Distraction Plate and Fragment-Specific Fixation of Distal Radius Fractures
Key Takeaway
Distraction plate fixation serves as a robust internal alternative to external fixators for highly comminuted distal radius fractures. By utilizing a dorsal spanning plate from the radius to the metacarpal, surgeons can maintain radial length and alignment while avoiding pin-tract infections. Combined with fragment-specific fixation techniques, this approach provides rigid stability, facilitates secondary bone grafting, and allows immediate postoperative digit mobilization for optimal functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The management of highly comminuted, intra-articular distal radius fractures presents a formidable challenge to the orthopedic surgeon, particularly in the presence of severe metaphyseal extension, extreme articular impaction, or profoundly osteopenic bone. Historically, external fixation was the gold standard for maintaining radial length and alignment through the principle of ligamentotaxis. By applying tension across the radiocarpal capsule and extrinsic ligaments, external frames could indirectly reduce major fracture fragments. However, external fixators are fraught with well-documented complications, including persistent pin-tract infections, superficial radial nerve irritation, pin loosening, and a high incidence of complex regional pain syndrome (CRPS) exacerbated by prolonged external tethering.
To circumvent these debilitating issues, modern operative orthopaedics has undergone a paradigm shift toward advanced internal fixation strategies. Two of the most significant advancements in this realm are Distraction Plate Fixation (the dorsal spanning plate) and Fragment-Specific Open Reduction and Internal Fixation (ORIF). These sophisticated techniques provide rigid, low-profile stabilization that bypasses the limitations of external frames. By utilizing the internal milieu, these constructs allow for immediate postoperative mobilization of the digits and facilitate secondary procedures, such as structural bone grafting, without the physical obstruction of an external apparatus.
The patho-epidemiology of these complex fractures typically follows a bimodal distribution. In young patients, high-energy trauma (such as motor vehicle collisions or falls from a significant height) drives the carpus into the distal radius, creating explosive intra-articular comminution and severe metaphyseal-diaphyseal dissociation. The energy transfer often results in a "die-punch" phenomenon, where the lunate is driven proximally into the lunate fossa, depressing the articular surface. Conversely, in the elderly population, low-energy falls onto an outstretched hand (FOOSH) in the setting of severe osteoporosis can result in equally devastating fracture patterns. The brittle, osteopenic bone shatters, leaving a void of structural support that renders standard volar locking plates inadequate due to a lack of distal purchase.
Before exploring these advanced salvage and reconstruction techniques, it is essential to understand the foundational approach to the distal radius, most commonly achieved via volar plating. Mastery of the standard volar approach provides the anatomical familiarity necessary to execute more complex fragment-specific and dorsal spanning interventions. The evolution of our understanding of distal radius morphology demands that surgeons possess a versatile armamentarium, seamlessly transitioning between volar, dorsal, and fragment-specific modalities based on the unique biomechanical demands of the fracture pattern.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the osteology and soft tissue envelope of the distal radius is paramount for executing complex reconstructions. The distal radius articulates with the scaphoid and lunate at the radiocarpal joint, and with the distal ulna at the sigmoid notch to form the distal radioulnar joint (DRUJ). Normal radiographic parameters dictate a radial inclination of approximately 22 degrees, a volar tilt of 11 degrees, and a radial height of 11 to 12 mm relative to the ulnar head. The volar cortex is relatively flat and thick, terminating distally at the "watershed line"—a critical anatomical landmark representing the most distal margin of the pronator quadratus fossa. Hardware placed distal to this line significantly increases the risk of flexor tendon attrition.
The soft tissue anatomy dictates our surgical approaches and influences the biomechanics of fixation. Volarly, the internervous plane lies between the flexor carpi radialis (FCR), innervated by the median nerve, and the radial artery. The pronator quadratus (PQ) muscle drapes transversely across the volar distal radius, serving as a natural protective barrier between the bone and the extrinsic flexor tendons. Dorsally, the anatomy is defined by the extensor retinaculum and its six distinct compartments. Lister's tubercle, a bony prominence on the dorsal cortex, acts as a pulley for the extensor pollicis longus (EPL) tendon (third compartment). The dorsal cortex is inherently thinner and more convex than the volar cortex, making it highly susceptible to comminution during hyperextension injuries.



