Volar Plate Fixation of Distal Radius Fractures

Key Takeaway
Volar plate fixation has become the gold standard for managing unstable, displaced distal radius fractures. Utilizing the flexor carpi radialis (FCR) approach, surgeons can achieve anatomic reduction and rigid internal fixation while minimizing dorsal tendon complications. This comprehensive guide details the step-by-step surgical technique, including pronator quadratus elevation, precise plate positioning, fluoroscopic evaluation, and postoperative rehabilitation protocols essential for optimal patient outcomes and restoration of wrist kinematics.
Comprehensive Introduction and Patho-Epidemiology
Fractures of the distal radius represent one of the most ubiquitous orthopedic injuries encountered in clinical practice, accounting for nearly one-sixth of all fractures treated in emergency departments. The patho-epidemiology of these fractures follows a classic bimodal distribution. In the younger demographic, these injuries are typically the sequelae of high-energy trauma—such as motor vehicle collisions, falls from significant heights, or high-impact athletic injuries—resulting in complex, intra-articular fracture patterns with substantial comminution, shear components, and concomitant soft-tissue trauma. Conversely, the elderly population typically sustains these fractures via low-energy mechanisms, predominantly a fall on an outstretched hand (FOOSH) from a standing height. In this osteoporotic cohort, the fracture patterns frequently present with apex-volar angulation, significant dorsal cortical comminution, and metaphyseal impaction.
Historically, the management of displaced distal radius fractures relied heavily on closed reduction and cast immobilization, or the utilization of first-generation dorsal plate designs intended to buttress the tension-sided dorsal cortex. However, these early dorsal plating techniques were fraught with unacceptable complication rates. The extensor tendons, lying in tight fibro-osseous compartments directly overlying the dorsal periosteum, were highly susceptible to hardware irritation, tenosynovitis, and delayed attritional rupture. Consequently, surgeons shifted toward external fixation and percutaneous pinning, though these modalities often failed to maintain articular congruity and volar tilt, particularly in the presence of severe osteopenia or extensive metaphyseal comminution.
The advent and subsequent refinement of fixed-angle volar plating techniques, driven by the development of angle-stable locking screws, revolutionized the operative management of distal radius fractures. Volar locking plates (VLPs) act fundamentally as internal fixators. By locking the screw heads into the plate, the construct provides rigid subchondral support to the articular surface without relying on plate-to-bone friction. This biomechanical advantage allows for the maintenance of reduction even in the presence of severe dorsal comminution and osteoporotic bone. By utilizing the volar approach, surgeons can exploit the relatively flat topography of the volar radius, allowing for thick soft-tissue coverage via the pronator quadratus, which effectively shields the flexor tendons from hardware prominence.
While dorsal plating retains a niche role—particularly with newer, low-profile, and fragment-specific designs for complex dorsal shear fractures—volar plate fixation remains the undisputed workhorse for the vast majority of displaced extra-articular and intra-articular distal radius fractures. The ability to achieve stable, rigid fixation that permits early active range of motion has fundamentally altered the rehabilitative trajectory for these patients, mitigating the stiffness and disuse osteopenia historically associated with prolonged cast immobilization.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the osseous and soft-tissue anatomy of the distal radius is paramount for successful surgical intervention. The distal radius is not a simple cylinder; it is a complex, multi-planar articular structure. Normal radiographic parameters dictate a radial inclination of 22 to 24 degrees, a radial height of 11 to 12 millimeters, and a volar tilt of 11 degrees. The articular surface is divided into the scaphoid fossa and the lunate fossa, separated by the interfossal ridge. Biomechanically, the radiocarpal joint transmits approximately 80% of axial loads across the wrist, with the lunate fossa bearing the highest stress concentration. Restoration of these precise anatomic relationships is critical to preserving normal radiocarpal and distal radioulnar joint (DRUJ) kinematics, thereby preventing post-traumatic osteoarthritis.
The "three-column theory" proposed by Rikli and Regazzoni provides a conceptual framework for understanding distal radius biomechanics and fracture fixation. The radial column (radial styloid and scaphoid fossa) acts as an osseous buttress against lateral carpal translation and provides an attachment site for the stout radioscaphocapitate and long radiolunate ligaments. The intermediate column (lunate fossa and sigmoid notch) is the primary load-bearing axis and is critical for DRUJ stability. The ulnar column (distal ulna, triangular fibrocartilage complex [TFCC], and DRUJ) serves as the axis around which forearm rotation occurs. Volar plating primarily addresses the intermediate and radial columns, utilizing fixed-angle subchondral pegs to support the lunate and scaphoid fossae, respectively.
