Percutaneous Reduction and Fixation of Calcaneal Fractures: A Comprehensive Surgical Guide
Key Takeaway
Percutaneous reduction and fixation of calcaneal fractures offers a minimally invasive alternative to extensile lateral approaches, significantly reducing wound complications. This technique utilizes targeted stab incisions, fluoroscopic or arthroscopic guidance, and precise screw placement to restore the posterior facet and tuberosity alignment. Ideal for Sanders type II fractures, it provides comparable functional outcomes to open reduction while accelerating return to work and minimizing soft tissue morbidity in high-risk patients.
Comprehensive Introduction and Patho-Epidemiology
The management of displaced intra-articular calcaneal fractures remains one of the most rigorously debated and continuously evolving topics in orthopedic trauma. Representing approximately 60% of all tarsal bone fractures, these injuries typically result from high-energy axial loading mechanisms, such as falls from a significant height or motor vehicle collisions. Historically, the extensile lateral approach has been championed as the gold standard for open reduction and internal fixation (ORIF). This traditional method provides unparalleled, direct visualization of the posterior facet, the lateral calcaneal wall, and the calcaneocuboid joint, allowing for meticulous anatomical reconstruction of the articular surfaces and restoration of overall calcaneal morphology. However, the extensile lateral approach is notoriously fraught with significant soft tissue morbidity. Complications such as marginal wound necrosis, complete flap dehiscence, and devastating deep osseous infections are well-documented, primarily owing to the tenuous vascular supply of the lateral hindfoot angiosome.
To mitigate these profound soft tissue risks, percutaneous reduction and fixation techniques have emerged as a highly effective, minimally invasive alternative that fundamentally alters the risk-benefit calculus of calcaneal fracture management. By utilizing targeted stab incisions, indirect reduction maneuvers, and advanced fluoroscopic or arthroscopic assistance, orthopedic surgeons can achieve anatomical restoration of the posterior facet and calcaneal tuberosity while meticulously preserving the delicate soft tissue envelope. This paradigm shift is particularly advantageous—and often strictly indicated—in patients with significant medical comorbidities. Populations afflicted with diabetes mellitus, peripheral vascular disease, neuropathy, or a history of chronic tobacco use present an unacceptably high risk of wound breakdown with an extensile approach. In these cohorts, percutaneous techniques offer a limb-saving alternative that balances the biomechanical necessity of articular reduction with the biological imperative of soft tissue preservation.
The primary biomechanical goals of any calcaneal fracture fixation, regardless of the surgical approach, remain steadfast: the anatomical restoration of congruity in the subtalar joint (specifically the posterior facet), the recovery of calcaneal height (measured by Böhler’s angle) and width, and the absolute correction of varus malalignment of the tuberosity. Failure to accurately correct varus malrotation severely limits transverse tarsal joint mobility, effectively locking the midfoot and leading to a rigid, painful gait cycle. Furthermore, uncorrected lateral wall blowout and loss of height consistently lead to debilitating lateral subfibular impingement, where the peroneal tendons become entrapped between the lateral calcaneal wall and the tip of the lateral malleolus. Thus, the percutaneous surgeon must rely on profound anatomical knowledge and advanced intraoperative imaging to achieve these biomechanical goals without the luxury of direct, wide visualization.
