
Introduction and Epidemiology
Calcaneus fractures represent a significant orthopedic challenge, demanding precise anatomic understanding and meticulous surgical execution. These injuries account for approximately 1% to 2% of all fractures in the human body, yet they carry a disproportionately high burden of morbidity and socioeconomic impact due to their propensity to affect young, working-age individuals. As the most frequently fractured tarsal bone, the calcaneus, or os calcis, represents 60% of all tarsal fractures in the adult population.
The annual incidence of calcaneal fractures is estimated at 11.5 per 100,000 people. Demographic analyses reveal a strong male predilection, with a male-to-female ratio of 2.4 to 1. The peak incidence occurs in males aged 20 to 29 years, correlating with high-energy occupational and recreational activities. Displaced intra-articular fractures comprise the vast majority of these injuries, representing 60% to 75% of all calcaneus fractures. Given the high-energy mechanisms typically involved, approximately 10% of calcaneus fractures present as open injuries, which require emergent surgical intervention and aggressive soft tissue management.
The predominant mechanism of injury for calcaneal fractures is axial loading. Approximately 70% of calcaneal fractures result from falls from a height. During such events, the talus is driven downward into the calcaneus like a wedge. The calcaneus is structurally composed of a thin cortical shell surrounding a dense network of cancellous bone, making it particularly susceptible to this crushing force. In motor vehicle collisions, calcaneus fractures frequently occur when the accelerator or brake pedal impacts the plantar aspect of the foot during sudden deceleration.
While axial loading is responsible for most intra-articular fractures, twisting forces are more commonly associated with extra-articular calcaneus fractures. These include fractures of the anterior process, the medial process, or the sustentaculum tali. Furthermore, specific patient populations exhibit unique fracture patterns; for instance, diabetic patients demonstrate an increased incidence of tuberosity fractures resulting from avulsion by the Achilles tendon, often occurring with relatively low-energy trauma.
Associated Injuries
The high-energy nature of the typical calcaneus fracture necessitates a comprehensive secondary survey. Up to 50% of patients with calcaneus fractures present with concomitant injuries. Lumbar spine fractures, particularly burst or compression fractures resulting from the same axial load vector, occur in approximately 10% of patients. Other fractures of the lower extremities, including tibial plateau and pilon fractures, are seen in up to 25% of cases. Bilateral calcaneus fractures are present in 5% to 10% of patients, intuitively correlating with higher-energy trauma such as bilateral foot impact following a significant fall.
Surgical Anatomy and Biomechanics
A profound understanding of calcaneal anatomy is the foundation of successful surgical reconstruction. The calcaneus serves as the primary weight-bearing structure of the hindfoot and acts as a lever arm for the Achilles tendon.
Articular Facets and Subtalar Joint
The superior articular surface of the calcaneus contains three distinct facets that articulate with the talus to form the subtalar joint.
1. The posterior facet is the largest of the three and constitutes the major weight-bearing surface. It is convex anteriorly to posteriorly and is highly susceptible to depression during axial loading.
2. The middle facet is located anteromedially and is supported by the sustentaculum tali, a dense cortical medial projection.
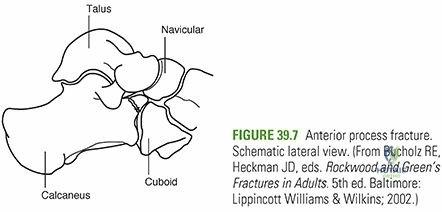
3. The anterior facet is located on the anterior process and is often confluent with the middle facet.
Between the middle and posterior facets lies the interosseous sulcus, also known as the calcaneal groove. When articulated with the corresponding talar sulcus, this structure forms the sinus tarsi, a critical anatomical landmark that houses the interosseous talocalcaneal ligament, the cervical ligament, and the primary blood supply to the talus.

The Sustentaculum Tali and Medial Structures
The sustentaculum tali is arguably the most critical anatomical feature in calcaneus fracture fixation. It supports the neck of the talus medially and contains the middle articular facet on its superior aspect. Biomechanically, it remains securely attached to the talus via the robust interosseous talocalcaneal and deltoid ligaments. Because these ligaments rarely fail, the sustentaculum tali typically remains in its anatomic position relative to the talus, earning it the designation of the "constant fragment." Surgical reduction of the posterior facet and the calcaneal tuberosity is fundamentally based on reducing these displaced fragments back to this constant sustentacular fragment.