The surgical anatomy of the volar approach is dictated by the modified Henry approach via the flexor carpi radialis (FCR) sheath. This approach utilizes the internervous plane between the radial artery (supplied by the radial nerve/artery axis) laterally, and the FCR tendon and median nerve (supplied by the median nerve) medially. Deep to the FCR sheath lies the flexor pollicis longus (FPL) muscle belly. Retracting the FPL ulnarly exposes the pronator quadratus (PQ) muscle, which originates on the distal ulna and inserts on the distal volar radius. The PQ serves as a critical anatomical landmark and a protective soft-tissue envelope.
A critical biomechanical and anatomical concept in volar plating is the "watershed line." This is a theoretical transverse ridge located at the most distal margin of the volar radius metaphysis, just proximal to the joint capsule attachment. The flexor tendons traverse directly over this ridge. If a volar plate is positioned distally to the watershed line, or if the plate design is excessively thick at its distal margin, the hardware will inevitably impinge upon the flexor tendons, most notably the FPL, leading to tenosynovitis and potentially catastrophic delayed tendon rupture. Therefore, meticulous plate positioning proximal to this line is a non-negotiable tenet of volar plate osteosynthesis.
Exhaustive Indications and Contraindications
The decision to proceed with operative fixation via volar plating must be individualized, synthesizing patient-specific factors (age, functional demands, bone quality, medical comorbidities) with fracture-specific characteristics. The overarching goal is to restore articular congruity, re-establish anatomic alignment, and permit early functional rehabilitation. Operative intervention is generally indicated when closed reduction cannot achieve or maintain acceptable radiographic parameters, as malunion inevitably alters carpal kinematics, restricts range of motion, and accelerates degenerative joint disease.
Loss of radial height greater than 3 millimeters is a critical indicator for surgery, as shortening significantly alters the load transmission across the ulnar carpus, leading to ulnocarpal impaction syndrome and DRUJ incongruity. Similarly, a loss of volar tilt (resulting in dorsal angulation greater than 10 degrees past neutral) shifts the center of rotation of the radiocarpal joint dorsally, increasing the load on the dorsal radiocarpal ligaments and the lunate, which precipitates midcarpal instability. Intra-articular step-offs greater than 2 millimeters are universally recognized as a harbinger of post-traumatic arthrosis and warrant meticulous open reduction and internal fixation.
Beyond radiographic parameters, clinical scenarios such as bilateral distal radius fractures, concomitant lower extremity polytrauma requiring the upper extremities for weight-bearing (e.g., crutch or walker use), and open fractures are absolute indications for stable internal fixation. However, surgeons must be equally cognizant of contraindications. Severe, active local infection precludes the placement of internal hardware. Furthermore, non-ambulatory patients with minimal functional demands, severe dementia, or prohibitive medical comorbidities may be better served with conservative management, accepting a radiographic malunion in favor of avoiding surgical morbidity.
| Category | Indications for Volar Plating | Contraindications for Volar Plating |
|---|---|---|
| Absolute | - Open fractures (after appropriate debridement) - Polytrauma requiring upper extremity weight-bearing - Acute carpal tunnel syndrome unresponsive to reduction - Concomitant neurovascular compromise |
- Active local soft-tissue or bone infection - Medically unstable patient (prohibitive anesthetic risk) - Critical soft-tissue compromise precluding closure |
| Relative | - Unstable extra-articular fractures (loss of volar tilt, radial shortening >3mm) - Displaced intra-articular fractures (step-off >2mm) - Metaphyseal comminution precluding cast maintenance - Bilateral distal radius fractures - Displaced volar shear (Barton's) fractures |
- Extremely low-demand, non-ambulatory patients - Severe cognitive impairment precluding rehab compliance - Highly comminuted dorsal shear fractures (may require dorsal approach) - Pediatric patients with open physes (relative to plate type) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a successful surgical outcome. Standard orthogonal imaging, including posteroanterior (PA), lateral, and oblique radiographs, is mandatory. The PA view assesses radial height, radial inclination, and ulnar variance. The lateral view is critical for evaluating volar tilt, dorsal comminution, and carpal alignment (assessing for dorsal or volar intercalated segment instability - DISI/VISI). Oblique views are particularly useful for profiling the radial styloid and assessing the dorsal ulnar corner of the radius. If closed reduction is performed in the emergency department, post-reduction films must be scrutinized to determine the inherent stability of the fracture pattern.
