Closed Reduction and Percutaneous Pinning of Distal Radial Fractures: A Comprehensive Surgical Guide

Key Takeaway
Closed reduction and percutaneous pinning (CRPP) remains a cornerstone technique for managing specific distal radius fractures. This guide details the biomechanical principles, step-by-step surgical execution, and postoperative protocols for CRPP and external fixation. By mastering precise Kirschner wire placement and frame biomechanics, orthopedic surgeons can achieve stable anatomical reduction, minimize soft tissue compromise, and optimize functional recovery in appropriately selected patients.
Comprehensive Introduction and Patho-Epidemiology
Distal radius fractures (DRFs) represent one of the most ubiquitous osseous injuries encountered by the orthopedic surgeon, accounting for nearly one-sixth of all fractures treated in emergency departments globally. The patho-epidemiology of these injuries classically follows a bimodal distribution. In the younger, physiologically robust demographic, DRFs typically result from high-energy trauma, such as motor vehicle collisions, falls from significant heights, or athletic injuries, often presenting with complex intra-articular comminution and concomitant soft-tissue compromise. Conversely, in the elderly population, these fractures are predominantly fragility injuries secondary to low-energy falls from a standing height, deeply intertwined with the prevalence of osteoporosis and osteopenia. The fundamental deforming forces at play—axial loading combined with wrist hyperextension—dictate the classic fracture morphology, typically resulting in dorsal comminution, dorsal angulation (loss of volar tilt), radial shortening, and loss of radial inclination.
The historical evolution of distal radius fracture management is a testament to the dynamic nature of orthopedic surgery. For decades, cast immobilization was the solitary treatment modality, a paradigm established by Abraham Colles in the early 19th century. However, as the understanding of carpal kinematics and the long-term sequelae of malunion (e.g., post-traumatic radiocarpal arthrosis, midcarpal instability, and ulnar impaction syndrome) advanced, the necessity for anatomical restoration became paramount. While the advent and widespread adoption of volar locking plate (VLP) osteosynthesis over the past two decades have undeniably revolutionized the management of complex, comminuted, and osteoporotic fractures, Closed Reduction and Percutaneous Pinning (CRPP), frequently deployed alongside External Fixation, remains an indispensable, highly effective pillar of the orthopedic armamentarium.
The modern rationale for CRPP and external fixation is rooted in the principles of minimally invasive surgery and damage-control orthopedics. These techniques are profoundly advantageous for extra-articular fractures (AO/OTA Type 11A), simple intra-articular patterns without severe articular step-off (AO/OTA Type 11C1), pediatric physeal injuries, and highly specific scenarios involving severe soft-tissue compromise where extensive surgical dissection and periosteal stripping are strictly contraindicated. The primary objective of these percutaneous techniques is to restore and rigidly maintain radial height, volar tilt, radial inclination, and articular congruity while minimizing iatrogenic soft-tissue trauma, preserving the critical fracture hematoma, and mitigating the risk of devascularizing comminuted fracture fragments.
Furthermore, in an era increasingly scrutinized for healthcare economics and resource allocation, CRPP and external fixation offer a substantially more cost-effective profile compared to VLP osteosynthesis. The operative time is generally shorter, the implant costs are exponentially lower, and the hardware is routinely removed in the outpatient clinic, negating the need for a secondary formal surgical procedure for hardware removal. However, the success of this modality is entirely contingent upon meticulous patient selection, an exhaustive understanding of radiocarpal biomechanics, and the precise execution of surgical technique. If an anatomical or highly acceptable reduction cannot be achieved via closed means, or if severe metaphyseal comminution precludes stable pin purchase, the surgeon must be prepared to seamlessly pivot to alternative techniques such as Open Reduction and Internal Fixation (ORIF).
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the osseous, ligamentous, and neurovascular anatomy of the distal forearm is the absolute prerequisite for the safe and effective execution of CRPP and external fixation. The distal radius articulates with the proximal carpal row (scaphoid and lunate) via the radiocarpal joint, and with the distal ulna via the sigmoid notch at the distal radioulnar joint (DRUJ). Normal radiographic parameters of the distal radius are strictly defined: radial inclination averages 22 degrees (range, 13 to 30 degrees), volar tilt averages 11 degrees (range, 1 to 21 degrees), and radial height averages 11 to 12 mm relative to the distal ulnar articular surface. Ulnar variance should ideally be neutral, though it varies slightly with forearm rotation. Restoration of these exact parameters is critical; for instance, a residual dorsal tilt greater than 10 degrees significantly alters the load transmission across the radiocarpal joint, transferring pathological stress to the dorsal radiocarpal ligaments and the DRUJ, ultimately predisposing the patient to degenerative arthrosis and restricted flexion.
