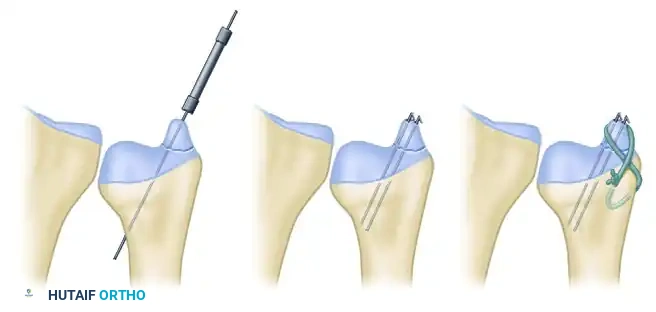
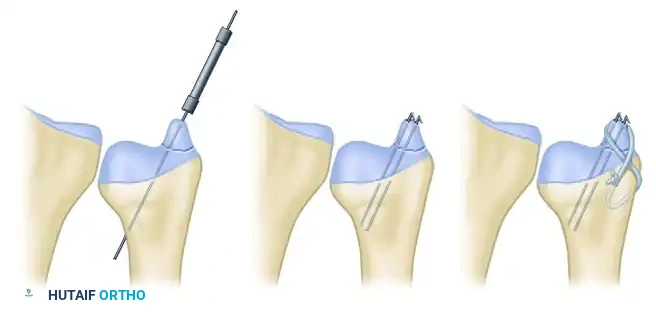
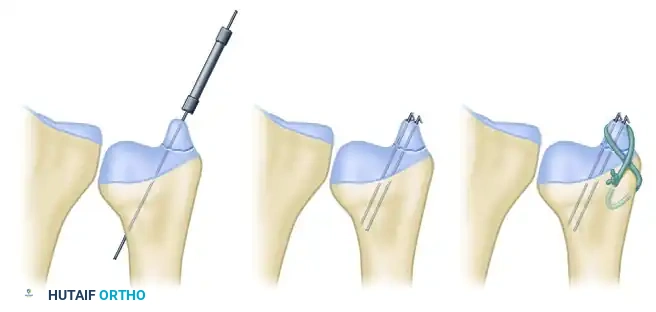
Ulnar Styloid Fractures
Ulnar styloid fractures occur in up to 60% of distal radius fractures. Base of styloid fractures are particularly concerning as they often represent an avulsion of the primary stabilizing components of the TFCC. If the DRUJ is unstable following fixation of the radius, the ulnar styloid should be addressed. Open reduction and internal fixation (ORIF) can be achieved via several techniques depending on fragment size:
* Lag Screw Fixation: Ideal for large, non-comminuted base fragments.
* Kirschner Wire Pinning: Useful for smaller fragments.
* Tension Band Wiring: Provides excellent biomechanical compression for transverse avulsion fractures.

Exhaustive Indications and Contraindications
Non-Operative Management and the Elderly Cohort
Stable fractures can be successfully treated with closed reduction and immobilization. The standard protocol involves initial stabilization with a well-padded sugar-tong splint to accommodate acute swelling, followed by conversion to a short-arm or long-arm cast once edema subsides. Weekly radiographic evaluation is mandatory for the first 3 weeks. Significant changes in radial length (shortening >3mm), palmar tilt (dorsal angulation >10 degrees from neutral), or loss of radial inclination should prompt immediate consideration of operative treatment.
In infirm and low-demand patients, closed treatment is often appropriate even in the presence of factors that would constitute absolute indications for operative treatment in younger, more active cohorts. In a prospective randomized trial comparing nonoperative treatment with volar locking plate fixation in 73 patients aged 65 years or older, Arora et al. found no significant differences in range of motion or level of pain at the 1-year follow-up. Although grip strength was objectively better in the operatively treated group, anatomical reconstruction did not improve the patients’ subjective ability to perform activities of daily living (ADLs). Similarly, Egol et al. demonstrated that minor limitations in wrist range of motion and diminished grip strength following nonoperative treatment did not limit functional recovery in a cohort of 90 patients older than 65 years.
Absolute and Relative Surgical Indications
The decision to proceed with operative intervention hinges on the inability to obtain or maintain an acceptable reduction via closed means. An acceptable reduction is generally defined as radial shortening of less than 3 mm, dorsal tilt of less than 10 degrees (or within 15 degrees of the contralateral uninjured wrist), and intra-articular step-off or gap of less than 2 mm.