For all intra-articular fractures, and complex extra-articular patterns, a Computed Tomography (CT) scan is highly recommended, and arguably standard of care in modern academic practice. CT imaging with 2D sagittal and coronal reformats, along with 3D reconstructions, allows the surgeon to precisely map the fracture fragments. It is invaluable for identifying central die-punch fragments, assessing the integrity of the volar ulnar corner (the critical lunate facet fragment, which, if missed, can lead to catastrophic volar carpal subluxation), and planning the trajectory of fixed-angle screws. Digital templating should be utilized to estimate plate size, left/right specificity, and anticipated screw lengths, though intraoperative verification remains essential.
Patient positioning must be optimized for both surgical access and fluoroscopic imaging. The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded proximal arm tourniquet is applied to ensure a bloodless surgical field. The shoulder should be abducted to approximately 90 degrees, but care must be taken to avoid excessive traction on the brachial plexus. The hand is secured in a standardized fashion, often utilizing a lead hand or custom traction setup if ligamentotaxis is anticipated.
Fluoroscopy setup is a critical component of the preoperative phase. The mini C-arm can be brought in from the head of the bed or parallel to the hand table, depending on the surgeon's preference and operating room constraints. The monitor must be positioned directly in the surgeon's line of sight. Prior to incision, the surgeon should confirm that perfect PA, lateral, and multi-planar tangential views can be easily obtained without obstruction from the table hardware. Proper positioning and fluoroscopic readiness minimize operative time and reduce the risk of intraoperative technical errors.
Step-by-Step Surgical Approach and Fixation Technique
The FCR Approach and Deep Dissection
The operation commences with an 8-cm longitudinal incision over the volar forearm, centered precisely between the radial artery and the FCR tendon. To prevent postoperative scar contracture across the flexion crease, the incision can be modified distally into a V-shape or Brunner-type zigzag at the wrist crease, though it rarely needs to extend into the palm. Dissection is carried down to the FCR sheath, which is opened longitudinally. The FCR tendon is retracted ulnarly, protecting the median nerve. The deep fascial floor of the FCR sheath is then incised, exposing the underlying flexor pollicis longus (FPL) muscle belly. Using blunt dissection, the FPL is swept ulnarly. The space of Parona is entered, and the pronator quadratus (PQ) is visualized.
To elevate the PQ, an L-shaped incision is made along the extreme radial border of the radius and the distal metaphyseal flare. Using a periosteal elevator, the PQ is carefully lifted from the radius as a single, continuous flap and reflected ulnarly. This exposes the entire volar metaphysis and the fracture site.
Fracture Reduction Techniques
Fracture disimpaction is the critical next step. A Freer elevator or a small osteotome is inserted directly into the fracture line and advanced to the dorsal cortex, acting as a lever to disimpact the collapsed fragments. Direct manual pressure is applied to the dorsal cortex to reduce dorsally displaced fragments. In cases of significant radial styloid displacement, the brachioradialis muscle exerts a powerful proximal and radial deforming force. Fractionally lengthening or step-cutting the brachioradialis tendon near its insertion on the first dorsal compartment is often essential to neutralize this force and achieve anatomic reduction. Sustained longitudinal traction applied by an assistant (capsuloligamentotaxis) is typically utilized to maintain length and alignment during plate positioning.
Plate Application and Proximal Fixation
With the fracture provisionally reduced, the volar locking plate is positioned on the bone. The plate must sit proximal to the watershed line to prevent flexor tendon attrition. The first screw is inserted into the proximal oblong (gliding) hole using a 2.5-mm drill and a 3.5-mm cortical screw. This allows for fine-tuned proximal-distal adjustment. Mini C-arm fluoroscopy is utilized to confirm that the plate is centered on the radial shaft and properly aligned with the articular surface.
Distal Articular Fixation and the 2-Millimeter Rule
Once plate position is finalized, the distal subchondral holes are drilled using a 2.0-mm drill bit through the locking guides. The holes are measured for screw length.