The ligamentous anatomy of the wrist is highly complex and serves as the biomechanical foundation for external fixation. The stout volar radiocarpal ligaments (radioscaphocapitate, long radiolunate, and short radiolunate) are intrinsically stronger and thicker than their dorsal counterparts. This anatomical discrepancy is the precise reason why the principle of ligamentotaxis—the application of longitudinal traction to realign fracture fragments via tensioning of intact ligaments—has inherent limitations. When longitudinal traction is applied across the wrist via a bridging external fixator, the strong volar ligaments reach maximal tension before the dorsal ligaments. Consequently, while linear traction effectively restores radial height and radial inclination, it typically fails to fully restore volar tilt, often leaving the distal articular fragment in a neutral or slightly dorsally angulated position. Recognizing this biomechanical limitation is crucial; it dictates the near-universal requirement for supplemental percutaneous Kirschner wire (K-wire) fixation to manually lever and secure the articular block into its anatomical volar tilt.
Neurovascular considerations during percutaneous pinning are paramount, with the Superficial Branch of the Radial Nerve (SRN) being the structure at highest risk for iatrogenic injury. The SRN emerges from beneath the brachioradialis approximately 9 cm proximal to the radial styloid, piercing the deep fascia to become subcutaneous. It then arborizes extensively over the first extensor compartment (containing the abductor pollicis longus and extensor pollicis brevis) to provide sensation to the dorsoradial aspect of the hand. Blind percutaneous pinning of the radial styloid carries an unacceptably high risk of impaling or wrapping the SRN around the K-wire, leading to a devastating and deeply debilitating neuroma. Therefore, a mini-open approach with blunt dissection down to the periosteum is an absolute surgical mandate for radial styloid pin placement.
Similarly, the extensor tendons traversing the dorsal aspect of the distal radius within their respective extensor retinacular compartments must be meticulously protected. The Extensor Pollicis Longus (EPL), residing in the third dorsal compartment and pivoting around Lister's tubercle, is particularly vulnerable to both iatrogenic injury from dorsal K-wires and delayed attritional rupture secondary to prominent hardware or fracture callus. Dorsal pins must be placed with precise fluoroscopic guidance to avoid intra-articular penetration and tendon transfixation. The biomechanical goal of the final construct—whether a combination of crossed K-wires or an external fixator augmented with pins—is to act as a neutralization frame. This frame must counteract the robust axial loads and deforming rotational forces generated by the physiological activity of the forearm musculature (e.g., brachioradialis, wrist flexors, and extensors) until provisional osseous union is achieved.
Exhaustive Indications and Contraindications
The decision to proceed with CRPP and/or external fixation versus open plating requires a nuanced analysis of fracture morphology, bone density, patient physiological age, and functional demands. The classical indication for CRPP is an extra-articular distal radius fracture (AO Type A) or a simple intra-articular fracture (AO Type C1) that is reducible by closed manipulation but inherently unstable, meaning it will inevitably displace if managed with cast immobilization alone. Instability criteria, often referred to as Lafontaine's criteria, include initial dorsal angulation greater than 20 degrees, dorsal comminution, radial shortening greater than 5 mm, intra-articular involvement, an associated ulnar fracture, and advanced patient age. The presence of three or more of these factors essentially guarantees loss of reduction in a cast, mandating surgical stabilization.
External fixation, often utilized as a spanning (bridging) construct across the radiocarpal joint, is particularly indicated in high-energy trauma scenarios characterized by severe intra-articular comminution (where the fracture fragments are too small to accept screws from a volar plate), gross radiocarpal instability, or extensive soft-tissue compromise. In the setting of open fractures with massive contamination or severe degloving injuries, external fixation adheres to the principles of damage-control orthopedics, providing rapid, rigid skeletal stabilization while allowing unimpeded access for serial soft-tissue debridement, vacuum-assisted closure, or eventual flap coverage. Furthermore, in the pediatric population, where the physes remain open, percutaneous pinning is the gold standard for displaced Salter-Harris fractures of the distal radius that cannot be maintained in a cast, as smooth K-wires minimize the risk of iatrogenic physeal arrest.