Medially, the flexor hallucis longus (FHL) tendon passes directly beneath the sustentaculum tali. This proximity places the FHL tendon at significant risk for iatrogenic injury if screws directed from lateral to medial are excessively long.
Lateral and Posterior Structures
Laterally, the peroneal tendons (peroneus longus and brevis) pass between the lateral wall of the calcaneus and the lateral malleolus. In displaced intra-articular fractures, the lateral wall of the calcaneus often "blows out," leading to subfibular impingement, peroneal tendon dislocation, or tenosynovitis. Restoring the morphology of the lateral wall is essential to decompress this space.
Posteriorly, the Achilles tendon inserts into the middle third of the posterior tuberosity. The superior third is separated from the Achilles tendon by the retrocalcaneal bursa, while the inferior third is continuous with the plantar fascia. The triceps surae complex exerts a massive superior and anterior pull on the tuberosity fragment, contributing to the classic varus, shortened, and dorsiflexed deformity seen in displaced fractures.
Clinical and Radiographic Evaluation
Clinical Presentation and Soft Tissue Assessment
Patients with calcaneus fractures typically present with moderate to severe heel pain, accompanied by profound tenderness, swelling, heel widening, and limb shortening. The classic physical examination finding is Mondor's sign, characterized by ecchymosis extending to the plantar arch, which is highly suggestive of a calcaneus fracture.
Soft tissue evaluation dictates the timing and feasibility of surgical intervention. Massive swelling often leads to fracture blisters, which typically develop within the first 36 hours post-injury. Clear fluid blisters represent an intra-epidermal cleavage plane, whereas blood-filled blisters indicate a deeper, subepidermal cleavage plane with more severe soft tissue compromise. Open fractures, though rare, predominantly occur on the medial aspect of the hindfoot due to the varus blowout of the tuberosity fragment piercing the medial skin.
Careful evaluation of neurovascular status is mandatory. Compartment syndrome of the foot must be rigorously ruled out, as it occurs in up to 10% of calcaneus fractures. The central compartment is most frequently involved. Missed compartment syndrome may result in devastating sequelae, including clawing of the lesser toes, chronic pain, and severe functional impairment.

Radiographic Imaging
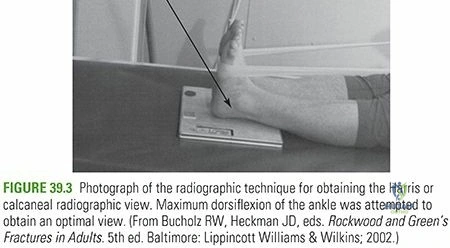
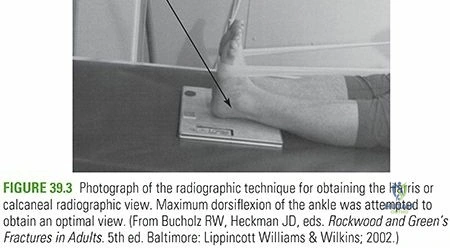
Initial radiographic evaluation must include a lateral view of the hindfoot, an anteroposterior (AP) view of the foot, a Harris axial view, and a complete ankle series to rule out associated injuries.
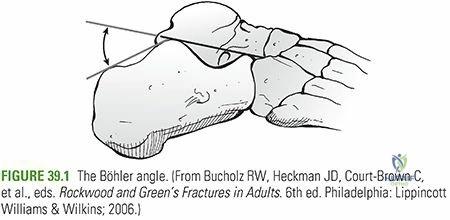
The lateral radiograph is critical for assessing two key morphologic parameters:
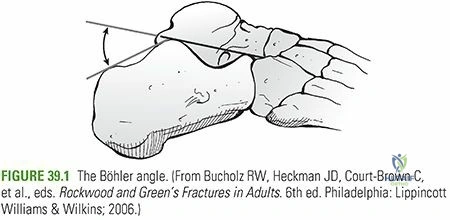
1. Böhler Angle: This angle is composed of a line drawn from the highest point of the anterior process of the calcaneus to the highest point of the posterior facet, intersecting with a line drawn tangential from the posterior facet to the superior edge of the tuberosity. The angle is normally between 20 and 40 degrees. A decrease in this angle indicates that the weight-bearing posterior facet of the calcaneus has collapsed, thereby shifting body weight anteriorly and disrupting hindfoot biomechanics.