Critical Step: The surgeon must insert locking screws that are exactly 2 mm shorter than the measured length. This intentional undersizing is a non-negotiable safety measure to prevent prominent distal screws from perforating the dorsal cortex, which is the leading cause of iatrogenic extensor pollicis longus (EPL) delayed rupture.



Standard PA and lateral fluoroscopy will NOT reliably show intra-articular screw penetration due to the concave nature of the articular surface. The surgeon must obtain tangential views (e.g., 20-degree elevated lateral, and varying degrees of tilt) to definitively rule out intra-articular penetration. Once the distal row is secured, the remaining proximal shaft holes are filled.
Management of the Distal Radioulnar Joint (DRUJ)
Following rigid fixation of the radius, the DRUJ must be assessed for stability throughout a full arc of forearm rotation. If the DRUJ is grossly unstable and an ulnar styloid base fracture is present, surgical intervention is warranted. The ulnar styloid can be fixed with percutaneous K-wires or a tension band construct. If the styloid fragment is comminuted, the peripheral rim of the TFCC is anchored directly to the ulnar fovea using transosseous sutures or a suture anchor.
Adjunctive Technique: Augmented External Fixation
In highly comminuted extra-articular fractures or cases with severe soft-tissue compromise where internal plating is insufficient or contraindicated, external fixation augmented with percutaneous pinning is employed. K-wires (0.045-inch or 0.0625-inch) are introduced into the fracture fragments in a crossed-pin configuration to provide torsional stability.

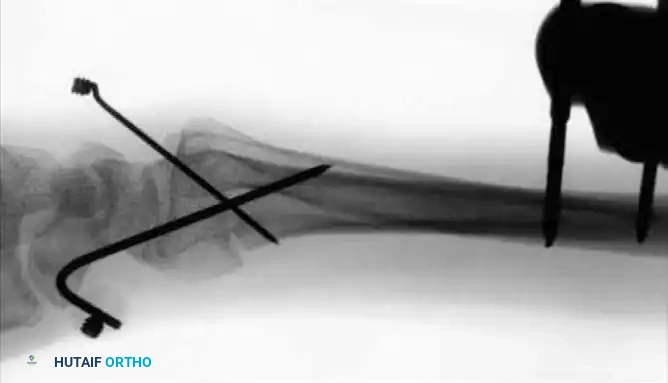
The external fixator frame is then applied using the distal pins as "joysticks" to restore volar tilt and radial length before locking the frame. Modern fixators feature clamps designed to integrate these augmenting K-wires directly into the construct.

Closure involves thorough irrigation and the reattachment of the PQ over the plate using braided absorbable sutures. While the PQ often cannot cover the entire plate due to swelling, priority is given to covering the distal portion to minimize flexor tendon contact.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates of volar plate fixation, complications do occur and can be broadly categorized into tendon-related, hardware-related, and biologic failures. Tendon complications are the most frequently reported. Flexor tendon irritation and rupture, particularly of the FPL, occur with an incidence of 2-12%. This is almost exclusively secondary to plate placement distal to the watershed line or the use of excessively thick plates. Extensor tendon rupture, most commonly the EPL, occurs in approximately 3-8% of cases and is typically caused by dorsal screw penetration.
Hardware failure, including screw back-out, plate breakage, or loss of fixation, is relatively rare with modern locking plates but can occur in severely osteoporotic bone or in cases of unrecognized dorsal comminution where the subchondral pegs fail to adequately support the articular surface. Intra-articular screw penetration is a devastating complication that leads to rapid chondrolysis and post-traumatic arthritis; meticulous utilization of tangential fluoroscopic views is the only reliable method for prevention.
Complex Regional Pain Syndrome (CRPS) is a severe biologic complication characterized by out-of-proportion pain, autonomic dysfunction, and severe stiffness, occurring in up to 10% of patients. Prophylactic administration of Vitamin C (500 mg daily for 50 days post-injury) has been suggested in the literature to reduce the incidence of CRPS, though evidence remains mixed. Early recognition and aggressive multimodal pain management, combined with intensive hand therapy, are critical for salvage.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| FPL Rupture | 2% - 12% | Strict plate placement proximal to the watershed line; meticulous PQ repair. | Hardware removal; tendon transfer (e.g., FDS of ring finger to FPL) or tendon grafting. |
| EPL Rupture | 3% - 8% | Undersize distal screws by exactly 2 mm; avoid prominent dorsal hardware. | Hardware removal; Extensor Indicis Proprius (EIP) to EPL tendon transfer. |
| Intra-articular Penetration | 1% - 4% | Mandatory use of 20-degree elevated lateral and multi-planar tangential fluoroscopy. | Immediate intraoperative screw exchange; if delayed, hardware removal and possible salvage arthrodesis if arthritis is advanced. |
| CRPS | 5% - 10% | Gentle tissue handling; avoid excessive traction; consider Vitamin C prophylaxis; early active ROM. | Aggressive hand therapy; gabapentinoids; sympathetic nerve blocks; pain management consultation. |
Phased Post-Operative Rehabilitation Protocols
The primary advantage of rigid volar plate fixation is the ability to institute early active range of motion, thereby mitigating the severe stiffness associated with historical casting techniques. The rehabilitation protocol must be phased and tailored to the individual patient's fracture stability, bone quality, and compliance.