Conversely, absolute contraindications to CRPP and external fixation are primarily dictated by fracture patterns that cannot be adequately reduced or stabilized via indirect means. Volar shear fractures (Barton's fractures or AO Type B3) are inherently unstable due to the deforming pull of the strong volar radiocarpal ligaments and the flexor tendons; these obligatorily require volar buttress plating. Similarly, fractures with massive metaphyseal voids or severe osteopenia represent a relative contraindication, as the K-wires will lack sufficient cortical purchase (the "windshield wiper" effect), leading to inevitable pin loosening, loss of reduction, and late collapse. In such scenarios, VLP osteosynthesis, which relies on the fixed-angle stability of locking screws, is biomechanically superior.
Indications and Contraindications Reference Table
| Category | Specific Clinical Scenarios | Rationale / Biomechanical Consideration |
|---|---|---|
| Absolute Indications | - Reducible but unstable extra-articular fractures (AO Type A) - Displaced pediatric physeal fractures (Salter-Harris II) - Severe soft-tissue compromise (degloving, burns, open fractures) |
Prevents loss of reduction post-casting; avoids physeal arrest; allows wound access and avoids hardware in contaminated beds. |
| Relative Indications | - Simple intra-articular fractures (AO Type C1) - Polytrauma / Damage-control orthopedics - Highly comminuted fractures lacking bone stock for screws |
Minimally invasive; rapid application; relies on ligamentotaxis to maintain length when internal fixation is impossible. |
| Relative Contraindications | - Severe osteoporosis / osteopenia - Delayed presentation (> 3 weeks post-injury) - Non-compliance with post-operative pin care |
Poor cortical purchase leads to pin loosening and loss of reduction; early callus prevents closed reduction; high risk of pin tract infection. |
| Absolute Contraindications | - Volar shear fractures (Volar Barton's / AO Type B3) - Irreducible intra-articular step-off > 2mm - Complex multi-fragmentary articular fractures (AO Type C3) |
Requires rigid volar buttress to counteract flexor forces; indirect reduction cannot restore articular congruity; requires direct visualization (ORIF). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful surgical outcome in the percutaneous management of distal radius fractures. The evaluation begins with high-quality orthogonal radiographs of the injured wrist, including true posteroanterior (PA), lateral, and oblique projections. In cases of significant shortening or comminution, a traction radiograph can be invaluable; it temporarily negates the deforming muscle forces and provides a preview of the fracture's behavior under ligamentotaxis, helping the surgeon determine if closed reduction will be feasible. For any fracture with suspected intra-articular extension, a non-contrast Computed Tomography (CT) scan with sagittal and coronal reconstructions is highly recommended. The CT scan precisely delineates articular step-offs, gap formations, the presence of a die-punch fragment, and the integrity of the sigmoid notch, thereby dictating the precise trajectory required for percutaneous pins or indicating the need for open reduction.
Templating, while more commonly associated with arthroplasty or internal fixation, remains highly relevant for external fixation. The surgeon must assess the uninjured contralateral wrist clinically or radiographically to establish the patient's baseline ulnar variance and radial inclination, as restoring the patient's native anatomy is the ultimate goal. The selection of the external fixator frame (single-bar, double-bar, or radiolucent carbon fiber) and the appropriate diameter of half-pins (typically 3.0 mm for the metacarpal and 3.0 to 4.0 mm for the radius) should be finalized prior to entering the operating theater. Furthermore, the surgeon must anticipate the need for adjunctive procedures, such as carpal tunnel release for acute median nerve neuropathy, or the utilization of bone graft substitutes (e.g., calcium phosphate cement) to fill substantial metaphyseal defects and prevent late collapse.
The choice of anesthesia is a collaborative decision between the orthopedic surgeon, the anesthesiologist, and the patient. Regional anesthesia, specifically an ultrasound-guided supraclavicular or axillary brachial plexus block, is the preferred modality. It provides excellent intraoperative muscle relaxation—crucial for overcoming the deforming forces of the brachioradialis during closed reduction—and offers superior post-operative analgesia, significantly reducing the need for systemic opioids. General anesthesia is reserved for polytrauma patients, pediatric patients, or those with contraindications to regional blockade. In austere or resource-limited environments, a well-executed hematoma block combined with conscious sedation can serve as an effective alternative for isolated CRPP.
