Distal Radius and Galeazzi Fractures: Principles of Operative Management
Key Takeaway
Distal radius fractures account for nearly 20% of all emergency department fractures. While historical management relied heavily on closed reduction, modern orthopedic surgery emphasizes precise anatomical restoration, particularly in high-demand patients. This guide details the biomechanics, radiographic parameters, and operative techniques for distal radius and Galeazzi fracture-dislocations, providing an evidence-based algorithm for rigid internal fixation and distal radioulnar joint (DRUJ) stabilization.
Comprehensive Introduction and Patho-Epidemiology
"…will at some remote period again enjoy perfect freedom in all of its motions and be completely exempt from pain."
— Abraham Colles, 1814
The management of distal radius fractures has evolved significantly since Abraham Colles’ optimistic proclamation in the early 19th century. Today, distal radius fractures represent one of the most ubiquitous orthopedic injuries, accounting for up to 20% of all fractures treated in emergency departments and encompassing nearly one-sixth of all fractures evaluated by orthopedic surgeons. Despite Colles' historical assertion of universal recovery, modern clinical follow-ups and rigorous outcomes research reveal that a substantial proportion of patients are not "completely exempt from pain" or functional limitation following treatment. The paradigm of treatment has therefore undergone a massive shift over the last three decades, transitioning from primarily closed reduction and cast immobilization to sophisticated, anatomically contoured internal fixation strategies.
In recent years, more than 1,000 peer-reviewed studies have been published regarding the optimal management of these injuries, yet absolute consensus remains elusive. Treatment algorithms are frequently complicated by confounding variables, including the required degree of anatomical restoration, inherent bone quality, the continuous emergence of novel fixation devices, surgeon experience, and the varying functional demands of aging populations. The desire for precise anatomical restoration of the radiocarpal and distal radioulnar joints is the primary rationale for operative intervention, driven by the understanding that articular incongruity and malalignment directly correlate with post-traumatic arthrosis and diminished grip strength.
Patient populations present in a distinctly bimodal distribution, which fundamentally dictates the patho-epidemiological approach to treatment. The first peak occurs in young, high-demand patients, typically males in their second or third decade of life. These individuals usually sustain high-energy trauma, such as motor vehicle collisions or falls from a significant height, resulting in complex, intra-articular, and highly comminuted fractures. In this cohort, restoration of distal radial anatomy is universally considered essential to minimize the devastating complications of post-traumatic radiocarpal arthrosis, carpal instability, and long-term vocational impairment. The energy of the injury often leads to concomitant soft tissue disruptions, including interosseous ligament tears and triangular fibrocartilage complex (TFCC) avulsions, requiring a comprehensive reconstructive approach.
The second, and vastly larger, demographic peak consists of elderly, low-demand patients, predominantly post-menopausal females. These patients typically sustain low-energy fragility fractures secondary to osteopenia or severe osteoporosis. Multiple recent reports indicate that older, lower-demand patients tend to tolerate radiographic incongruity, deformity, and malunion surprisingly well compared to their younger counterparts. However, nonoperative management in the elderly is not entirely benign. Studies have noted that among elderly patients treated nonoperatively with unacceptable radiographic parameters, over a quarter still reported significant functional impairment and chronic pain. While it is established that elderly patients tolerate more displacement than younger cohorts, identifying precisely which elderly patients would benefit from operative anatomical restoration remains a topic of active debate, heavily influenced by the patient's physiological age, baseline activity level, and the structural integrity of the osteoporotic bone.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the osseous architecture and ligamentous anatomy of the distal radius and distal radioulnar joint (DRUJ) is the cornerstone of successful operative management. The distal radius is conceptualized biomechanically as a three-column structure: the radial column (comprising the radial styloid and scaphoid facet), the intermediate column (comprising the lunate facet and sigmoid notch), and the ulnar column (comprising the distal ulna and TFCC). The intermediate column is particularly critical, as it bears the majority of axial loads transmitted across the radiocarpal joint. The volar surface of the distal radius is relatively flat but features a distinct distal ridge known as the "watershed line." This anatomical landmark is of paramount surgical importance; hardware placed distal to this line poses a severe risk of flexor tendon irritation, attrition, and eventual rupture, most notably involving the flexor pollicis longus (FPL).