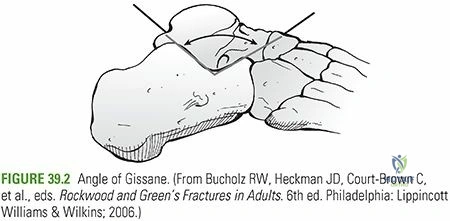
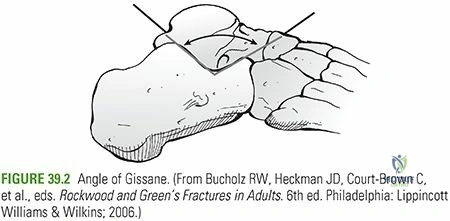
2. Angle of Gissane: Formed by the downward slope of the posterior facet and the upward slope of the anterior process, this angle normally measures 120 to 145 degrees. An increase in the Angle of Gissane typically indicates a depressed posterior facet.
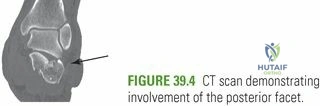
Computed Tomography and Classification
Computed Tomography (CT) is the gold standard for preoperative planning. Axial, sagittal, and coronal reformats are essential.
* Coronal views are utilized to assess the posterior facet and the sustentaculum tali.
* Axial views evaluate the calcaneocuboid joint, the anterior process, and the lateral wall blowout.
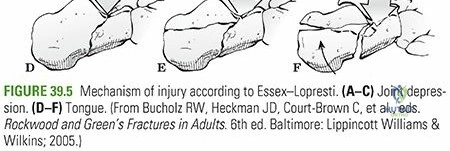
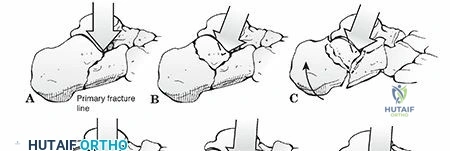
* Sagittal views differentiate between Essex-Lopresti joint depression and tongue-type fracture patterns.
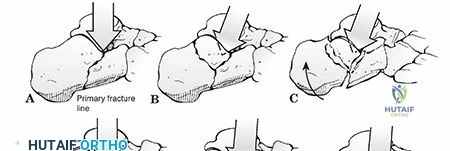
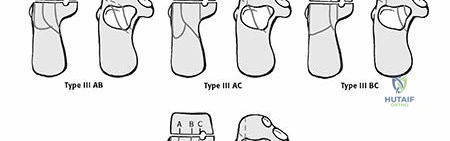
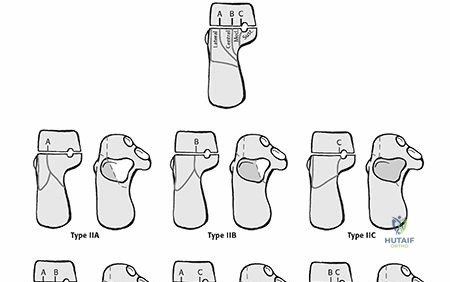
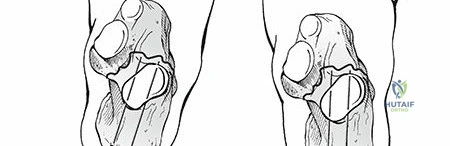
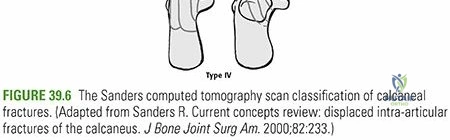
The Sanders Classification is the most widely utilized system for intra-articular calcaneus fractures, based on coronal CT images at the widest portion of the posterior facet. The classification divides the posterior facet into three potential fracture lines (A, B, and C), moving from lateral to medial.