Phase 1: Acute Healing (0–2 Weeks)
Immediately postoperatively, the wrist is immobilized in a bulky, compressive dressing and a volar resting splint to control edema. The patient is instructed to keep the extremity elevated above the level of the heart. Immediate, aggressive active range of motion (ROM) of the fingers (full composite flexion and extension), elbow, and shoulder is highly encouraged. Digit stiffness is a common and debilitating complication; ensuring full tendon excursion early prevents adhesions.
Phase 2: Early Motion (2–6 Weeks)
At the first postoperative visit (typically 10-14 days), sutures are removed. If the surgeon is confident in the rigid stability of the fixed-angle construct, the bulky splint is discontinued. The patient is transitioned to a custom-molded, removable Orthoplast splint. Active wrist flexion, extension, pronation, and supination are initiated. The splint is worn between exercise sessions and at night for protection. Passive stretching is generally avoided during this phase to prevent stressing the hardware-bone interface.
Phase 3: Strengthening and Maturation (6–12 Weeks)
By 6 weeks, radiographic evidence of early callus formation and clinical stability is typically present. The removable splint is discontinued entirely. Progressive strengthening exercises, encompassing grip strengthening and loaded wrist ROM, are initiated. Most patients succeed with a self-directed home exercise program; however, patients exhibiting guarding, severe stiffness, or early signs of CRPS require intensive, supervised hand therapy two to three times per week.
External Fixation Protocol
For patients managed with adjunctive external fixation, the protocol is necessarily modified. The wrist remains immobilized in a supinated position with a sugar-tong splint for the first 10 days to promote DRUJ stability. From 10 days to 6 weeks, active and passive finger motion is mandatory, and forearm rotation is initiated. The external fixator frame is typically removed in the clinic at 6 weeks. Supplemental K-wires are retained for an additional 2 weeks and removed at 8 weeks. Supervised hand therapy is strongly recommended following frame removal to restore terminal wrist arcs.
Summary of Landmark Literature and Clinical Guidelines
The evolution of distal radius fracture management is deeply rooted in robust clinical literature. The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines provide a strong recommendation for operative fixation of fractures with post-reduction radial shortening >3 mm, dorsal tilt >10 degrees, or intra-articular step-off >2 mm.
The seminal work by Orbay and Fernandez (2002) fundamentally shifted the paradigm toward volar fixed-angle plating. Their research demonstrated that the volar approach, utilizing the distal radius's flat volar topography and the protective envelope of the pronator quadratus, provided superior biomechanical stability and dramatically lower tendon complication rates compared to dorsal plating. They established the concept of the volar plate acting as an internal fixator, capable of supporting the dorsal subchondral bone even in the presence of severe comminution.
Further literature has refined our understanding of indications, particularly in the elderly. Studies by Arora et al. and Chung et al. have compared volar plating to cast immobilization in patients over 65 years of age. While volar plating provides superior early functional recovery and radiographic alignment, these studies suggest that at 12 months post-injury, functional outcomes (DASH scores) may equilibrate between operative and non-operative groups in low-demand elderly patients, despite persistent radiographic malunion in the casted cohorts. This highlights the necessity of individualized patient selection, weighing the immediate benefits of early mobilization against the inherent risks of surgical intervention.
Finally, the biomechanical studies defining the "watershed line" by Prommersberger and others have become foundational to surgical technique. Adherence to these anatomically driven guidelines has significantly reduced the incidence of iatrogenic flexor tendon ruptures, cementing volar plating as the gold standard in modern orthopedic trauma surgery.