Detailed Surgical Anatomy and Biomechanics
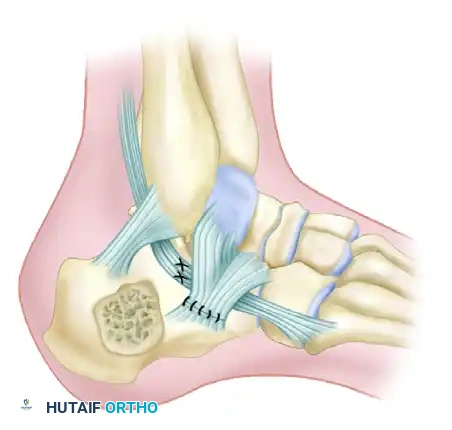
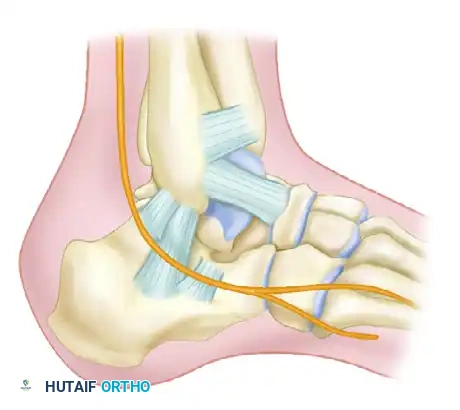
A profound understanding of hindfoot osteology, ligamentous restraints, and regional vascularity is the absolute cornerstone of successful percutaneous calcaneal fixation. The calcaneus is a complex, three-dimensional structure that articulates superiorly with the talus through three distinct facets (anterior, middle, and posterior) and anteriorly with the cuboid. The posterior facet is the largest and most critical weight-bearing articular surface, and its anatomical restoration is the primary objective in the management of intra-articular fractures. Medially, the sustentaculum tali projects outwards to support the middle facet. Crucially, the sustentaculum tali is tightly bound to the talus by the robust deltoid and interosseous talocalcaneal ligaments. Because these ligamentous attachments rarely rupture during axial loading, the sustentacular fragment typically remains anatomically aligned with the talus, earning its designation as the "constant" fragment. All reduction maneuvers in percutaneous fixation are fundamentally based on bringing the displaced, comminuted lateral and posterior tuberosity fragments back to this medial constant fragment.
The vascular anatomy of the lateral hindfoot dictates the boundaries of surgical intervention and explains the high complication rates associated with traditional open approaches. The lateral calcaneal skin flap is primarily supplied by the lateral calcaneal artery, a terminal branch of the peroneal artery, with variable contributions from the sural artery and the lateral tarsal artery. This vascular network forms a delicate angiosome that is highly susceptible to disruption from trauma, edema, and surgical incisions. The lack of a robust muscular layer between the skin and the lateral calcaneal wall means that any surgical incision relies entirely on the subdermal plexus for healing. Percutaneous techniques respect this vascular vulnerability by utilizing small stab incisions that avoid transecting the primary arterial branches, thereby preserving the microcirculation essential for uneventful wound healing.
Biomechanically, the calcaneus functions as a critical lever arm for the Achilles tendon and serves as the foundational block for the longitudinal arch of the foot. Normal calcaneal morphology is often assessed radiographically using Böhler’s angle (normally 20 to 40 degrees) and the Crucial Angle of Gissane (normally 100 to 130 degrees). In a typical axial load injury, the talus acts as a wedge, driving down into the calcaneus, flattening Böhler’s angle, widening the calcaneus laterally, and driving the tuberosity into varus. If this pathological anatomy is not corrected, the biomechanical consequences are severe. A flattened Böhler’s angle decreases the lever arm of the Achilles tendon, leading to profound plantarflexion weakness. A widened lateral wall causes subfibular impingement and subluxation or stenosis of the peroneal tendons. Finally, a varus tuberosity alters the axis of the subtalar joint, locking the talonavicular and calcaneocuboid joints, which abolishes the foot's ability to accommodate uneven terrain.
Exhaustive Indications and Contraindications
The decision to proceed with percutaneous reduction and fixation of a calcaneal fracture requires a nuanced evaluation of the fracture morphology, the condition of the soft tissue envelope, and the patient's physiological status. Percutaneous techniques are most effectively deployed in Sanders Type IIA and IIB fractures, where the posterior facet is split into two primary articular fragments that can be manipulated indirectly. It is also the treatment of choice when the soft tissue envelope is severely compromised by fracture blisters, massive edema, or abrasions that would absolute preclude a traditional extensile lateral incision. Furthermore, percutaneous fixation is highly indicated in polytrauma patients requiring rapid stabilization for mobilization, or in patients with profound medical comorbidities (e.g., poorly controlled diabetes, heavy smoking) where the risk of catastrophic wound infection following an open approach outweighs the benefits of direct articular visualization.
Conversely, there are strict contraindications to percutaneous management. Sanders Type IV fractures, characterized by severe, highly comminuted "blow-out" patterns of the posterior facet, generally cannot be anatomically reduced via closed or percutaneous means. Attempting percutaneous fixation in these scenarios often results in retained intra-articular step-offs and rapid progression to post-traumatic subtalar arthrosis; these patients are often better served by primary subtalar arthrodesis or an extensile open approach if reconstruction is attempted. Active localized infection or severe peripheral arterial disease rendering the foot ischemic are absolute contraindications to any internal fixation. Relative contraindications include fractures presenting more than three weeks post-injury, as early consolidation and fracture callus make indirect reduction maneuvers nearly impossible.