The articular surface of the distal radius normally exhibits an ulnar inclination of approximately 21 to 23 degrees and a volar tilt of 11 to 12 degrees. Radial height, measured from the tip of the radial styloid to the lunate facet, averages 11 to 12 mm. Biomechanically, the radiocarpal joint transmits approximately 80% of axial compressive forces across the wrist, while the ulnocarpal articulation transmits the remaining 20%. Any alteration in these radiographic parameters drastically shifts this load distribution. For instance, a residual dorsal tilt of merely 20 degrees redistributes up to 50% of the axial load onto the distal ulna and TFCC, leading to ulnocarpal abutment syndrome, DRUJ instability, and accelerated degenerative joint disease. Furthermore, radial shortening alters the kinematics of the proximal carpal row, leading to a compensatory midcarpal supination deformity and secondary carpal instability.
The distal radioulnar joint (DRUJ) is a highly complex, inherently unstable articulation that relies heavily on extrinsic soft tissue stabilizers for its integrity. The osseous architecture of the shallow sigmoid notch provides minimal constraint against translation. The primary stabilizer of the DRUJ is the triangular fibrocartilage complex (TFCC), specifically the deep radioulnar ligaments (ligamentum subcruentum) that insert into the fovea at the base of the ulnar styloid. Secondary stabilizers include the pronator quadratus, the extensor carpi ulnaris (ECU) tendon subsheath, and the interosseous membrane. Disruption of these structures, as seen in Galeazzi fracture-dislocations, results in profound mechanical instability of the forearm axis.
Galeazzi fractures are classified based on the direction of radial displacement, which is dictated by the biomechanics of the forearm at the moment of axial loading. This mechanistic understanding is crucial for intraoperative reduction maneuvers.
Mechanism of Injury and Classification
Type I (Apex Volar):
Caused by axial loading of the forearm in supination. This mechanism results in the dorsal displacement of the distal radius fragment and a corresponding volar dislocation of the distal ulna. The deforming forces of the brachioradialis and pronator quadratus exacerbate the angular deformity.
Type II (Apex Dorsal):
Caused by axial loading of the forearm in pronation. This results in the anterior (volar) displacement of the distal radius fragment and a dorsal dislocation of the distal ulna. This is the more common variant and requires careful intraoperative assessment of the dorsal stabilizing structures of the DRUJ.
Exhaustive Indications and Contraindications
A constant theme in contemporary orthopedic literature is that the specific surgical technique (e.g., closed reduction and percutaneous pinning, external fixation, dorsal plating, volar locked plating, or intramedullary nailing) is secondary in importance to the actual attainment and maintenance of anatomical reduction. Operative intervention is indicated when closed reduction fails to achieve or maintain acceptable radiographic parameters, or when the injury pattern is inherently unstable. The threshold for surgical intervention is significantly lower in young, high-demand patients compared to low-demand, elderly individuals.
The standard radiographic parameters that dictate the thresholds for acceptable reduction include: Ulnar Variance (acceptable is no more than 2 mm of shortening relative to the ulnar head); Radial Height (acceptable is within 2 to 3 mm of the contralateral normal wrist); Palmar Tilt (acceptable is neutral 0 degrees, as dorsal angulation is poorly tolerated); Radial Inclination (acceptable is no less than 10 degrees); and Intra-articular Step or Gap (acceptable is less than 2 mm). Even 1 mm of articular incongruity in the radiocarpal joint has been associated with a significantly increased risk of post-traumatic arthrosis in high-demand patients. When closed reduction cannot achieve these strict parameters, operative intervention is strongly indicated.