Patient positioning must facilitate unimpeded fluoroscopic access and ergonomic comfort for the surgical team. The patient is positioned supine on the operating table. The operative upper extremity is extended and supported on a radiolucent hand table. Standard sterile preparation and draping are performed from the fingertips to the mid-arm. A sterile pneumatic tourniquet is routinely applied to the proximal arm; however, for isolated CRPP or external fixation, it is rarely inflated unless a mini-open reduction or carpal tunnel release becomes necessary. The utilization of sterile finger traps applied to the thumb, index, and long fingers, suspended from an intravenous pole or a dedicated traction tower with 10 to 15 pounds of counterweight applied to the upper arm, is instrumental. This setup allows for sustained, fatigue-free longitudinal traction, facilitating disimpaction of the fracture fragments and establishing the foundation for ligamentotaxis prior to the commencement of formal surgical fixation.
Step-by-Step Surgical Approach and Fixation Technique
The execution of Closed Reduction and Percutaneous Pinning, with or without the addition of an external fixator, is a highly choreographed sequence of maneuvers that demands both tactile finesse and rigorous fluoroscopic vigilance.
Fracture Reduction Maneuvers
With the patient's digits secured in sterile finger traps and counter-traction applied to the upper arm, the fracture is allowed to disimpact under sustained longitudinal traction for 5 to 10 minutes. This critical pause overcomes the spasticity of the forearm musculature and maximizes the effect of ligamentotaxis.
Following this, the surgeon executes manual manipulation. For the classic dorsally displaced Colles-type fracture, the surgeon places both thumbs over the dorsal aspect of the distal radial fragment and the index/long fingers on the volar aspect of the proximal radial shaft. A combination of volar translation, ulnar deviation, and pronation is applied to the distal fragment to correct the dorsal tilt, radial translation, and supination deformity. The reduction is immediately evaluated via dynamic fluoroscopy in true AP and lateral planes. If anatomical or acceptable reduction is not achieved, the surgeon must abort the percutaneous plan and convert to ORIF.
The Radial Styloid Incision and Nerve Protection
Once reduction is provisionally achieved and held manually or via traction, the pinning sequence begins. A strict mini-open approach is mandatory for radial styloid pin placement. A 1.5-cm to 2.0-cm longitudinal incision is made centered over the tip of the radial styloid.
Using a fine hemostat, the subcutaneous tissues are bluntly spread. The surgeon must meticulously identify and mobilize the terminal sensory branches of the superficial radial nerve (SRN).
These delicate nerve branches are gently retracted using small Ragnell or Senn retractors. The first extensor compartment is identified, and the periosteum of the radial styloid is exposed. A drill guide or tissue protector is firmly seated against the bone to prevent the K-wire from skiving and to completely isolate the rotating wire from the adjacent soft tissues.
Step-by-Step Pinning Configurations
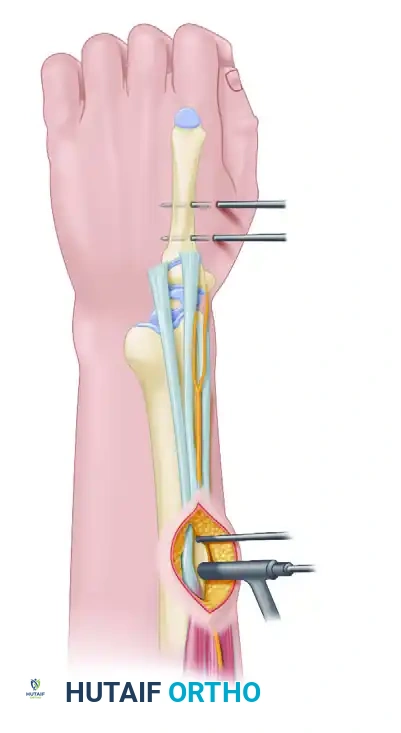
Typically, 1.6-mm (0.062-inch) smooth K-wires are utilized. The first pin is driven from the tip of the radial styloid, directed proximally and ulnarly, aiming to cross the fracture site and engage the thick cortical bone of the proximal ulnar aspect of the radial shaft. A second, parallel or slightly divergent pin is often placed from the styloid to increase rotational stability.
To achieve multiplanar biomechanical stability, an orthogonal dorsal pin is frequently required.

This pin is inserted through a separate micro-incision just distal to Lister's tubercle, taking great care to avoid the EPL tendon. It is driven in a proximal and volar direction to engage the intact volar cortex of the proximal radius.
In cases of severe metaphyseal comminution, alternative configurations such as crossed-pin constructs or Kapandji intrafocal pinning may be employed. The Kapandji technique involves driving K-wires directly into the fracture line and leveraging them against the intact cortex to buttress the distal fragment and restore volar tilt.