Indications and Contraindications Summary
| Category | Percutaneous Fixation Parameters | Clinical Rationale / Impact |
|---|---|---|
| Primary Indications | Sanders Type IIA and IIB fractures; large, simple posterior facet fragments. | Allows for indirect manipulation and reduction using bone tamps and joystick techniques without requiring direct visualization. |
| Soft Tissue Indications | Severe edema, hemorrhagic fracture blisters, tenuous skin wrinkling. | Avoids the catastrophic wound necrosis associated with extensile incisions through compromised, edematous tissue. |
| Patient Demographics | Diabetics, active smokers, peripheral vascular disease, elderly patients. | Minimizes the risk of deep infection and amputation in populations with known microvascular and macrovascular healing deficits. |
| Contraindications (Absolute) | Active local infection; critical limb ischemia; non-ambulatory baseline. | Hardware placement in an infected or ischemic field guarantees failure; non-ambulatory patients do not require articular reconstruction. |
| Contraindications (Relative) | Sanders Type IV (severe comminution); fractures >3 weeks old. | Extreme comminution cannot be accurately reduced percutaneously; older fractures have early callus preventing indirect manipulation. |
Pre-Operative Planning, Templating, and Patient Positioning
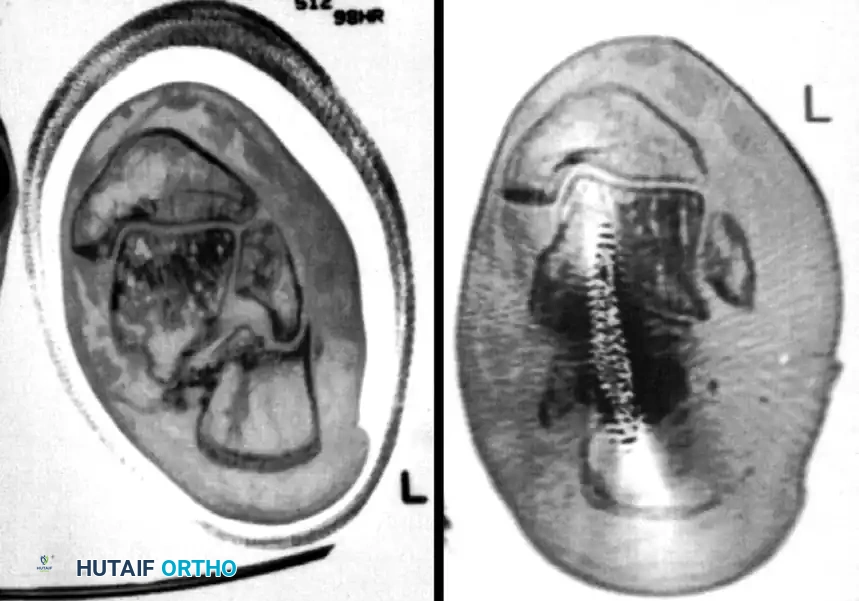
Meticulous preoperative planning is the absolute prerequisite for successful percutaneous fixation, as the surgeon must mentally reconstruct the three-dimensional fracture pattern before entering the operating room. Standard trauma radiographs, including lateral, axial (Harris), and anteroposterior views of the foot, must be obtained to assess overall calcaneal morphology, height, and varus/valgus alignment. However, a fine-cut computed tomography (CT) scan (1-2mm slices) with multiplanar sagittal and coronal reconstructions is mandatory. The CT scan delineates the exact fracture pattern, assesses the degree of posterior facet comminution, identifies the location of the primary fracture lines (e.g., central, medial, lateral), and is required to classify the injury according to the Sanders classification system. The surgeon must specifically evaluate the integrity of the sustentaculum tali and the anterior process, as these regions serve as the anchor points for definitive hardware placement.
Operating room setup and patient positioning must be optimized to facilitate unhindered fluoroscopic imaging, which serves as the surgeon's "eyes" during a percutaneous procedure. The patient is typically placed in the lateral decubitus position on a fully radiolucent operating table. A vacuum bean bag positioner is highly recommended to maintain strict stability, ensuring the patient does not roll during aggressive reduction maneuvers. The non-operative leg is flexed at the hip and knee and padded securely, while the operative leg is extended. A well-padded thigh tourniquet is applied to provide a bloodless surgical field if an open conversion becomes necessary, though inflation is rarely required for purely percutaneous techniques unless excessive bleeding obscures arthroscopic visualization.