The biomechanics of distraction plating rely entirely on the concept of internal ligamentotaxis. By securing a rigid plate to the stable radial diaphysis proximally and the rigid third metacarpal distally, the surgeon applies longitudinal traction. This tension is transmitted through the intact radiocarpal ligaments—specifically the radioscaphocapitate and long radiolunate ligaments—which pull the comminuted articular fragments out of their proximally impacted positions. Unlike external fixation, the internal spanning plate acts as a load-bearing device that shares physiological stresses, shielding the healing bone from bending and torsional forces while allowing unhindered excursion of the extrinsic tendons.
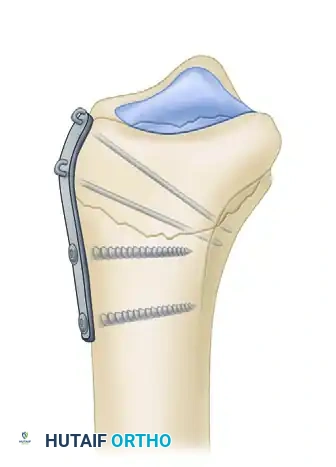
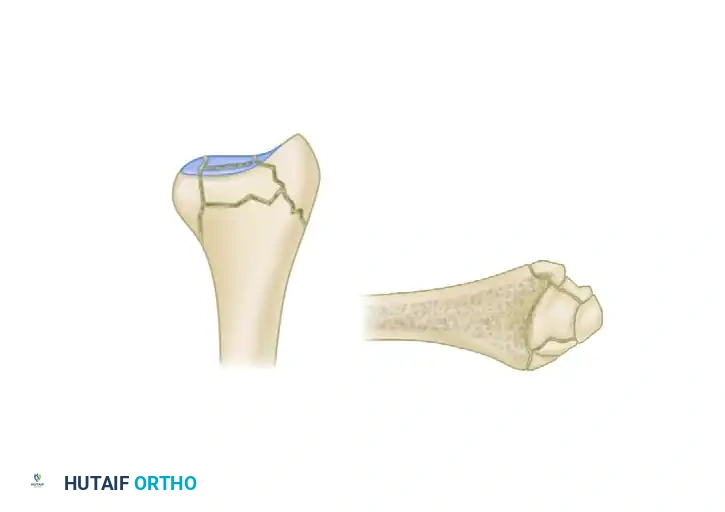
Conversely, the biomechanics of fragment-specific fixation are rooted in neutralizing forces at the individual fragment level. In severe injuries, the distal radius fails in a predictable pattern, yielding up to five distinct fragments: the radial styloid, the dorsal wall, the dorsal ulnar split, the volar rim, and the central articular fragment. Traditional Kirschner wire fixation provides only a single point of constraint, acting as a pivot that fails to prevent settling or radial drift under physiological loads. Fragment-specific pin-plate constructs transform this biomechanical environment by providing dual-point constraint. The pin captures the small fragment, while the attached buttress plate is secured to the intact radial shaft, effectively halting collapse, resisting dorsal torque, and neutralizing shear forces at the articular surface.

Exhaustive Indications and Contraindications
The decision to utilize a distraction plate versus a fragment-specific construct, or to abandon standard volar plating altogether, requires a nuanced understanding of the fracture personality and patient-specific factors. Distraction plating is primarily indicated in cases of massive metaphyseal bone loss or extreme intra-articular comminution where individual fragments are simply too small or osteoporotic to hold a screw. It is also the treatment of choice for polytraumatized patients who require immediate weight-bearing through their upper extremities for mobility (e.g., using crutches or a walker), as the rigid dorsal spanning construct can withstand these immense axial loads.
Fragment-specific fixation is indicated when discrete, critical articular fragments cannot be captured by a standard pre-contoured volar locking plate. The classic example is the "volar marginal rim" fracture (lunate facet), which, if left unaddressed, will lead to catastrophic volar subluxation of the entire carpus. Additionally, severe dorsal comminution involving the sigmoid notch (the dorsal ulnar split) often requires a dedicated dorsal or ulnar pin-plate to restore the congruity of the DRUJ. Fragment-specific techniques are highly modular, allowing the surgeon to build a customized construct tailored to the exact fracture morphology.