Operative intervention is strongly indicated for high-energy shear injuries (Fernandez Type II), die-punch fractures (Fernandez Type III) with significant articular depression, and any fracture presenting with acute carpal tunnel syndrome that does not resolve immediately upon closed reduction. Open fractures require emergent surgical debridement and stabilization, typically utilizing external fixation or immediate internal fixation depending on the soft tissue envelope.
| Parameter | Indications for Operative Intervention | Contraindications / Non-Operative Indications |
|---|---|---|
| Articular Congruity | Intra-articular step-off or gap > 2 mm | Articular step-off < 1-2 mm |
| Radial Length | Shortening > 3-5 mm relative to the ulna | Shortening < 3 mm |
| Sagittal Alignment | Dorsal tilt > 10° or Volar tilt > 20° | Dorsal tilt < 10°, neutral, or normal volar tilt |
| Comminution | Severe dorsal/volar metaphyseal comminution | Minimal to no comminution |
| Soft Tissue | Open fractures, Acute compartment syndrome, Acute CTS | Intact soft tissue envelope, resolving neurovascular status |
| Patient Factors | High-demand, young, active patients | Elderly, low-demand, severe medical comorbidities |
| Associated Injuries | Galeazzi variant, unstable DRUJ, concomitant carpal fractures | Isolated injury with stable DRUJ |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and 3D Reconstruction
While standard posteroanterior (PA), lateral, and oblique radiographs are sufficient for diagnosing and managing simple extra-articular fractures, advanced imaging is indispensable for complex intra-articular patterns. A non-contrast Computed Tomography (CT) scan with 2D multiplanar reformats (coronal and sagittal) and 3D surface rendering is the gold standard for evaluating intra-articular comminution, identifying die-punch fragments, and assessing the integrity of the sigmoid notch.
CT imaging often reveals occult fracture lines extending into the diaphysis or subtle coronal splits of the lunate facet that are completely obscured on plain radiographs due to overlapping carpal bones. Traction radiographs, obtained under fluoroscopy in the emergency department or operating room, can also be highly beneficial for visualizing the primary fracture fragments by utilizing ligamentotaxis to pull the fragments out of their impacted positions.
Digital Templating and Implant Selection
Pre-operative digital templating is a critical step in surgical planning. Utilizing the contralateral uninjured wrist as a template allows the surgeon to accurately gauge the patient's native radial inclination, volar tilt, and ulnar variance. The surgeon must plan the surgical approach (volar vs. dorsal vs. fragment-specific), select the appropriate implant type (e.g., standard volar locking plate, variable-angle locking plate, fragment-specific hook plates), and anticipate the need for supplementary bone grafting or bone substitutes for large metaphyseal voids.
Patient Positioning and Operating Room Setup
The patient is positioned supine on the operating table with the affected extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The C-arm fluoroscope is typically positioned either parallel to the hand table (coming in from the foot or head of the bed) or perpendicular to the table, depending on surgeon preference.
The surgeon sits in the axilla, and the assistant sits opposite. The monitor must be placed in direct line of sight for the primary surgeon. Prior to inflation of the tourniquet, the arm is exsanguinated using an Esmarch bandage. A sterile tourniquet may be utilized for proximal extension if a combined approach or extensive diaphyseal exposure is anticipated.
Step-by-Step Surgical Approach and Fixation Technique
Closed Reduction and Percutaneous Pinning (CRPP)
Percutaneous pinning after closed reduction is a highly effective, minimally invasive technique useful for distal radial fractures exhibiting metaphyseal instability or simpler intra-articular displacement (e.g., 2-part sagittal splits). An anatomical reduction must be obtained first via closed manipulation (traction, palmar translation, and ulnar deviation). Kirschner wires (K-wires) do not reduce the fracture; they merely maintain the reduction by acting as internal splints.
Surgical Technique:
1. Positioning: The patient is positioned supine with the arm extended on a radiolucent hand table. Fluoroscopy is positioned parallel to the table.