The positioning of the C-arm fluoroscope is arguably the most critical logistical step in the procedure. The C-arm should be brought in from the anterior or plantar aspect of the patient, allowing the base of the machine to remain out of the surgeon's primary working space. The C-arm must be able to rapidly transition between lateral, axial (Harris), and Broden’s views without encountering physical obstruction from the table or the patient's contralateral limb. Broden’s views are specifically utilized to visualize the posterior facet; they are obtained by internally rotating the leg 40 degrees and angling the fluoroscope beam cephalad at 10, 20, 30, and 40 degrees. The surgeon must confirm that all necessary fluoroscopic angles can be achieved seamlessly before the patient is prepped and draped, as intraoperative delays for imaging adjustments can compromise the reduction.
Step-by-Step Surgical Approach and Fixation Technique
1. Traction, Disimpaction, and Tuberosity Control
The initial and arguably most physically demanding step in percutaneous fixation involves regaining control of the displaced calcaneal tuberosity. Due to the massive deforming force of the Achilles tendon, the tuberosity fragment is typically pulled proximally (resulting in loss of Böhler’s angle), translated laterally, and rotated into varus. To counter this, a large, fully threaded Steinmann pin (typically 4.0mm to 5.0mm) or a heavy Schanz screw is inserted transversely into the posteroinferior aspect of the tuberosity fragment, taking care to stay inferior to the fracture line.
Once the pin is securely engaged in the dense bone of the tuberosity, the surgeon applies sustained, forceful manual traction in a plantar, distal, and valgus direction. This maneuver utilizes the principle of ligamentotaxis to disimpact the fracture fragments, restore calcaneal length, and correct the critical varus deformity. The surgeon must physically unlock the tuberosity from the proximal fragments. If manual traction is insufficient due to early consolidation or a highly impacted fracture pattern, a temporary external fixator or a femoral distractor can be applied. Half-pins are placed in the calcaneal tuberosity and the distal tibial diaphysis, allowing for controlled, sustained mechanical distraction to maintain length and alignment while the articular surface is addressed.
2. Reduction of the Posterior Facet
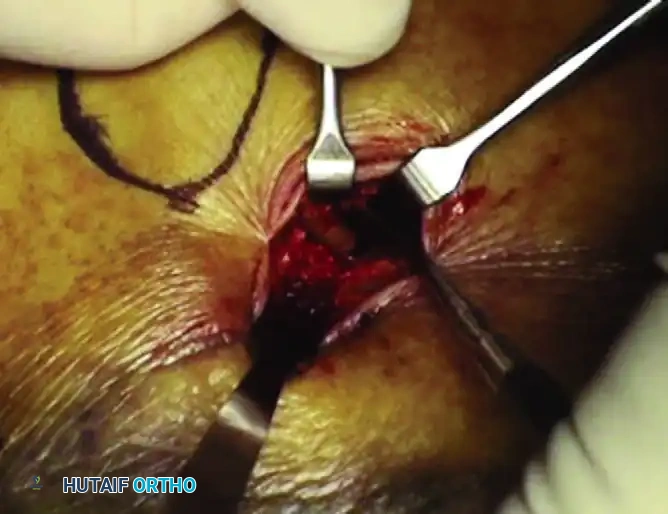
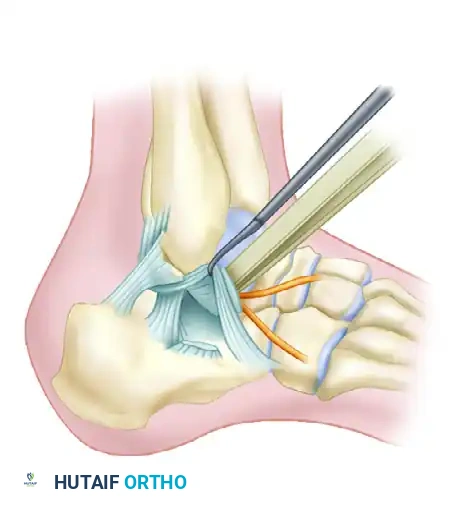
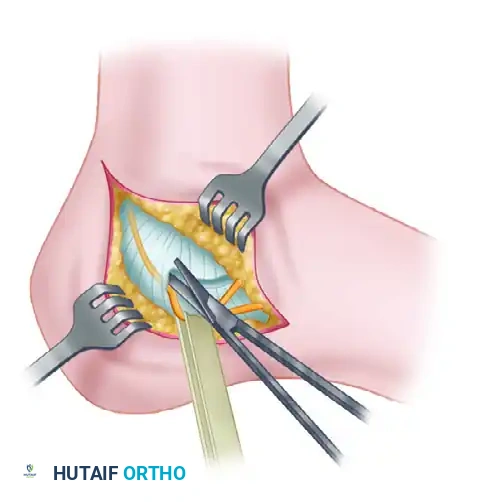
Once the tuberosity is disimpacted and gross calcaneal morphology is restored, attention is directed to the articular surface of the subtalar joint. A small (1-2 cm) stab incision is made directly over the sinus tarsi, guided by lateral fluoroscopy. Blunt dissection is carried down to the lateral wall of the calcaneus, taking immense care to protect the peroneal tendons and the sural nerve, which lie in close proximity. A small periosteal elevator or a specialized, curved bone tamp is introduced through this incision and positioned precisely beneath the depressed posterior facet fragment.