Contraindications for these advanced techniques must be strictly respected. Distraction plating is contraindicated in the presence of active local infection, pre-existing severe radiocarpal osteoarthritis (as the prolonged immobilization across a degenerative joint will lead to intractable stiffness), and in patients who are non-compliant, as the plate requires a mandatory secondary surgery for removal. Fragment-specific fixation is contraindicated when the bone is so severely pulverized that even low-profile pins cannot achieve purchase, or in low-demand, medically frail patients where a lengthy, complex reconstruction poses an unacceptable anesthetic risk.
| Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Volar Locking Plate | Extra-articular fractures, simple intra-articular patterns, reducible volar tilt. | Volar rim fractures too distal for plate purchase, massive dorsal comminution. | Severe osteopenia with metaphyseal voids. |
| Distraction (Spanning) Plate | Polytrauma requiring upper extremity weight-bearing, severe osteopenia, massive comminution, radiocarpal fracture-dislocations. | Active local infection, pre-existing radiocarpal arthritis, extreme non-compliance. | Complex regional pain syndrome (CRPS) history. |
| Fragment-Specific Fixation | Uncapturable volar rim fragments, dorsal ulnar splits, radial styloid escape, highly comminuted articular shear injuries. | Pulverized bone lacking pin purchase, medically unstable patients for prolonged surgery. | Severe soft tissue compromise over dorsal/ulnar aspects. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful complex distal radius reconstruction. Standard posteroanterior, lateral, and oblique radiographs are often insufficient to fully appreciate the degree of articular comminution and the spatial orientation of specific fragments. Therefore, a non-contrast computed tomography (CT) scan with 2-millimeter cuts, including 2D sagittal and coronal reformats as well as 3D surface-rendered reconstructions, is considered mandatory. The CT scan allows the surgeon to identify critical elements such as the size of the volar lunate facet, the presence of a central die-punch fragment, and the integrity of the sigmoid notch.
Digital templating is subsequently performed to determine the optimal implant strategy. For distraction plating, the surgeon must estimate the length of the 3.5-mm dynamic compression plate or dedicated spanning plate required. The plate must be long enough to secure at least three to four bicortical screws in the intact radial diaphysis proximally, span the comminuted segment and the radiocarpal joint, and secure three bicortical screws in the third metacarpal distally. Typically, a 12- to 16-hole plate is required. Anticipation of bone graft needs—whether autograft from the iliac crest, allograft, or synthetic bone substitutes—must be documented and prepared prior to the incision.
Patient positioning is critical for optimal fluoroscopic access and surgical ergonomics. The patient is positioned supine on the operating table with the affected arm extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. It is imperative that the hand table is completely radiolucent and free of underlying metal supports that could obscure fluoroscopic imaging. The C-arm is typically brought in parallel to the hand table, allowing the surgeon to obtain perfect posteroanterior and lateral views simply by rotating the patient's forearm, rather than maneuvering the heavy fluoroscopy machine.
Preparation and draping must allow for unhindered access from the elbow to the fingertips. The fingers are often placed in sterile Chinese finger traps suspended from a traction tower during the initial preparation to utilize gravity and ligamentotaxis for provisional reduction. A sterile tourniquet may be utilized if proximal extension of the incision is anticipated. The surgical team must ensure that all specialized equipment, including the fragment-specific implant trays, wire-bending tools, and bone grafting materials, are immediately available on the back table before the time-out is performed.
Step-by-Step Surgical Approach and Fixation Technique
Volar Plate Fixation: The Modified Henry Approach
While distraction plating is reserved for severe comminution, standard volar plate fixation remains the workhorse for the majority of displaced distal radius fractures. The volar approach utilizes the internervous plane between the flexor carpi radialis (FCR) and the radial artery, providing excellent exposure of the volar cortex while minimizing the risk of dorsal tendon irritation.