For Galeazzi fracture-dislocations, nonoperative management is universally condemned in the adult population. Historically termed the "fracture of necessity," adult Galeazzi fractures cannot be managed conservatively. Closed treatment inevitably leads to loss of reduction, malunion of the radius, and chronic, painful instability of the DRUJ due to the relentless deforming forces of the forearm musculature. Therefore, the presence of a Galeazzi fracture is an absolute indication for open reduction and internal fixation of the radius, followed by systematic evaluation and stabilization of the DRUJ.
Contraindications to operative intervention, while few, must be rigorously respected to avoid catastrophic complications. Absolute contraindications include active local soft tissue infection, critically compromised soft tissue envelopes that preclude safe surgical incisions, and medically unstable patients who cannot tolerate regional or general anesthesia. Relative contraindications require nuanced clinical judgment and shared decision-making. These include severe baseline dementia in non-ambulatory patients who experience minimal pain, advanced physiological age with minimal functional demands, and severe osteopenia where hardware purchase is deemed impossible without catastrophic failure.
| Category | Absolute Indications / Contraindications | Relative Indications / Contraindications |
|---|---|---|
| Indications for Surgery | - Open fractures - Associated neurovascular compromise (e.g., acute carpal tunnel syndrome unresponsive to reduction) - Galeazzi fracture-dislocations in adults - Irreducible articular step-off > 2mm |
- Loss of volar tilt > 10 degrees dorsal - Radial shortening > 3mm - High-demand patient with borderline radiographic parameters - Concomitant ipsilateral upper extremity injuries (floating elbow) |
| Contraindications to Surgery | - Active local infection or osteomyelitis - Medically unstable patient (ASA IV/V) - Inadequate soft tissue coverage precluding incision |
- Non-ambulatory patient with severe dementia - Extreme osteoporosis precluding screw purchase - Delayed presentation (> 4 weeks) with asymptomatic malunion in low-demand elderly |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the foundation of successful execution in the operating theater. Standard orthogonal radiographs (posteroanterior, lateral, and oblique views) are mandatory. A traction view is often invaluable for delineating fracture fragments and assessing the degree of ligamentotaxis achievable. For any fracture exhibiting intra-articular extension, comminution, or suspected die-punch fragments (particularly of the lunate facet), a non-contrast Computed Tomography (CT) scan with 2D sagittal and coronal reformats, as well as 3D reconstructions, is considered the gold standard. The CT scan allows the surgeon to map the fracture lines precisely, identify central articular depression that may require bone grafting, and select the appropriate fragment-specific fixation strategy.
Templating software should be utilized to estimate the size and contour of the required volar locking plate. The surgeon must anticipate the need for adjunctive fixation, such as radial styloid pins, dorsal spanning plates for highly comminuted osteoporotic fractures, or bone graft substitutes to fill metaphyseal voids. For Galeazzi fractures, the length of the radial shaft plate must be templated to ensure a minimum of six cortices of fixation proximal and distal to the fracture site, utilizing a 3.5-mm dynamic compression plate (DCP) or locking compression plate (LCP).