Under continuous fluoroscopic guidance—specifically utilizing dynamic Broden’s views—the surgeon gently elevates the articular fragment. The goal is to bring the depressed lateral articular surface flush with the medial "constant" sustentacular fragment.

Subtalar arthroscopy can be an invaluable, advanced adjunct during this step, particularly for Sanders Type IIA and IIB fractures. By inserting a 2.7mm or 4.0mm arthroscope into the posterior portal, the surgeon gains direct, magnified visualization of the articular cartilage. This ensures an absolute anatomical reduction (step-off < 1mm) that two-dimensional fluoroscopy alone may occasionally fail to confirm. Any soft tissue or small osteochondral debris interposed in the fracture site can be arthroscopically debrided to facilitate a perfect cortical read.
3. Provisional Stabilization and K-Wire Placement
Once anatomical reduction of the posterior facet is confirmed via fluoroscopy and/or arthroscopy, the fragments must be provisionally stabilized before the definitive cannulated screws are introduced. Loss of reduction during drilling is a common pitfall that must be actively prevented.
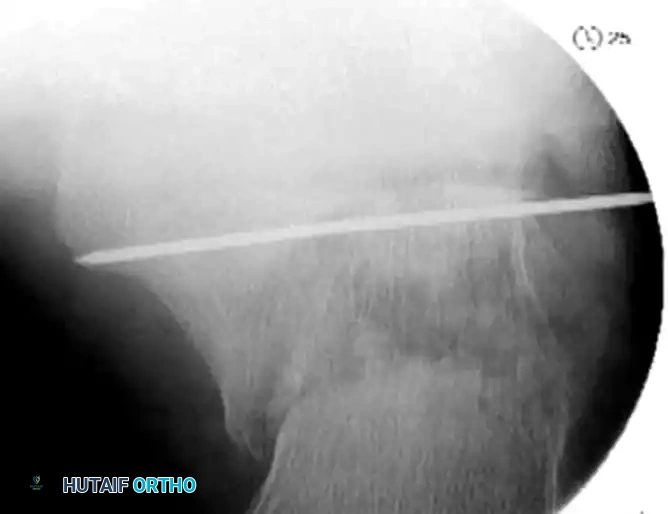
Multiple smooth Kirschner wires (K-wires), typically 1.6mm or 2.0mm, are inserted percutaneously from the lateral aspect of the calcaneus. These wires are directed medially and slightly superiorly, aiming for the dense, high-quality cortical bone of the sustentaculum tali. The trajectory of these wires is critical; they must capture the elevated lateral articular fragment and compress it against the stable medial fragment.

The surgeon must meticulously verify the position of every K-wire using axial and Broden’s fluoroscopic views. It is imperative to ensure that the wires do not inadvertently penetrate the subtalar joint space, which would cause iatrogenic cartilage damage, nor should they plunge too far medially, where they risk tethering the flexor hallucis longus (FHL) tendon or injuring the medial neurovascular bundle (posterior tibial artery and tibial nerve).