The patient is positioned supine with the arm extended on a hand table. A tourniquet is applied to the proximal arm and inflated after exsanguination. A longitudinal incision is made over the course of the FCR tendon, extending proximally from the wrist crease for approximately 8 to 10 centimeters, depending on the proximal extension of the fracture.
The incision is carried down through the subcutaneous tissue, taking care to identify and protect the palmar cutaneous branch of the median nerve, which typically lies ulnar to the FCR tendon. The FCR sheath is incised longitudinally. Rather than retracting the tendon radially, the tendon is retracted ulnarly. This maneuver is critical as it protects the median nerve, which lies immediately deep and ulnar to the FCR.
The floor of the FCR sheath is then incised to access the deep volar compartment. The flexor pollicis longus (FPL) muscle belly is identified. The FPL is partially detached or retracted ulnarly from the radius to expose the underlying pronator quadratus (PQ) muscle. Care must be taken during this deep dissection to avoid injury to the radial artery, which is gently retracted radially.
Using a Freer elevator or electrocautery, the pronator quadratus is elevated from its radial and distal insertions in an L-shaped fashion. The muscle is reflected ulnarly, exposing the volar cortex of the distal radius. It is vital to preserve the ulnar attachment of the PQ to facilitate later repair.
The fracture line is now fully exposed. The fracture hematoma is meticulously evacuated using a curette and irrigation. The fracture is reduced under direct vision and fluoroscopic guidance. Provisional reduction can be maintained with smooth Kirschner wires placed outside the planned footprint of the volar plate.
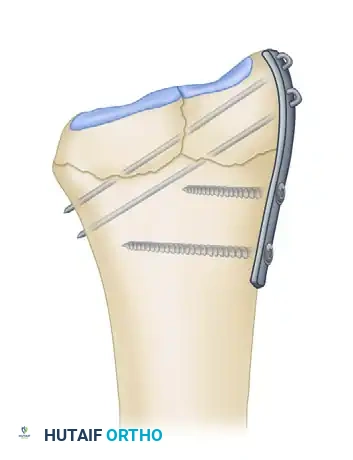
A pre-contoured volar locking plate is selected and positioned on the volar cortex. It is imperative that the plate is seated proximal to the watershed line to prevent future flexor tendon irritation. The first screw is inserted into the elongated gliding hole in the radial shaft. This allows for fine proximal-distal adjustments of the plate position before definitive fixation.

After confirming the restoration of volar tilt, radial inclination, and articular congruity via fluoroscopy, the distal locking screws are inserted. These screws must be placed just proximal to the subchondral bone to support the articular surface without penetrating the radiocarpal joint.
Once the distal articular block is secured, the remaining proximal diaphyseal screws are placed to finalize the construct. A final fluoroscopic check is performed in multiple planes, including a 20-degree elevated lateral view, to ensure no screws are protruding into the dorsal compartments or the radiocarpal joint.

Prior to closure, the pronator quadratus is meticulously repaired and sutured back to the edge of the brachioradialis or radial periosteum. This step is crucial as it covers the plate and protects the flexor tendons from mechanical attrition. The skin is closed with non-absorbable sutures.

Distraction Plate Fixation: Dorsal Spanning Technique
As an alternative to external fixation for highly comminuted fractures, Burke and Singer described the use of a distraction plate as an internal fixator. This technique was later modified and popularized by Ruch et al., who utilized a minimally invasive submuscular approach to minimize soft tissue stripping. The distraction plate relies on the principle of ligamentotaxis to restore radial length and alignment, avoiding external pin site problems and facilitating secondary bone grafting.