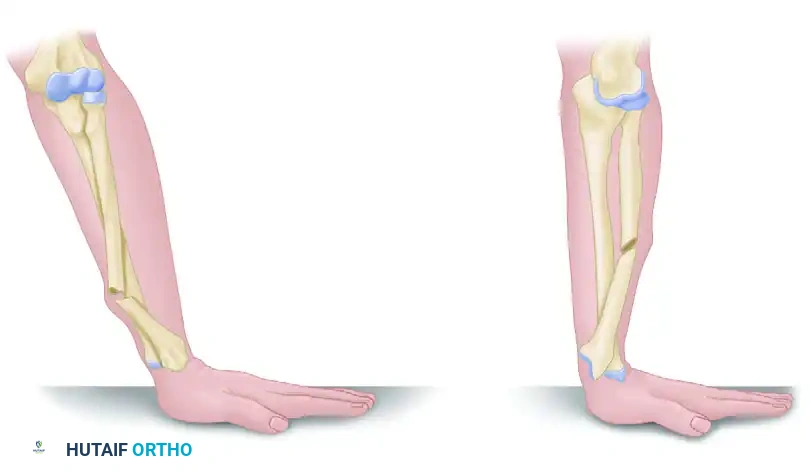
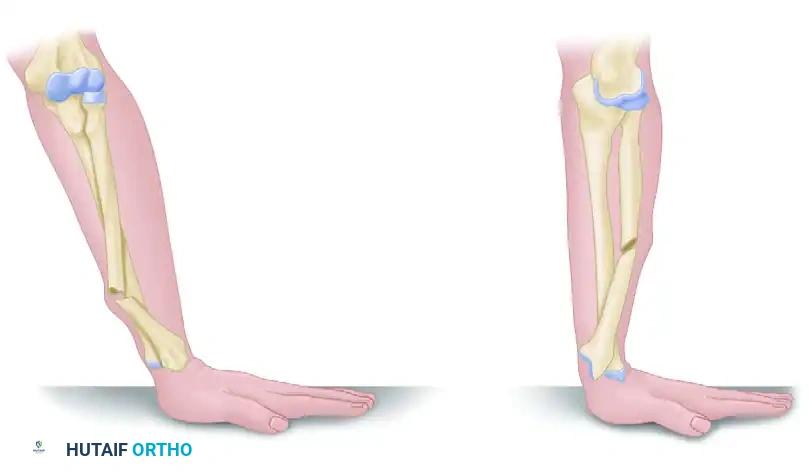
Preoperative radiograph demonstrating a classic Galeazzi fracture-dislocation with significant displacement of the distal radial shaft and gross disruption of the DRUJ.
Patient positioning and operating room setup must be standardized to optimize surgical flow and fluoroscopic imaging. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia, specifically a supraclavicular or axillary brachial plexus block, is highly preferred as it provides excellent intraoperative muscle relaxation, profound intraoperative analgesia, and minimizes the need for volatile anesthetics. General anesthesia is reserved for patients with contraindications to regional blocks or those with polytrauma.
The fluoroscopy unit (C-arm) should be brought in from the foot of the hand table, parallel to the longitudinal axis of the table, allowing for seamless transition between AP and lateral views without moving the fracture. The surgeon must ensure that a true lateral view of the radiocarpal joint can be obtained. This requires elevating the hand and tilting the C-arm approximately 15 to 22 degrees proximally to account for the normal radial inclination, allowing the beam to pass tangentially across the articular surface to confirm that no subchondral screws have penetrated the joint space.
Step-by-Step Surgical Approach and Fixation Technique
The workhorse approach for the vast majority of distal radius fractures and Galeazzi fractures is the volar approach, most commonly utilizing the flexor carpi radialis (FCR) bed (the modified Henry approach). An 8 to 10 cm longitudinal incision is made directly over the FCR tendon, extending proximally from the wrist crease. The superficial fascia is incised, and the FCR tendon sheath is opened. The FCR tendon is retracted ulnarly, protecting the median nerve which lies deep and ulnar to it. Alternatively, some surgeons prefer to retract the FCR radially to protect the radial artery, though this requires meticulous care of the palmar cutaneous branch of the median nerve. The deep internervous plane lies between the FCR (median nerve) and the brachioradialis (radial nerve).
Deep dissection reveals the flexor pollicis longus (FPL) tendon, which is gently retracted ulnarly to expose the pronator quadratus (PQ) muscle. An L-shaped incision is made along the radial and distal borders of the PQ, leaving a small cuff of tissue for later repair. The PQ is elevated subperiosteally from radial to ulnar, exposing the volar cortex of the distal radius. The fracture hematoma is evacuated, and the fracture site is debrided. Reduction is achieved using a combination of longitudinal traction, volar translation, and ulnar deviation. A Kapandji intrafocal pin or a periarticular reduction forceps can be utilized to lever the distal fragment out of its dorsally angulated position and restore volar tilt.