External Fixation Application
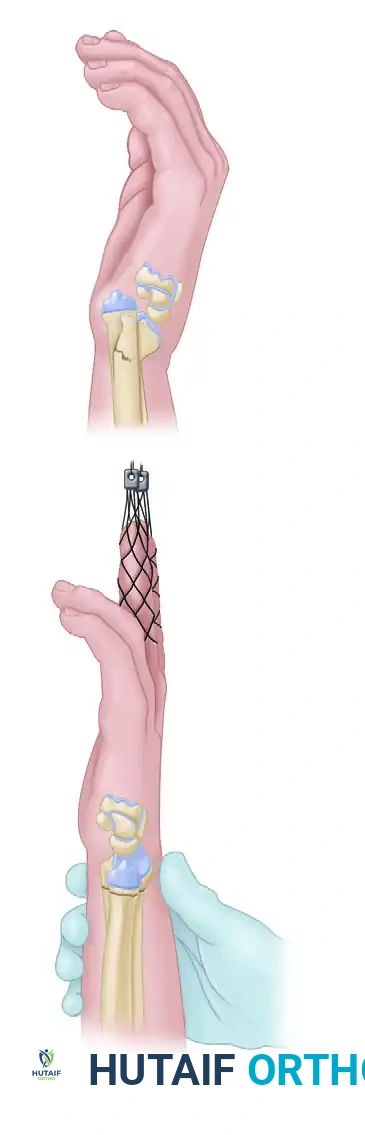
If an external fixator is indicated, the bridging technique is most commonly employed. Two 3.0-mm half-pins are inserted into the dorsoradial aspect of the second metacarpal via mini-open incisions, ensuring the extensor mechanism and dorsal interosseous muscles are protected. Next, two 3.0-mm or 4.0-mm half-pins are placed into the dorsoradial aspect of the radial shaft, approximately 10 cm proximal to the fracture site, carefully avoiding the SRN and the radial artery.

A carbon-fiber frame is assembled to connect the metacarpal and radial pin clusters. Traction is applied to the hand to achieve ligamentotaxis, and the clamps are rigidly locked.
Because linear traction rarely restores volar tilt completely, the external fixator is almost universally augmented with percutaneous K-wires (as described above) to directly manipulate and secure the articular fragments.

The external fixator thus acts primarily as a neutralization device to protect the delicate K-wire construct from the compressive forces of the forearm musculature.

Following final fluoroscopic confirmation of articular congruity and hardware placement, the K-wires are bent, cut, and left protruding through the skin to facilitate easy removal in the clinic. The incisions are closed with interrupted absorbable sutures, and a sterile, non-adherent dressing is applied, followed by a well-molded sugar-tong splint.
Complications, Incidence Rates, and Salvage Management
Despite the minimally invasive nature of CRPP and external fixation, the procedures are not without significant risks. The complication profile is distinct from that of volar locking plates, primarily revolving around the presence of percutaneous hardware and the reliance on indirect reduction techniques. The most ubiquitous complication is pin tract infection, which occurs in up to 20-30% of patients. Fortunately, the vast majority of these are superficial cellulitides that respond rapidly to a short course of oral antibiotics and enhanced local pin care. Deep osseous infections (osteomyelitis) are exceedingly rare but necessitate immediate hardware removal and formal surgical debridement.
Neurological complications, particularly iatrogenic injury to the Superficial Radial Nerve (SRN), represent a severe source of post-operative morbidity. SRN neuritis or neuroma formation can lead to debilitating chronic regional pain syndrome (CRPS) Type II. This underscores the absolute necessity of the mini-open approach for radial styloid pins. If a neuroma develops, conservative management with gabapentinoids and desensitization therapy is initiated; refractory cases may require surgical exploration, neuroma excision, and burying of the proximal nerve stump into the brachioradialis muscle belly.
Loss of reduction is another critical complication, predominantly seen in older patients with osteoporotic bone or in cases of unrecognized severe volar comminution. The K-wires may cut through the soft cancellous bone, leading to recurrent dorsal angulation and radial shortening. Tendon complications, including irritation, tenosynovitis, or frank rupture (most commonly the Extensor Pollicis Longus), occur due to direct abrasion against prominent dorsal K-wires or external fixator half-pins.