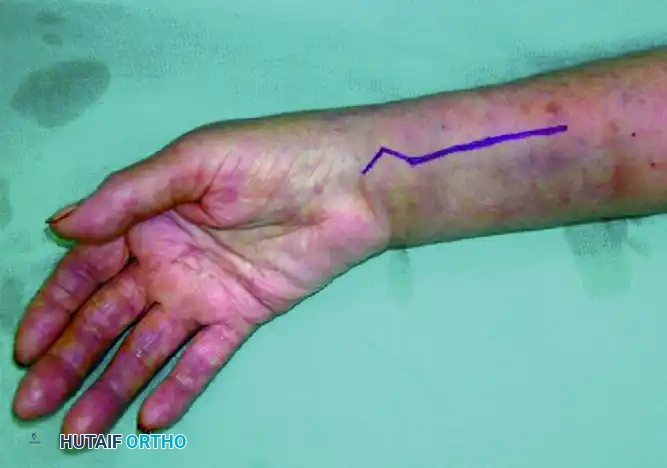
The Ruch modification utilizes three small incisions. The first is a 4-cm longitudinal incision over the dorsal aspect of the long finger (third) metacarpal shaft. The extensor tendon is retracted to expose the bone. The second is a 4-cm dorsal incision over the radial diaphysis, at least 4 cm proximal to the comminuted segment. The third is a 2-cm middle incision directly over Lister's tubercle, exposing the EPL tendon and allowing for direct visualization of the joint surface.
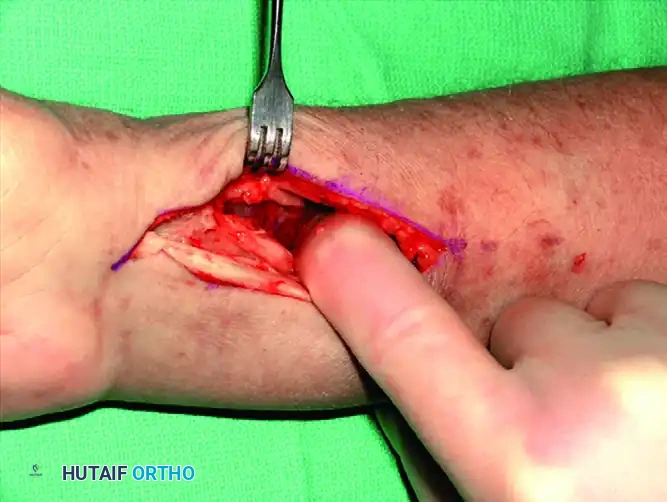
A 12- to 16-hole, 3.5-mm spanning plate is selected and passed submuscularly from the distal incision in a proximal direction. The plate