Once provisional reduction is achieved and confirmed fluoroscopically, a volar locking plate is applied. The plate must be positioned proximal to the watershed line to prevent FPL attrition. A proximal cortical screw in an oblong hole is placed first to allow for proximal-distal sliding and fine-tuning of the plate position. Distal locking screws are then placed into the subchondral bone to support the articular surface. The subchondral screws act as a fixed-angle construct, essentially functioning as an internal fixator that prevents secondary collapse, even in osteoporotic bone. A dorsal tangential fluoroscopic view is absolutely critical at this stage to ensure no screws have penetrated the dorsal cortex or the radiocarpal joint.
For Galeazzi fractures, the primary surgical objective is the rigid, anatomical restoration of the radial shaft. This is achieved via open reduction and internal fixation utilizing the same volar approach extended proximally. The radius is exposed, and the fracture is reduced anatomically. Fixation is achieved using a 3.5-mm dynamic compression plate (DCP) or locking compression plate (LCP) applied to the volar surface.


Postoperative anteroposterior (AP) and lateral radiographs following rigid fixation with a 3.5-mm AO dynamic compression plate and screws. In this specific case, anatomical restoration of the radius spontaneously reduced the DRUJ, rendering temporary stabilization with a transverse Kirschner wire unnecessary.
Once the radius is rigidly fixed, the surgeon's attention must immediately turn to the DRUJ. The stability of the DRUJ dictates the remainder of the surgical procedure. The DRUJ must be dynamically tested intraoperatively through a full range of pronation and supination using the ballottement test. If the DRUJ is reduced and stable, no further intervention is needed. If it is reducible but unstable, and a large ulnar styloid fragment is present, ORIF of the styloid is performed. If the instability is purely ligamentous, the TFCC must be repaired openly, or the ulna must be pinned to the radius with a transverse K-wire in supination. If the DRUJ is irreducible, soft tissue interposition (often the ECU tendon or median nerve) must be suspected, mandating a dorsal open exploration and reduction.
Complications, Incidence Rates, and Salvage Management
Despite advancements in implant design and surgical technique, the operative management of distal radius and Galeazzi fractures carries a distinct complication profile. The overall complication rate for volar plating of distal radius fractures ranges from 5% to 15%, depending on the complexity of the fracture and the patient's baseline comorbidities. Complications can be broadly categorized into hardware-related issues, soft tissue complications, nerve injuries, and late arthritic changes. Recognizing these complications early and understanding the appropriate salvage pathways is critical for the orthopedic surgeon.
Tendon complications are among the most frequently reported. Flexor pollicis longus (FPL) tendon rupture is a devastating complication unique to volar plating, occurring in approximately 1% to 2% of cases. It is almost exclusively caused by the placement of the plate at or distal to the watershed line, leading to mechanical attrition of the tendon against the prominent distal edge of the implant. Extensor tendon ruptures, particularly of the extensor pollicis longus (EPL), can occur if dorsal cortical screws protrude excessively through the dorsal cortex. Median nerve neuropathy, either transient neuropraxia from retraction or acute carpal tunnel syndrome from fracture hematoma, occurs in up to 5% of cases. Complex Regional Pain Syndrome (CRPS) is another debilitating complication, characterized by disproportionate pain, autonomic dysfunction, and severe stiffness.
Intra-articular screw penetration is a technical error that leads to rapid destruction of the radiocarpal or radioulnar joint cartilage. This highlights the absolute necessity of utilizing the dorsal horizon (tangential) fluoroscopic view during the index procedure. In the context of Galeazzi fractures, the most significant complication is chronic instability or arthrosis of the DRUJ, often resulting from failure to recognize and appropriately manage TFCC disruption during the initial surgery. Chronic DRUJ instability presents with profound weakness in grip strength and pain during forearm rotation.