Salvage management for failed CRPP or external fixation depends strictly on the timing of the failure. Early loss of reduction (within the first 2-3 weeks) should be aggressively managed with a return to the operating room for conversion to Open Reduction and Internal Fixation (ORIF) with a volar locking plate and potential bone grafting. Late failures that progress to symptomatic malunion require complex reconstructive procedures. Extra-articular malunions with significant functional deficit are typically addressed with a corrective closing-wedge or opening-wedge osteotomy of the distal radius. If the malunion results in severe DRUJ incongruity and restricted forearm rotation, salvage procedures such as the Darrach procedure (distal ulnar resection) or the Sauvé-Kapandji procedure (DRUJ arthrodesis with proximal ulnar pseudoarthrosis) may be indicated to restore functional supination and pronation.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Pin Tract Infection | 15% - 30% | Inadequate pin care, excessive soft tissue motion around pins, prolonged fixation time. | Oral antibiotics (e.g., Cephalexin); increased frequency of chlorhexidine pin care; early pin removal if deep infection is suspected. |
| SRN Injury / Neuroma | 2% - 5% | Blind percutaneous pinning of radial styloid; aggressive retraction during mini-open approach. | Gabapentinoids; desensitization therapy; surgical neuroma excision and intra-muscular burying for refractory cases. |
| Loss of Reduction | 10% - 15% | Unrecognized severe comminution; osteoporotic bone ("windshield wiper" effect); premature pin removal. | Early (<3 weeks): Convert to VLP ORIF. Late (Malunion): Corrective distal radius osteotomy. |
| EPL Tendon Rupture | 1% - 3% | Iatrogenic transfixation by dorsal pins; attritional wear against prominent hardware or fracture callus. | Extensor Indicis Proprius (EIP) to Extensor Pollicis Longus (EPL) tendon transfer. |
| Complex Regional Pain Syndrome (CRPS) | 5% - 10% | Severe initial trauma; tight cast/splint; untreated nerve irritation; psychological factors. | Aggressive hand therapy; high-dose Vitamin C (controversial but low risk); sympathetic nerve blocks; multimodal pain management. |
Phased Post-Operative Rehabilitation Protocols
The surgical stabilization of a distal radius fracture is merely the first step in a continuum of care; meticulous, phased post-operative rehabilitation is absolutely vital to prevent debilitating joint stiffness, combat edema, and ensure optimal functional recovery. The rehabilitation protocol must be tailored to the stability of the fracture construct, the patient's bone quality, and their cognitive ability to comply with restrictions.
Phase 1: Immediate Post-Operative Immobilization (Weeks 0–2)
Immediately following surgery, the patient is placed in a bulky, well-molded sugar-tong splint. This splint immobilizes the wrist and strictly controls forearm supination and pronation, which is critical for minimizing rotational torque across the fracture site and preventing soft-tissue irritation at the pin-skin interfaces. The paramount goal during this acute inflammatory phase is edema control. Patients are rigorously instructed to maintain strict elevation of the operative extremity above the level of the heart. Active, full-excursion range of motion (ROM) exercises for the metacarpophalangeal (MCP) joints, interphalangeal joints, thumb, elbow, and shoulder are initiated on post-operative day one. Tendon gliding exercises are emphasized to prevent adhesions. Pin site care is instituted, typically involving daily cleansing with sterile saline or a dilute chlorhexidine solution, followed by the application of sterile, dry gauze to prevent maceration.
Phase 2: Transition and Provisional Mobilization (Weeks 2–6)
At the two-week post-operative mark, the patient returns to the clinic. The initial sugar-tong splint and any non-absorbable sutures are removed. Radiographs are obtained to verify the maintenance of reduction. If the construct is stable, the patient is transitioned to a short-arm cast or a custom-molded thermoplastic wrist splint fabricated by an occupational therapist. Crucially, this immobilization must stop proximal to the distal palmar crease to allow for completely unrestricted MCP joint flexion. Depending on the surgeon's assessment of fracture stability, gentle active ROM of the wrist may be initiated out of the splint under the strict supervision of a hand therapist, though passive stretching is strictly contraindicated at this stage. The K-wires and/or external fixator are typically removed in the outpatient clinic between 4 and 6 weeks post-operatively. The exact timing is dictated by the fracture pattern, patient age, and the radiographic appearance of bridging trabecular callus.
Phase 3: Aggressive Mobilization and Strengthening (Weeks 6–12+)
Following the removal of all percutaneous hardware and clinical confirmation of fracture stability (defined as the absence of focal tenderness over the fracture site), the patient enters the final phase of rehabilitation. The patient is transitioned to a removable wrist splint, worn primarily for protection during high-risk activities, in crowds, and at night for an additional 1 to 2 weeks. Supervised hand therapy is