must glide through the fourth dorsal compartment, sitting flat against the bone beneath the extensor tendons. The plate is first secured to the long finger metacarpal shaft using three bicortical 3.5-mm screws.
Under fluoroscopic guidance, longitudinal distal traction is applied to the fingers to obtain normal radial length via ligamentotaxis. With the hand held in approximately 0-10 degrees of extension and neutral rotation, the plate is secured to the proximal radius with a bone clamp. Once full forearm rotation is confirmed without impingement, the plate is secured to the radial shaft with three bicortical 3.5-mm screws.
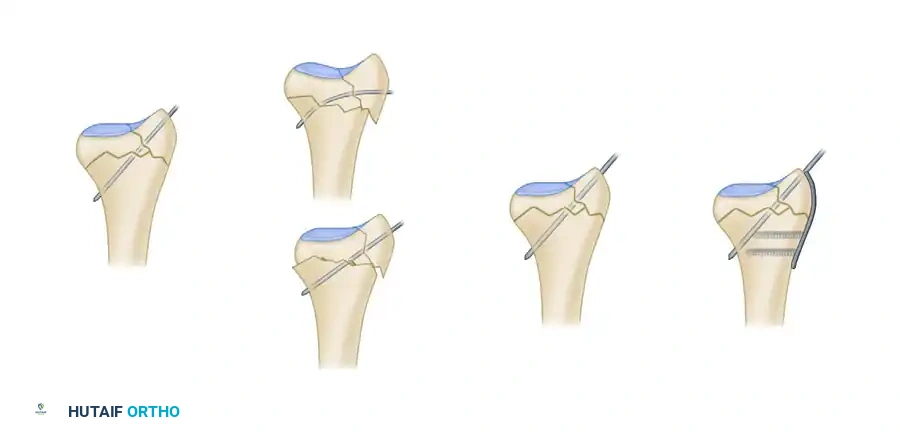
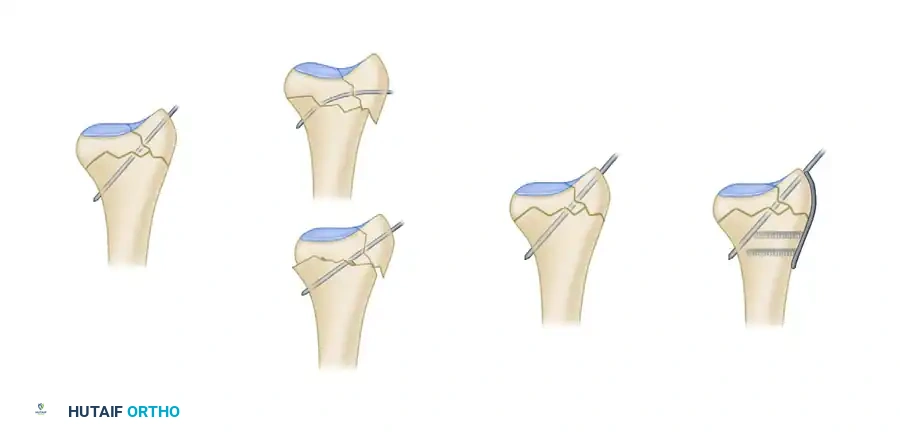