* Type I: Non-displaced fractures, regardless of the number of fracture lines.
* Type II: Two-part fractures of the posterior facet (IIA, IIB, IIC based on the primary fracture line).
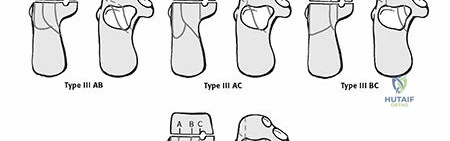
* Type III: Three-part fractures with a central depressed fragment (IIIAB, IIIAC, IIIBC).
* Type IV: Four-part, highly comminuted intra-articular fractures.
Indications and Contraindications
The decision to operate on a calcaneus fracture requires a delicate balance between the benefits of anatomic restoration and the significant risks of soft tissue complications. Patient selection is paramount.
| Indication Category | Specific Conditions |
|---|---|
| Operative Indications | Displaced intra-articular fractures (Sanders Type II and III) involving the posterior facet with >2mm step-off. |
| Tongue-type fractures with posterior skin compromise (impending open fracture). | |
| Displaced extra-articular fractures resulting in varus/valgus malalignment or significant loss of calcaneal height/length. | |
| Lateral wall blowout causing severe subfibular impingement or peroneal tendon dislocation. | |
| Open fractures requiring irrigation and debridement. | |
| Non-Operative Indications | Non-displaced or minimally displaced intra-articular fractures (Sanders Type I). |
| Extra-articular fractures with minimal displacement and intact Achilles function. | |
| Patients with severe peripheral vascular disease or critical limb ischemia. | |
| Uncontrolled diabetes mellitus with neuropathy (Charcot risk). | |
| Heavy smokers who refuse cessation (relative to absolute contraindication depending on surgeon preference). | |
| Non-ambulatory patients or those with severe medical comorbidities precluding surgery. | |
| Severe, non-resolving soft tissue compromise where surgical intervention would guarantee wound necrosis. |
Pre Operative Planning and Patient Positioning
Timing of Surgery
Timing is arguably the most critical factor in mitigating wound complications. Surgery must be delayed until the soft tissue envelope has adequately recovered from the initial trauma. This is clinically assessed using the "wrinkle test." When the skin over the lateral hindfoot wrinkles upon dorsiflexion and eversion of the ankle, the edema has subsided sufficiently to proceed. This typically occurs between 10 and 21 days post-injury. Operating through swollen, non-compliant tissue drastically increases the risk of wound dehiscence and deep infection.
In cases of tongue-type fractures where the displaced tuberosity threatens the posterior skin, emergent closed reduction and percutaneous pinning are required to prevent full-thickness skin necrosis.
Patient Positioning and Fluoroscopy Setup
Patient positioning depends on the chosen surgical approach. For the classic extensile lateral approach, the patient is placed in the lateral decubitus position on a radiolucent beanbag. All bony prominences must be meticulously padded. The operative leg is positioned with the knee slightly flexed.
A radiolucent triangle or bump is placed under the operative leg to facilitate unobstructed lateral and axial fluoroscopic views. The C-arm is typically brought in from the anterior or plantar aspect of the foot to allow for dynamic intraoperative imaging without compromising the sterile field.
For minimally invasive sinus tarsi approaches or percutaneous fixation of tongue-type fractures, the patient may be positioned prone or semi-prone. A thigh tourniquet is routinely utilized to ensure a bloodless surgical field, though its use should be minimized in patients with borderline vascular status.
Detailed Surgical Approach and Technique
The Extensile Lateral Approach
The extensile lateral approach remains the workhorse for complex, highly comminuted calcaneus fractures (Sanders III and IV). It provides unparalleled exposure of the lateral wall, posterior facet, and calcaneocuboid joint.
- Incision and Flap Creation: A right-angled "L" incision is utilized. The vertical limb is placed slightly anterior to the Achilles tendon, and the horizontal limb is placed in the transition zone between the glabrous plantar skin and the lateral heel skin, avoiding the sural nerve.