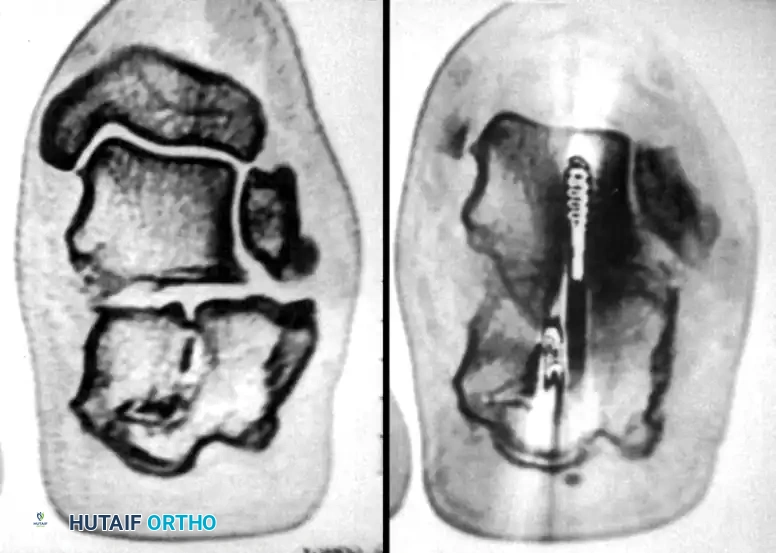
4. Definitive Cannulated Screw Fixation
Definitive stabilization is achieved using cannulated screws, which provide robust interfragmentary compression across the fracture lines and rigid maintenance of the restored three-dimensional anatomy. Over the provisional K-wires securing the posterior facet, 3.5-mm or 4.0-mm partially threaded cortical screws are placed. The appropriate length is measured, and the lateral cortex is carefully over-drilled to allow for a lag effect. These screws are driven from lateral to medial, compressing the lateral articular fragment firmly against the medial sustentacular fragment. Washers may be utilized if the lateral wall bone quality is osteoporotic.
Following articular fixation, the corrected position of the tuberosity must be locked in place. Fully threaded screws (typically 4.5mm or 6.5mm) are inserted from the posterior tuberosity, directed anteriorly toward the calcaneocuboid joint or the base of the anterior process. These screws are placed parallel to the initial Steinmann pin used for traction. Fully threaded screws are strictly preferred in this location to act as "position screws"; they hold the corrected length and Böhler's angle without compressing the fracture, which could inadvertently shorten the calcaneus and recreate the deformity.
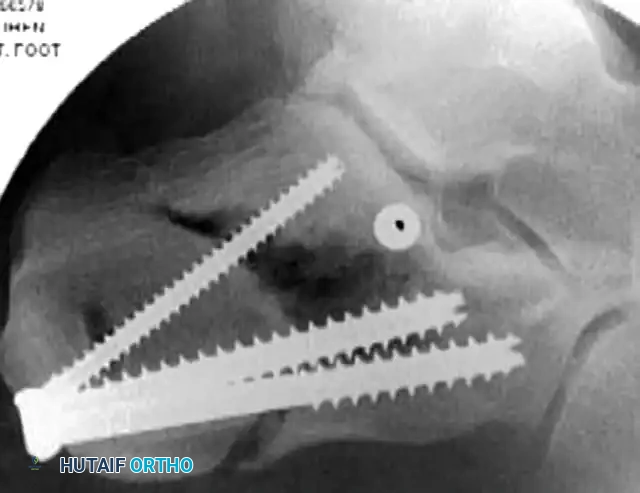
Once all definitive hardware is placed, the initial Steinmann pin and any remaining provisional K-wires are removed. A final, comprehensive fluoroscopic check is performed. The surgeon must confirm extra-articular hardware placement, complete restoration of Böhler’s angle, and absolute correction of varus alignment on the axial Harris view.


The small stab incisions are copiously irrigated and closed using simple interrupted non-absorbable sutures (e.g., 3-0 Nylon or Prolene) to minimize tissue strangulation.

5. Surgical Management of Calcaneal Malunion (Salvage Technique)
Despite optimal initial management, or in cases of neglected fractures, calcaneal malunion can occur, necessitating complex reconstructive salvage. Patients typically present with chronic lateral subtalar pain, posttraumatic arthrofibrosis, and severe lateral calcaneofibular impingement. When conservative measures fail, lateral decompression and realignment are required. The technique described by Braly, Bishop, and Tullos provides an excellent, highly technical framework for addressing these late complications.