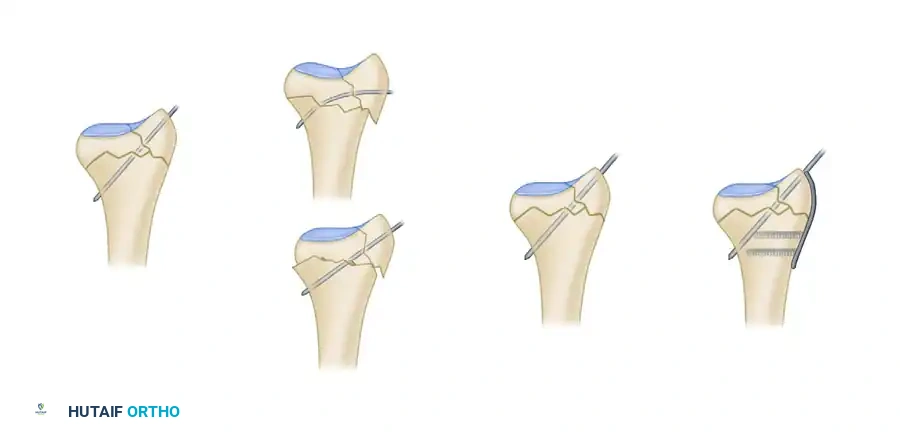
Adjunctive fixation is often necessary. The depressed lunate fossa can be elevated through the middle incision, and bone graft packed into the metaphyseal void. Kirschner wires can be percutaneously placed to stabilize specific articular fragments. The stability of the DRUJ must be assessed; if unstable, a sugar-tong splint is applied postoperatively.
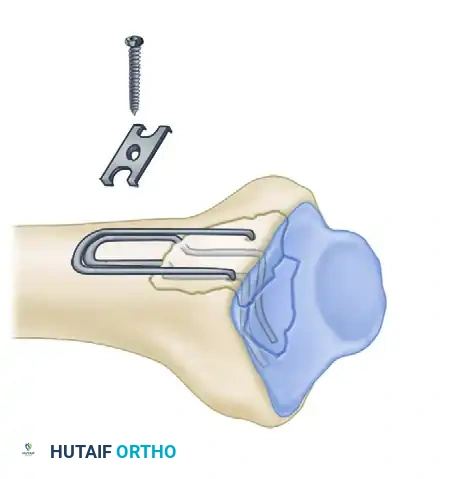
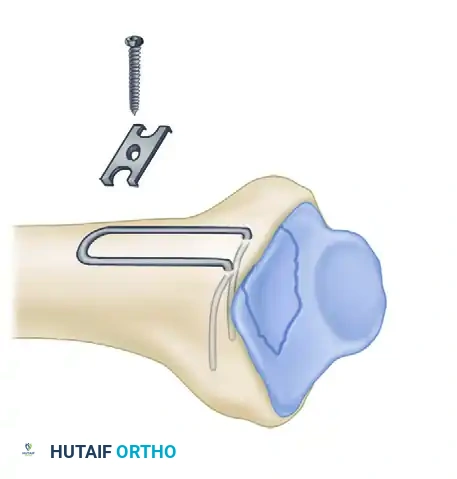
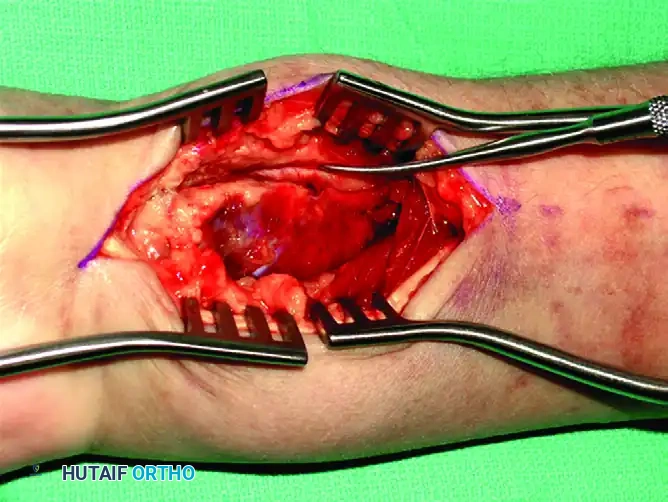
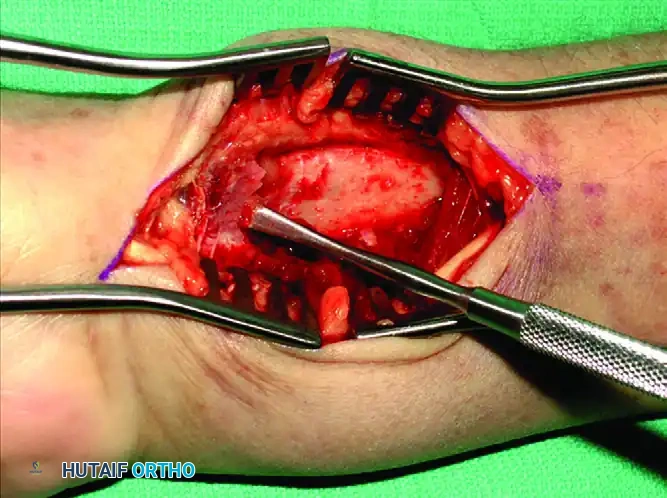
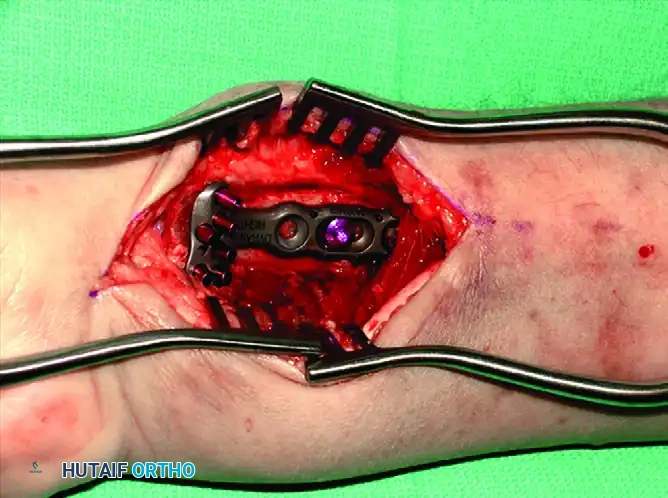
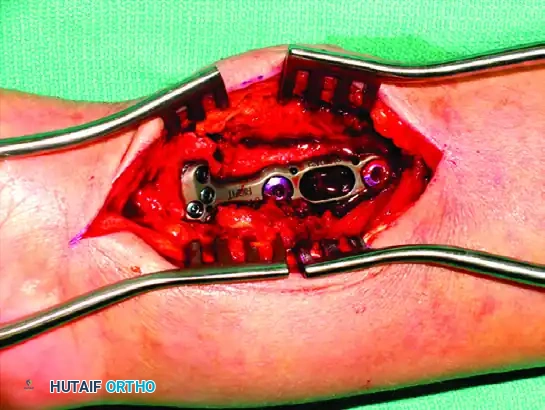
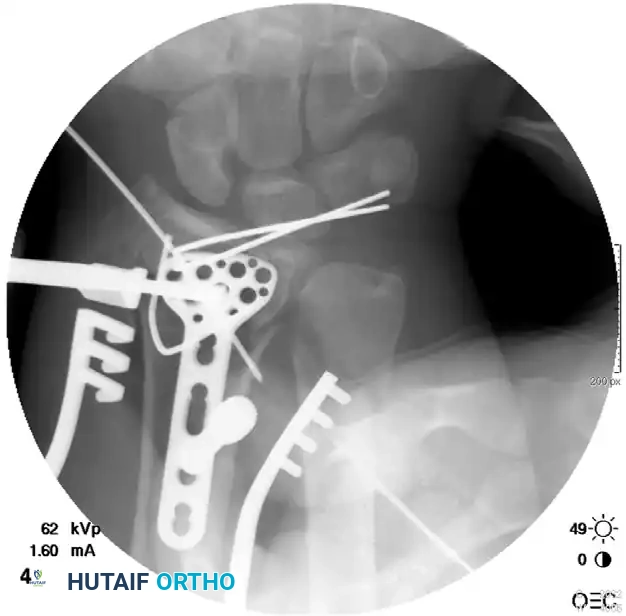