Salvage management depends entirely on the nature of the complication. FPL or EPL ruptures require prompt tendon transfer (e.g., extensor indicis proprius to EPL transfer) or tendon grafting. Intra-articular hardware must be removed immediately upon recognition. For end-stage post-traumatic radiocarpal arthrosis, total wrist arthrodesis or total wrist arthroplasty (in low-demand patients) are the definitive salvage options. For chronic, painful DRUJ arthrosis or irreparable instability following a Galeazzi fracture, salvage procedures such as the Darrach procedure (resection of the distal ulna) or the Sauvé-Kapandji procedure (DRUJ arthrodesis with creation of a proximal ulnar pseudarthrosis) are highly effective at restoring painless forearm rotation, though they alter the load-bearing mechanics of the wrist permanently.
| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| FPL Tendon Rupture | 1% - 2% | Prevention: Keep plate proximal to watershed line. Salvage: Hardware removal, FDS or palmaris longus tendon transfer. |
| EPL Tendon Rupture | 1% - 3% | Prevention: Ensure screws do not penetrate dorsal cortex; use smooth pegs. Salvage: Extensor Indicis Proprius (EIP) to EPL tendon transfer. |
| Median Nerve Neuropathy | 2% - 5% | Prevention: Avoid aggressive retraction; consider prophylactic carpal tunnel release in high-energy injuries. Salvage: Endoscopic or open carpal tunnel release. |
| Intra-articular Screw Penetration | 2% - 4% | Prevention: Mandatory dorsal tangential fluoroscopic view. Salvage: Immediate hardware removal/exchange; late arthrodesis if cartilage destroyed. |
| Chronic DRUJ Instability (Galeazzi) | 5% - 10% | Prevention: Strict adherence to intra-operative DRUJ assessment algorithm. Salvage: Late TFCC reconstruction; Darrach or Sauvé-Kapandji procedure. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional outcome following surgical fixation of distal radius and Galeazzi fractures is heavily dependent on the execution of a structured, phased post-operative rehabilitation protocol. The advent of rigid volar locking plates has revolutionized post-operative care by allowing for early active mobilization, thereby mitigating the severe stiffness and capsular contractures that historically plagued cast-treated patients. However, the rehabilitation protocol must be carefully tailored to the specific injury pattern, the stability of the fixation achieved, and the status of the DRUJ.
The immediate post-operative phase (0 to 2 weeks) focuses on edema control, pain management, and the preservation of uninvolved joint mobility. The patient is typically placed in a bulky, non-circumferential volar resting splint to accommodate immediate post-operative swelling. Strict elevation of the extremity above heart level is mandated. Most crucially, patients are instructed to begin immediate active range of motion (ROM) of the digits, encompassing full composite flexion and extension. This not only prevents tendon adhesions but also acts as a muscle pump to reduce distal edema. Active motion of the elbow and shoulder is also encouraged to prevent proximal stiffness.
The intermediate phase (2 to 6 weeks) marks the transition to wrist-specific rehabilitation. At the two-week mark, sutures are removed, and the surgical splint is transitioned to a removable thermoplastic wrist orthosis. Under the guidance of a certified hand therapist, the patient begins active and active-assisted ROM of the radiocarpal joint, focusing on flexion, extension, radial deviation, and ulnar deviation. Passive stretching is generally avoided during this phase to prevent disruption of the healing osseous and soft tissue structures. If the DRUJ is stable, gentle pronation and supination exercises are initiated.