2. Reduction: Longitudinal traction is applied, often utilizing finger traps. The fracture is disimpacted and reduced.
3. Styloid Pinning: The first pins (usually 1.6 mm / 0.062-inch K-wires) are placed percutaneously from the tip of the radial styloid, directed proximally and ulnarly across the fracture site into the intact medial radial metaphysis and diaphysis. Surgical Warning: The superficial branch of the radial nerve (SBRN) is highly vulnerable during radial styloid pin insertion. A mini-open technique—utilizing a small incision and blunt dissection down to the bone with a hemostat—is strongly recommended to protect the nerve and extensor tendons.
4. Lunate Facet Pinning: If the lunate facet is displaced, a separate pin can be driven from the dorso-ulnar aspect of the distal radius fragment into the proximal radial shaft.
5. Kapandji (Intrafocal) Technique: Intrafocal pins can be added to provide a direct dorsal buttress. A K-wire is introduced directly into the fracture hematoma dorsally, levered to reduce dorsal tilt, and driven into the intact volar cortex.
We generally use at least two to three pins and confirm adequate reduction on true anteroposterior and lateral fluoroscopic views. Splint or cast immobilization is strictly necessary after percutaneous pinning, as the pins alone cannot withstand physiological loads. Pins are typically removed in the clinic at 4 to 6 weeks postoperatively once clinical and radiographic union is evident.
The Volar Approach (Modified Henry) and Volar Locking Plate (VLP) Fixation
The volar approach has become the workhorse for the operative management of distal radius fractures. The Modified Henry approach exploits the internervous plane between the Flexor Carpi Radialis (FCR, median nerve) and the radial artery.
Surgical Technique:
1. Incision: A longitudinal incision is made directly over the FCR tendon, extending proximally from the wrist crease for approximately 8-10 cm.
2. Dissection: The FCR sheath is incised, and the tendon is retracted ulnarly, protecting the median nerve lying deep and ulnar to it. The superficial radial artery is identified and carefully retracted radially.
3. Deep Exposure: The flexor pollicis longus (FPL) tendon and the flexor digitorum profundus (FDP) tendons are retracted ulnarly to expose the pronator quadratus (PQ) muscle.
4. Pronator Quadratus Elevation: The PQ is incised along its most radial border (leaving a small cuff for later repair) and elevated subperiosteally from radial to ulnar, exposing the volar surface of the distal radius.
5. Fracture Reduction: The fracture hematoma is evacuated. Reduction is achieved utilizing manual traction, a periosteal elevator as a lever, or temporary K-wire fixation.
6. Plate Application: A Volar Locking Plate (VLP) is applied. The plate must be positioned proximal to the "watershed line" (the volar prominence of the distal radial metaphysis) to prevent attritional rupture of the flexor tendons, particularly the FPL.
7. Fixation: An oblong gliding hole in the diaphyseal segment is typically filled first to allow proximal-distal adjustment. Distal locking screws are then inserted to secure the articular fragments. Subchondral support is critical; screws should be placed 2-3 mm proximal to the articular surface.
Dorsal Plating and Fragment-Specific Fixation
While volar plating is preferred due to the generous soft tissue envelope, dorsal plating is strictly indicated for displaced dorsal shear fractures (dorsal Barton's), highly comminuted dorsal cortices that cannot be indirectly reduced, and complex intra-articular fractures requiring direct visualization of the joint surface.
The dorsal approach typically utilizes a longitudinal incision centered over Lister's tubercle. The extensor retinaculum is incised, typically over the third dorsal compartment, mobilizing the Extensor Pollicis Longus (EPL) tendon. The second and fourth compartments are elevated subperiosteally to expose the dorsal radius. Low-profile plates must be utilized to minimize tendon irritation. In complex, multi-fragmentary injuries, fragment-specific fixation utilizing small wire forms, hook plates, or mini-fragment screws allows customized buttressing of individual columns (e.g., radial styloid, dorsal ulnar corner).
Joint-Spanning External Fixation
External fixation relies on the principle of ligamentotaxis. By applying longitudinal traction across the radiocarpal joint, the intact volar and dorsal radiocarpal ligaments pull the fracture fragments into alignment. This technique is primarily indicated for highly comminuted, intra-articular fractures where internal fixation is impossible, or in the setting of severe open fractures with massive soft tissue compromise.
Standard spanning external fixation involves placing two 3.0 mm Schanz pins into the dorsal radial diaphysis and two 2.0 or 2.5 mm pins into the dorsal aspect of the second
Clinical & Radiographic Imaging Archive