Postoperative Fixation with Distraction Plate Sequence:






Fragment-Specific Open Reduction and Internal Fixation
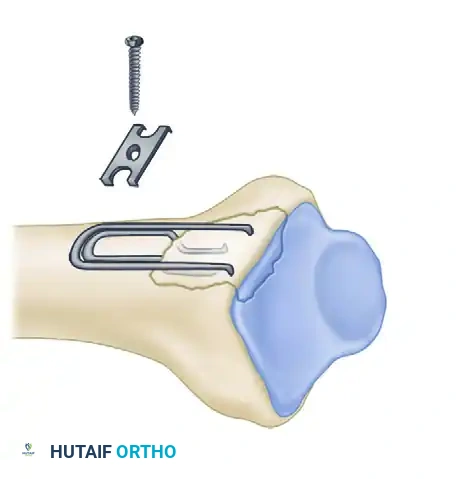
Recognizing the biomechanical pitfalls of standard constructs in highly comminuted osteopenic bone, Medoff developed a comprehensive fragment-specific wrist fixation system. This system combines the principles of pinning and plating to achieve stable reconstruction utilizing low-profile wire-forms and pin-plates.
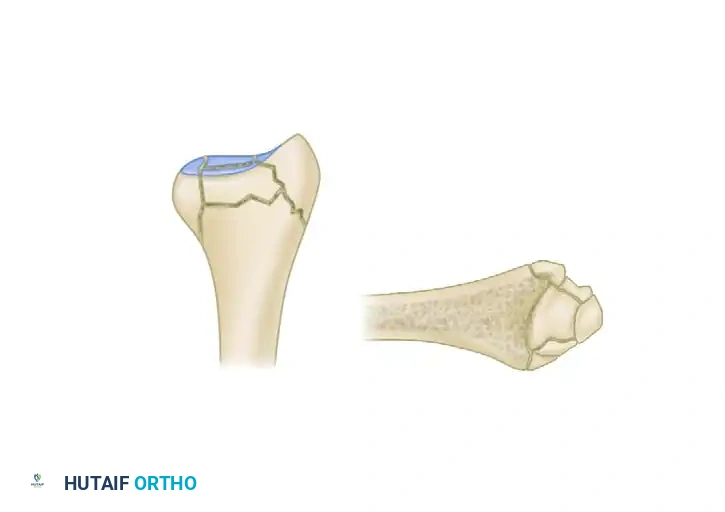
The distal radius typically fails in a predictable pattern, resulting in up to five distinct fragments:
1. Radial Column (Styloid)
2. Dorsal Cortical Wall
3
Clinical & Radiographic Imaging Archive