- Full-Thickness Dissection: It is imperative to raise a full-thickness fasciocutaneous flap directly off the periosteum. Skiving into the subcutaneous tissues will disrupt the delicate vascular supply (primarily from the lateral calcaneal artery) and lead to flap necrosis.
- No-Touch Retraction: Once the flap is elevated, it is retracted using 1.6mm or 2.0mm K-wires driven into the talus and lateral malleolus. Retractors should never be used on the skin edges, as this precipitates ischemia and wound breakdown. The peroneal tendons are mobilized and retracted superiorly within the flap.
The Sinus Tarsi Approach
For less comminuted fractures (Sanders II), the minimally invasive sinus tarsi approach has gained significant traction due to drastically lower wound complication rates.
1. Incision: A 3 to 5 cm linear incision is made from the tip of the lateral malleolus extending towards the base of the fourth metatarsal.
2. Deep Dissection: The extensor digitorum brevis is elevated or split to expose the subtalar joint and the posterior facet. This approach provides excellent visualization of the articular surface but limits access to the posterior tuberosity, necessitating percutaneous manipulation of the heel.
Fracture Reduction Sequence
Regardless of the approach, the reduction follows a systematic sequence:
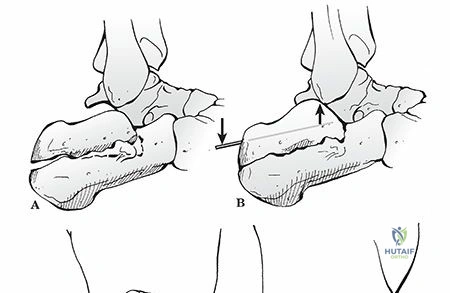
1. Tuberosity Reduction: A 5.0mm Schanz pin is inserted transversely into the posterior tuberosity from lateral to medial. This pin is used as a joystick to pull the tuberosity out of varus, restore calcaneal length, and correct the loss of height.
2. Posterior Facet Reduction: The depressed articular fragments are elevated. In an extensile approach, the lateral wall is hinged open like a book to access the joint. The posterior facet is reduced anatomically to the constant sustentacular fragment. Provisional fixation is achieved with K-wires directed from lateral to medial into the sustentaculum.
3. Anterior Process and Calcaneocuboid Joint: If involved, the anterior process is reduced to restore the lateral column length.
4. Lateral Wall Decompression: The lateral wall blowout is reduced to eliminate subfibular impingement.
Internal Fixation Strategy
Once anatomic reduction is confirmed fluoroscopically (utilizing Brodén views to assess the posterior facet), definitive fixation is applied.
* Subchondral Raft Screws: 3.5mm or 4.0mm lag screws are placed directly beneath the posterior facet, engaging the dense bone of the sustentaculum tali. Care must be taken to avoid penetrating the medial cortex, which risks tethering the FHL tendon.
* Plate Application: A low-profile calcaneal locking plate is applied to the lateral wall. The plate acts as a neutralization device for the articular screws and a buttress for the lateral wall.
* Void Management: Elevation of the depressed posterior facet often leaves a significant cancellous void. The use of bone graft or orthobiologic bone substitutes remains controversial but is frequently utilized to provide structural support and prevent late subsidence.
Complications and Management
The surgical management of calcaneus fractures is fraught with potential complications, primarily driven by the tenuous soft tissue envelope and the complex articular anatomy.
| Complication | Estimated Incidence | Etiology and Clinical Presentation | Salvage and Management Strategies |
|---|---|---|---|
| Wound Dehiscence / Infection | 10% - 25% (Extensile Approach) | Ischemia of the apex of the L-flap; smoking; premature surgery. Presents as marginal necrosis or deep hardware infection. | Local wound care, negative pressure wound therapy. Deep infections require hardware removal, aggressive debridement, and potential free tissue transfer. |
| Post-Traumatic Subtalar Arthritis | 30% - 50% | Chondral injury at the time of impact or residual articular step-off. Presents as chronic hindfoot pain exacerbated by uneven ground. | Conservative management with rigid AFOs or custom orthotics. Surgical salvage requires subtalar arthrodesis (fusion). |
| Sural Nerve Injury |
Clinical & Radiographic Imaging
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding calcaneus-fractures