The late phase (6 to 12 weeks) is initiated once radiographic evidence of clinical union is observed. The orthosis is progressively weaned and discontinued. Therapy shifts toward aggressive passive stretching to maximize terminal range of motion, followed by progressive strengthening exercises. Grip strength, pinch strength, and endurance training are incorporated. Work conditioning and sport-specific activities are gradually introduced, with the expectation that maximum functional recovery may take up to a full year post-injury.
For Galeazzi fractures, the rehabilitation protocol is fundamentally altered by the management of the DRUJ. If the DRUJ was stable after radial plating, the standard early mobilization protocol is followed. However, if the DRUJ required K-wire pinning or open TFCC repair, the forearm must be strictly immobilized to protect the ligamentous healing. These patients are placed in an above-elbow (Muenster or sugar-tong) cast with the forearm in supination for 4 to 6 weeks. Only after the K-wires are removed or the TFCC is deemed adequately healed can forearm rotation exercises commence. This deliberate delay in rotation often requires a prolonged and intensive therapy course to overcome secondary DRUJ stiffness.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of distal radius and Galeazzi fractures is heavily guided by landmark clinical trials and consensus guidelines formulated by major orthopedic societies. The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines (CPG) on the Management of Distal Radius Fractures provides a robust, evidence-based framework for clinical decision-making. A strong recommendation within the CPG supports the use of rigid internal fixation for fractures with post-reduction radial shortening greater than 3 mm, dorsal tilt greater than 10 degrees, or intra-articular step-off greater than 2 mm, emphasizing that anatomical restoration correlates with superior functional outcomes in active individuals.
One of the most pivotal contributions to the literature regarding the bimodal demographic of these injuries is the WRIST (Wrist and Radius Injury Surgical Trial) study. This multicenter randomized controlled trial compared volar locking plate fixation, closed reduction with percutaneous pinning, external fixation, and cast immobilization in patients over the age of 60. The trial demonstrated that while volar plating yielded superior early radiographic alignment and earlier return of function at 3 to 6 months, there was no clinically significant difference in patient-reported outcome measures (PROMs) or pain scores at 12 and 24 months across the treatment modalities. This landmark finding has significantly influenced the modern approach to elderly, low-demand patients, suggesting that the risks of surgery may outweigh the benefits if acceptable, albeit imperfect, alignment can be maintained nonoperatively.
Regarding Galeazzi fractures, the historical literature remains foundational. The seminal work by Hughston in 1957 firmly established the Galeazzi injury as a "fracture of necessity," documenting a nearly 100% failure rate with closed management in adults. Modern biomechanical studies, such as those by Adams and colleagues, have further elucidated the kinematics of the DRUJ, confirming that anatomical plating of the radius restores approximately 80% of DRUJ stability, while the remaining 20% relies on the integrity of the TFCC. This biomechanical data directly underpins the modern surgical algorithm requiring intraoperative dynamic testing of the DRUJ after radial fixation.
Future directions in the management of these complex injuries are focusing on personalized surgical solutions. The integration of 3D printing technology for the creation of patient-specific, anatomically contoured plates is showing promise in the management of severe intra-articular malunions and highly comminuted osteoporotic fractures. Furthermore, the use of orthobiologics, including bone morphogenetic proteins (BMPs) and advanced osteoconductive scaffolds, is being actively investigated to augment fracture healing and address metaphyseal bone voids, aiming to reduce the reliance on autologous bone grafting and its associated donor site morbidity. As the literature continues to evolve, the fundamental principles of meticulous anatomical restoration, stable fixation, and structured rehabilitation remain the bedrock of operative success.

Chapter Index
- Comprehensive Introduction and Patho-Epidemiology
- Detailed Surgical Anatomy and Biomechanics
- Exhaustive Indications and Contraindications
- Pre-Operative Planning, Templating, and Patient Positioning
- Step-by-Step Surgical Approach and Fixation Technique
- Complications, Incidence Rates, and Salvage Management
- Phased Post-Operative Rehabilitation Protocols
- Summary of Landmark Literature and Clinical Guidelines
Back to Master Guide