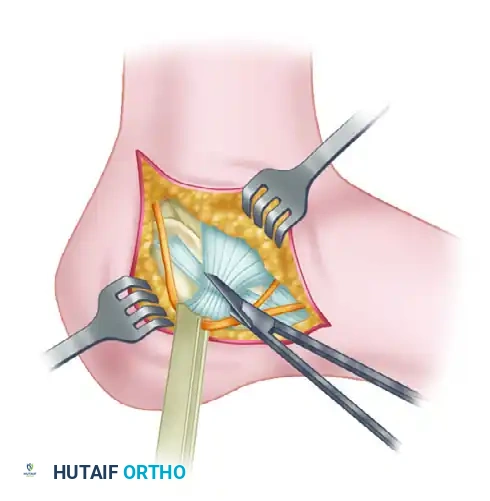
The procedure begins with an extensile lateral incision made just plantar to the course of the peroneal tendons to expose the lateral wall exostosis.

The sural nerve, which is frequently encased in dense, unyielding scar tissue from the initial trauma, must be meticulously identified and decompressed along its entire course in the surgical field.

Next, the inferior extensor retinaculum is incised, and a thorough peroneal tenolysis is performed to free the tendons from the lateral wall blowout.
The calcaneofibular ligament is then transected to fully expose the lateral wall of the calcaneus and the subtalar joint.
Following exposure, a lateral wall exostectomy is performed using an osteotome or sagittal saw, removing the impinging bone mass to decompress the subfibular space. If the subtalar joint is arthritic (Stephens and Saunders Type II or III), the articular cartilage is denuded, and an in situ or bone-block distraction subtalar arthrodesis is performed to restore calcaneal height and alleviate arthritic pain.
Complications, Incidence Rates, and Salvage Management
The management of calcaneal fractures, regardless of the surgical modality chosen, is associated with a notoriously high complication profile. Soft tissue edema and contusion are inherent aspects of high-energy axial loading injuries. Operating through such compromised soft tissue—especially in the lateral hindfoot, which possesses a tenuous blood supply and lacks a protective muscle layer—entails a significant risk of marginal wound necrosis. Historically, after a standard extensile L-shaped approach, wound complications developed in up to 25% of patients, with 21% requiring secondary surgical intervention such as deep debridement, negative pressure wound therapy, or free flap coverage. Although the percutaneous approach drastically reduces these risks (infection rates drop to 0% - 15%), minor wound dehiscence at the pin sites can still occur and requires vigilant postoperative monitoring.
Sural nerve and peroneal tendon injuries are critical complications that can lead to chronic, debilitating pain. The sural nerve courses posterior and inferior to the peroneal tendons and is highly vulnerable during percutaneous stab incisions and K-wire insertion. Iatrogenic injury can result in painful neuromas or regional numbness. Peroneal tendons are particularly vulnerable to subluxation, tenosynovitis, or direct laceration if the lateral calcaneal wall remains "blown out" or if drill sleeves are not utilized during percutaneous fixation. Limited periosteal elevation, blunt dissection to the bone, and the mandatory use of soft tissue protectors and drill sleeves during percutaneous fixation are absolute requirements to prevent these iatrogenic injuries.
Loss of reduction and hardware failure are mechanical complications often stemming from poor bone quality or non-compliance with weight-bearing restrictions. The calcaneus is composed primarily of cancellous bone, which provides poor purchase for screws, particularly in osteoporotic patients. If weight-bearing is initiated prematurely, the tuberosity fragment can displace proximally, resulting in a loss of Böhler's angle and a recurrence of the varus deformity. Accurate restoration of the proper valgus alignment of the tuberosity fragment is paramount; the human foot tolerates varus malrotation exceptionally poorly, leading to a rigid midfoot and severe lateral subfibular impingement.
Classification of Calcaneal Malunions
When malunion occurs, it is frequently classified using the Stephens and Saunders prognostic CT-based classification system, which guides surgical reconstruction:
- Type I: Lateral wall exostosis without subtalar arthrosis.

- Type II: Lateral wall exostosis with significant subtalar arthrosis.
- Type III: Lateral wall exostosis, subtalar arthrosis, and varus malunion of the calcaneal body.

Complications Summary Table
| Complication | Incidence Rate (Percutaneous) | Prevention & Salvage Management |
|---|---|---|
| Superficial Wound Infection | 2% - 5% | Prevention: Delay surgery until "wrinkle sign" appears; use |
